Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
PSVAC Training Session
January 4th, 2009
1
Agenda
Protocol Changes
Selective Spinal Immobilization
Telemetry Contact
RMA policy
Moshe Karp (30 minutes)
Moshe Karp (30 minutes)
(15 minutes)
(15 minutes)
***************** 15 Minute Break ******************
Albuterol
Epi Pen
New SCAM report
MOLST / DNR Orders
SAFE Centers
Matt Jachyra (30 minutes)
Matt Jachyra (40 minutes)
Will Tung (10 minutes)
Will Tung (15 minutes)
Will Tung (10 minutes)
Total time: 3 Hours, 30 Minutes
January 4th, 2008
PSVAC Training
2
2009 NYC REMSCO
Protocol Changes
Moshe Karp
3
BLS Changes - GOPs
There are just two changes to note within the General
Operating Procedures that apply to both BLS and ALS
providers:
– 10 Minute Rule Redefined
– Signs and Symptoms of Shock
January 4th, 2008
PSVAC Training
4
BLS Changes - GOPs
Page A.8
January 4th, 2008
PSVAC Training
5
BLS Changes - GOPs
The result of
this protocol can
be thought of in
terms of this
diagram
January 4th, 2008
PSVAC Training
6
BLS Changes - GOPs
Page A.11 – A.12
Because pale conjunctiva are a
sign of anemia, and not
necessarily shock, and
because it is a bad idea to ask
someone with suspected
decompensated shock to stand
just to that you can assess for
orthostatic vital signs, this
wording has been removed
from this section of the GOPs.
January 4th, 2008
PSVAC Training
7
BLS Protocols
The following BLS Protocols were changed:
– 400: WMD / Nerve Agent Exposure Protocol
– 404: Non-Traumatic Chest Pain
– 407: Asthma
– 414: Poisoning or Drug Overdose
– 432: Cold-Related Emergencies
– 421: Head and Spine Injuries
January 4th, 2008
PSVAC Training
8
BLS Protocols
Protocol 400 – WMD / Nerve Agent Protocol
So, particularly during the initial treatment, you can’t give one drug
(atropine) without giving the other (2-PAM). For this reason, the
portion of the protocol for the treatment of the yellow tag adult
patient has been changed – calling for two doses of each agent.
January 4th, 2008
PSVAC Training
9
BLS Protocols
Protocol 400 – WMD / Nerve Agent Protocol
The Mark I autoinjector kit that was previously
used is no longer available. Instead, the
company is now packaging both drugs in a
single autoinjector kit –Duodote.
January 4th, 2008
PSVAC Training
10
BLS Protocols
Protocol 404 – Non-Traumatic Chest Pain
– “Don't take VIAGRA if you take
nitrates, often prescribed for
chest pain, as this may cause a
sudden, unsafe drop in blood
pressure.”
– Though this warning is straight
out of the commercial, it also
applies to us.
January 4th, 2008
PSVAC Training
11
BLS Protocols
Protocol 404 – Non-Traumatic Chest Pain
There are a variety of drugs used to treat erectile dysfuntion:
– sildenafil (Viagra)
– tadalafil (Cialis)
– vardenafil (Levitra)
The new protocol requires that 72 hours have passed from
the time that a patient takes one of these medications until
you can safely administer nitroglycerin without OLMC contact.
January 4th, 2008
PSVAC Training
12
BLS Protocols
Protocol 404 – Non-Traumatic Chest Pain
One additional change is the age at which the
treatments in the protocol are indicated. Consistent with
the American Heart Association recommendations,
patients age 33 or older are to be considered “at risk”
for heart disease and treated as such. This protocol has
been altered to reflect this younger age.
January 4th, 2008
PSVAC Training
13
BLS Protocols
Protocol 407 – Asthma Wheezing
The first change to this protocol is right at the top. In
fact, it’s the title.
Now titled wheezing, this protocol no longer requires
that the patient have a history of asthma. Whether their
wheezing is due to asthma, COPD, smoke inhalation or
anything, you can treat their wheezing with this
protocol.
January 4th, 2008
PSVAC Training
14
BLS Protocols
Protocol 411 – Poisoning or Drug Overdose
Activated charcoal is not a harmless substance. It can make a
patient feel nauseated and, if aspirated, can cause a severe
inflammatory reaction in the lungs, leading to lung diseases.
Also because its benefit is even questionable for many
overdoses, it has been removed from the REMAC protocols.
January 4th, 2008
PSVAC Training
15
BLS Protocols
Protocol 432 – Cold-Related Emergencies
Severely hypothermic patients may have very slow
heart rates and/or hypotension. And so their pulse can
be very difficult to feel. The protocol now reflects that,
allowing “at least 30-45 seconds” to check for a carotid
pulse.
January 4th, 2008
PSVAC Training
16
Selective Spinal
Immobilization
Moshe Karp
17
NYS Spinal Update
Suspected
Spinal Injury
New York State
Department of Health
Bureau of Emergency Medical Services
January 4th, 2008
PSVAC Training
18
Selective Spinal
Immobilization
Protocol 421 – Head and Spine Injuries
After years of development, the statewide selective
spinal immobilization protocol is finally ready for
implementation. And, beginning January 1st, it will be
incorporated into the NYC REMAC protocols.
First, let’s address why this is such an important
change.
Q: Do you know how long it takes, just lying on a long
spine board, to develop the changes consistent with a
decubitus ulcer (“bedsore”, “decub”)?
A: Just one hour.
January 4th, 2008
PSVAC Training
19
Selective Spinal
Immobilization
Protocol 421 – Head and Spine Injuries
Spinal immobilization,
when unnecessary,
prolongs scene times,
causes undo pain for
the patient, and may
even worsen some
injuries.
The problem is
figuring out when it is
unnecessary.
January 4th, 2008
PSVAC Training
20
Selective Spinal
Immobilization
Protocol 421 – Head and Spine Injuries
Fortunately, this question has been asked and
answered. A large study (NEXUS) was performed to
identify criteria which could be used to determine who
does and does not need x-rays. And, in subsequent
studies, it was shown that these same criteria could be
used to determine who did and did not need spinal
immobilization.
January 4th, 2008
PSVAC Training
21
BLS Protocols
Selective Spinal
Immobilization
Patients meeting one or more of the following criteria
must be immobilized:
i. Altered mental status for any reason, including possible
intoxication due to drugs or alcohol.
ii. GCS <15
January 4th, 2008
PSVAC Training
23
Selective Spinal
Immobilization
iii. Complaint of, or inability of the
provider to assess for, neck and/or
spine pain or tenderness.
iv. Weakness, paralysis, tingling, or
numbness of the trunk or extremities
at any time since the injury.
v. Deformity of the spine not present
prior to the injury.
January 4th, 2008
PSVAC Training
24
Selective Spinal
Immobilization
vi. Distracting injury or circumstances, including anything
producing an unreliable physical exam or history.
January 4th, 2008
PSVAC Training
25
Selective Spinal
Immobilization
vii. High risk mechanism:
•
•
•
•
axial load such as diving or tackling,
high-speed motor vehicle accidents,
rollover accidents,
falls greater than
standing height.
vii. Provider concern for
potential spinal injury.
January 4th, 2008
PSVAC Training
26
Selective Spinal
Immobilization
NOTE: ONCE SPINAL IMMOBILIZATION HAS BEEN
INITIATED, IT MUST BE COMPLETED. SPINAL
IMMOBILIZATION MAY NOT BE REMOVED IN THE
PREHOSPITAL SETTING.
3. If necessary to initiate spinal immobilization, utilize the
Rapid Takedown technique ONLY if the patient is
standing.
January 4th, 2008
PSVAC Training
27
Selective Spinal
Immobilization
Protocol 421 – Head and Spine Injuries
Three final comments on this protocol:
1) Once immobilization is initiated (c-collar, KED,
backboard, etc), it may not be removed.
2) The protocol is not meant to identify patients for whom
immobilization is needed, only those for who it is not
needed.
3) If a patient is found to not need immobilization, all of
the criteria that led to this decision must be
documented in the PCR narrative.
January 4th, 2008
PSVAC Training
29
Telemetry Contact
30
Telemetry
What is telemetry?
– Greek: tele = remote, metron = measure
– Remote assessment and reporting
For us? OLMC
– On-Line Medical Control
– Physician (or Medical Control Officer operating under
Physician’s protocol) available 24/7
January 4th, 2008
PSVAC Training
31
When To Call
RMA
–
–
–
–
–
–
Patient lacks Decisional Capability
High Index of Suspicion
Unsafe Environment
Uncooperative Patient
Patient under 6 years old
Questions about DNR or MOLST
10-83
– Obvious signs of death but CPR in progress
– DNR or MOLST presented after CPR has been started
January 4th, 2008
PSVAC Training
32
When To Call
Medication Orders
– Epi-pen Administration
Transport
– Patient requests a hospital outside of “10 minute rule”
• Absolutely refuses transport to a closer hospital.
– Patient requests a specialty referral center
• Memorial Sloan-Kettering
– Patient requests hospital on diversion
January 4th, 2008
PSVAC Training
33
Who To Call
Methodist Medical Control
(718) 780-5555
January 4th, 2008
PSVAC Training
34
What To Say
Identify Yourself
Identify Your Patient
– {name}, {age}, {gender}
– “complaining of” or “called 911 for” {reason}
State Reason for calling OLMC
Patient Information: Past History, Meds, Allergies
Physical Assessment: Vital Signs, Skin CTC, etc.
Surroundings: good or bad environment
Friends / Family members present
January 4th, 2008
PSVAC Training
35
What To Document
Always inform your DO of any OLMC contact
ACR
– Physician name & ID, or MCO name & badge
– Translator name, address & phone
– Any OLMC-approved decisions
• RMA
• Alternate treatment or transport
• Approved cessation of resuscitation
January 4th, 2008
PSVAC Training
36
RMA Policy Changes
37
Definitions
Refusal of Medical Aid (RMA): A refusal of
emergency medical aid (treatment and/or transport) by
a patient or guardian on behalf of a patient.
Patient: Any individual for whom an ambulance has
been requested for treatment and/or transport.
Patient Contact: Any instance in which an emergency
medical provider has initiated an assessment or
treatment of a patient.
January 4th, 2008
PSVAC Training
38
Definitions
Decisional Capacity: An individual's ability to make an
informed decision concerning his or her medical
condition or treatment. Must understand:
– Nature of his medical condition
– Risks and consequences of refusal
– Treatment and transport alternatives
January 4th, 2008
PSVAC Training
39
Index of Suspicion
High Index of Suspicion: Possible acute medical,
traumatic, psychiatric, social condition with possible
life–threatening or life-altering outcome.
–
–
–
–
The Mechanism of Injury
Severity of Injury or Illness
Abnormal Vital Signs
Another person who expresses concern based on a change
in the PT’s condition
– Suicidal or Homicidal Behavior
– A healthcare provider indicates change in PT condition
Low Index of Suspicion: Everything else!
January 4th, 2008
PSVAC Training
40
Safe Environment
No immediate danger to PT health or safety
Adequate supportive resources (or assistance to obtain
them)
Suspicion of abuse? Automatically unsafe!
Undomiciled? Not automatically unsafe.
January 4th, 2008
PSVAC Training
41
Who Can RMA?
PT must be 18, or an Emancipated Minor:
General Operating Procedures page A.14
–
–
–
–
–
Is a mother
Is married
Has left home and is self supporting
Is enlisted in the Armed Forces
Is requesting treatment for STD, drug abuse, child abuse
Guardians may request an RMA for their charges.
– Parents (including grandparents)
– School Officials
January 4th, 2008
PSVAC Training
42
Who CANNOT RMA?
A Minor (under 18 years old) without a guardian
Parent/guardian for a child under 6 years old
An impaired patient (or guardian)
– Substance abuse
• Clinical signs of intoxication
– AMS due to:
• Trauma
• Psychiatric condition
• CNS dysfunction
• Medical condition
January 4th, 2008
PSVAC Training
43
Interagency Cooperation
PT in custody of law enforcement may RMA
– PT has Decisional Capability
– Must be PT’s decision (i.e. not coerced)
Suspect Coercion?
– Call OLMC or request a Duty Officer!
Patient may request specific destination
– Must be a 911 receiving facility
– Exception: Critical PT must go to nearest 911 facility
– Exception: Specialty Referral Centers (STEMI, etc)
January 4th, 2008
PSVAC Training
44
OLMC - (718) 780-5555
Required for:
–
–
–
–
–
PT under 6 w/ parent or guardian
PT with High Index of Suspicion
Medication administered
Unsafe environment
PT lacking Decisional Capability
–
–
–
–
Unaccompanied minor
PT cannot or refuses to provide information
Situations where a Health Care Proxy is requesting RMA
Questions/concerns with DNR or MOLST
Document all OLMC contact!
January 4th, 2008
PSVAC Training
45
Medication Administration
All providers (both EMTs and Paramedics) must contact OLMC
when a medication was administered to the patient by
EMS or others on scene.
Oxygen is only considered a medication if used for the
treatment of a patient condition that would be considered a
high index of suspicion (e.g., CHF, major trauma).
OLMC contact not required when “minor treatment”
(Bandages, gauze, icepacks, splints, immobilizers and oxygen)
is provided to patients who choose to RMA.
January 4th, 2008
PSVAC Training
46
Alternate Destinations
Patient may RMA due to destination
Follow the “10 minute rule”:
– General Operating Procedures page A.8
– You may transport a patient to their hospital of choice as long as
• Patient is Stable or Potentially Unstable
• Destination is less than an additional 10 minutes away
More than 10 minutes?
– CO or OLMC may approve up to an additional 20 minutes
– Usually requires specific need available only at that destination
Txp to Hospitals on Diversion need OLMC approval
Specialty Referral Centers
– Require OLMC approval to override
– May need to continue to SRC even is PT becomes unstable
January 4th, 2008
PSVAC Training
47
What Do You Do?
ALWAYS recommend TXP!
– PT may have right of refusal, but an MD can provide peace
of mind.
– Never encourage an RMA!
Full Assessment
– Including two sets of vital signs
– Required for every RMA
Determine Index of Suspicion
Determine Safe Environment
Evaluate Decisional Capacity
January 4th, 2008
PSVAC Training
48
What Do You Do?
Request Duty Officer to the scene
– Always the first option
Contact OLMC
Request Police Department
Document RMA in PCR if approved
January 4th, 2008
PSVAC Training
49
PCR
RMA Disposition Code: 005
“Trinity”
– PT aware of medical condition
– PT advised of risks & consequences
– PT advised of alternate destinations & continuance of 911 care
Sign & Witness!
OLMC Contact?
– Document physician name & ID
Translator used?
– Document name, address and phone of translator
Radio Codes
– 10-93: Patient with Decisional Capacity
– 10-93A: Patient without Decisional Capacity; OLMC approval
January 4th, 2008
PSVAC Training
50
RMA Flowchart
January 4th, 2008
PSVAC Training
51
Question to Ask
1. Who called for the ambulance? If not the patient, who and why did
they call?
2. Is the patient capable of communicating with the On-Line Medical
Control Physician? If not, why not?
3. Why does the patient not want to go to the hospital? What would
change the patient's mind (e.g., going to a specific hospital)?
4. What are the signs and symptoms of injury or illness (physical or
mental)?
5. What is the patient’s usual health status?
6. Does the patient's chronic/acute medical or psychiatric condition
(e.g., diabetes, mental retardation, Alzheimers) lead you to suspect
that the patient may not have the appropriate decisional capacity to
refuse treatment and/or transport?
January 4th, 2008
PSVAC Training
52
Question to Ask
7. What has changed since the initial call for the ambulance, if
anything?
8. Was the patient given all alternatives (e.g., choice of hospitals,
seeing private physician)?
9. Does the patient appear to understand the alternatives?
10. Has the patient taken any medications (on their own or provided
by EMS) since the onset of their current complaint?
11. Does the patient understand the consequences of their injury or
condition and of refusing treatment and or transport to the hospital?
(This should include the possibility of death, if the circumstances
indicate that it is indeed possible.)
12. Does the patient clearly understand that EMS is still available by
calling 911, should the patient desire treatment or transportation to a
hospital?
13. Will someone be able to stay with the patient if the RMA is
granted by the OLMC physician?
January 4th, 2008
PSVAC Training
53
Sample Case 1
Two teenage boys (both 18) are involved in a carversus-telephone-pole MVA. Both airbags are deployed
and the patients must be extracted. They say they have
no neck or back pain, but the driver has cuts on his
head and says he “feels a little woozy”. He cannot
correctly state today’s date. Neither want to go to the
hospital, because their “parents will get angry”.
–
–
–
–
Do you
What if
What if
What if
January 4th, 2008
contact OLMC? Why or why not?
one was 17?
the passenger was the father of the driver?
there was only minor damage and no head injury?
PSVAC Training
54
Sample Case 2
911 call to an assisted living facility for a suspected
CVA. The PT presents with mild slurred speech, no facial
droop, partial weakness and drift in the left arm and
leg, strong vitals. The PT has a DNR on file (presented
to you by the facility). The caregiver tells you the PT
does not want to go to the hospital.
–
–
–
–
Do you write up the RMA? Why or why not?
Do you contact OLMC? Why or why not?
What if there was no signs of stroke?
What if the PT had bedsores, and there is fecal matter on
the floor of the PT room?
January 4th, 2008
PSVAC Training
55
B R E A K
15 Minutes
56
Albuterol Administration
Matt Jachyra
57
Albuterol
Albuterol is a bronchodilator that relaxes muscles in the
airways and increases air flow to the lungs. Albuterol is
used to treat or prevent bronchospasm in people with
reversible obstructive airway disease such as COPD,
bronchitis and asthma. Albuterol is also used to prevent
exercise-induced bronchospasm.
January 4th, 2008
PSVAC Training
58
Albuterol
January 4th, 2008
PSVAC Training
59
Albuterol
407 Wheezing
For patients over one (1) year of age who are
experiencing asthma exacerbation or wheezing.
1. Assess the airway
2. Administer oxygen
3. Monitor breathing
NOTE: IF PATIENT EXHIBITS SIGNS OF IMMINENT
RESPIRATORY FAILURE, REFER TO PROTOCOL #401
– ADULT RESPIRATORY DISTRESS/FAILURE OR
#450 – PEDIATRIC RESPIRATORY
DISTRESS/FAILURE.
January 4th, 2008
PSVAC Training
60
Albuterol
4. Do not permit physical activity
5. Place the patient in a Fowler’s or Semi-Fowler’s position
6. Assess the following prior to administration of the first
nebulized treatment:
•
•
•
•
Vital signs
Patient’s ability to speak in complete sentences
Accessory muscle use
Wheezing
January 4th, 2008
PSVAC Training
61
Albuterol
7. Administer Albuterol Sulfate 0.083%, one (1) unit dose
or 3 cc via nebulizer at a flow rate that will deliver the
solution over 5 minutes to 15 minutes. Do not delay
transport to complete medication administration.
8. Begin transport.
NOTE: FOR PATIENTS IN SEVERE RESPIRATORY
DISTRESS, CALL FOR ADVANCED LIFE SUPPORT
ASSISTANCE, DO NOT DELAY TRANSPORT.
9. If symptoms persist, Albuterol Sulfate 0.083% may be
repeated twice for a total of three (3) doses, with the
third occurring during transport.
10. Upon completion of patient treatment or transfer of
patient care to an ALS Provider or a 911 Receiving
Hospital, reassess the patient. See Step # 6.
January 4th, 2008
PSVAC Training
62
Albuterol
MEDICAL CONTROL MUST BE CONTACTED FOR
ANY PATIENT REFUSING MEDICAL ASSISTANCE
OR TRANSPORT.
January 4th, 2008
PSVAC Training
63
Albuterol
So what is Albuterol and how do I eat it?
January 4th, 2008
PSVAC Training
64
Albuterol
Medication name
Generic - Albuterol
1. Actions - Beta agonist bronchodilators
Which in plain English means that it dilates bronchioles
reducing airway resistance.
2. Side effects:
-Increased pulse rate
-Tremors
-Nervousness
-Nausea
January 4th, 2008
PSVAC Training
65
Albuterol
3. Supplied in 3mm plastic vial in 0.083% concentration.
Like with every medication prior to administration
please check for expiration, cloudiness of the liquid,
proper name, intact medication container and if there is
an indication for drug administration. Document
properly not only when and how medication was given
but also patient response.
OK! OK! OK! But how do I administer it to
my patient??
January 4th, 2008
PSVAC Training
66
Albuterol
Nebulizer is a device used to administer medication to
people in the form of a mist inhaled into the lungs.
There are different types of nebulizer, although the most
common are the jet nebulizers, which are also called
"atomizers". Jet nebulizers are connected by tubing to a
compressed air source that causes air or oxygen to blast
at high velocity through a liquid medicine to turn it into
an aerosol, which is then inhaled by the patient.
Nebulizers accept their medicine in the form of a liquid
solution, which is often loaded into the device upon use.
January 4th, 2008
PSVAC Training
67
Albuterol
1.
2.
3.
4.
5.
Mouthpiece
Nebulizer t-piece
Nebulizer cap
Nebulizer chamber
Nebulizer air-inlet
connector
6. Nebulizer baffle
7. Tubing
January 4th, 2008
PSVAC Training
68
Albuterol
Assemble clean nebulizer
parts by placing baffle down
in nebulizer chamber. Holding
chamber stationary, screw on
nebulizer cap. Add prescribed
medication through the
opening on cap using a
medicine dropper or
premeasured dose container.
January 4th, 2008
PSVAC Training
69
Albuterol
Assemble mouthpiece and
T-piece and insert into the top
of the nebulizer cap.
January 4th, 2008
PSVAC Training
70
Albuetrol
Attach tubing to nebulizer
air-inlet connector. Set the
LPM flow between 4-6 to
deliver medication over 5-15
minutes.
January 4th, 2008
PSVAC Training
71
Albuterol
Begin treatment by advising the
patient to place the mouthpiece
between their teeth. With
mouth closed, pt should inhale
deeply and slowly through
mouth as aerosol begins to flow
then exhale slowly through the
mouthpiece.
January 4th, 2008
PSVAC Training
72
Albuterol
So how bad your patient can get?
- Previous intubations
- Prolonged hospitalizations
- Family history
- Events leading to the episode
- Medications compliance
- Inhaled steroids use
- Severity of current episode
- Patients lifestyle
- Combination of all of the above
January 4th, 2008
PSVAC Training
73
Epinepherine Autoinjector
Matt Jachyra
74
Epinephrine Auto Injector
Anaphylaxis, or anaphylactic shock, is an allergic
reaction that can be fatal within minutes, either through
swelling that shuts off airways or through a dramatic
drop in blood pressure.
Anaphylaxis occurs in individuals when they are
exposed to an allergen to which they are allergic. An
allergen is almost always a protein that is treated by the
immune system as a foreign substance. Contact with, or
ingestion of this allergen will set off a chain reaction in a
person's immune system that may lead to swelling of
the airways, loss of blood pressure, and loss of
consciousness, resulting in anaphylactic shock.
January 4th, 2008
PSVAC Training
75
Epinephrine Auto Injector
Common causes of anaphylaxis include:
Food - Peanuts, tree nuts (walnuts, cashews, etc.),
shellfish, fish, milk, and eggs commonly cause
anaphylactic reactions.
Medication - Anaphylactic reactions to medication will
typically occur within an hour after taking the drug,
however reactions may occur several hours later.
Insect stings - The symptoms of anaphylactic reactions
to insect stings usually occur within minutes of the
sting.
Latex - Approximately 10 to 17 percent of those
employed in the health care occupations have this
allergy.
January 4th, 2008
PSVAC Training
76
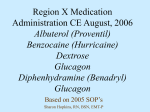
Epinephrine Auto Injector
Signs and Symptoms of an Allergic Reaction:
-Hives
-Swelling of the throat, lips, tongue, or around the eyes
-Difficulty breathing or swallowing
-Generalized flushing, itching, or redness of the skin
-Abdominal cramps, nausea, vomiting, or diarrhea
-Increased heart rate
-Sudden decrease in blood pressure (and accompanying
paleness)
January 4th, 2008
PSVAC Training
77
Epinephrine Auto Injector
Example of Hives
January 4th, 2008
PSVAC Training
78
Epinephrine Auto Injector
It is impossible to predict the severity of future
anaphylactic reactions in any particular person. There is
no set pattern, but the severity of an allergic reaction is
thought to depend on:
-The amount of allergen to which a patient is exposed
-The individual's degree of hypersensitivity to the
allergen
-Time elapsed from exposure until your arrvial
January 4th, 2008
PSVAC Training
79
Epinephrine Auto Injector
So what can we do???
January 4th, 2008
PSVAC Training
80
Epinephrine Auto Injector
1. Perform initial assessment (your ABC).
2. Perform a focused history and physical exam:
-History of allergies
-What was the patient exposed to
-How were they exposed
-What effects
-Time of onset
-Progression
-Interventions
January 4th, 2008
PSVAC Training
81
Epinephrine Auto Injector
3. Assess baseline vital signs and SAMPLE history.
4. Administer oxygen if not already done in the initial
assessment.
5. Determine if patient has prescribed preloaded
epinephrine available. Facilitate administration of
preloaded epinephrine.
6. Record and reassess in two minutes.
7. Record reassessment findings.
NOW THIS IS WHERE IT GETS TRICKY!!!
January 4th, 2008
PSVAC Training
82
Epinephrine Auto Injector
Patient has contact with substance that causes allergic
reaction without signs of respiratory distress or
shock/hypoperfusion (anaphylactic shock):
1. Continue with focused assessment.
2. Patient is not wheezing or without signs of
respiratory distress or hypotension should not receive
epinephrine.
3. Transport, reassess, reevaluate and closely monitor.
January 4th, 2008
PSVAC Training
83
Epinephrine Auto Injector
Patient has contact with substance that causes allergic
reaction with signs of respiratory distress or
shock/hypoperfusion (anaphylactic shock):
Protocol 410 – Anaphylactic Reaction
January 4th, 2008
PSVAC Training
84
Epinephrine Auto Injector
ANAPHYLAXIS CAN BE A POTENTIALLY LIFE
THREATENING SITUATION MOST OFTEN ASSOCIATED
WITH A HISTORY OF EXPOSURE TO AN INCITING
AGENT/ALLERGEN (BEE STING OR OTHER INSECT
VENOM, MEDICATIONS/DRUGS, OR FOODS SUCH AS
PEANUTS, SEAFOOD, ETC.). THE PRESENCE OF
RESPIRATORY DISTRESS (UPPER AIRWAY
OBSTRUCTION [STRIDOR], SEVERE BRONCHOSPASM
[WHEEZING]) AND/OR CARDIOVASCULAR
COLLAPSE/HYPOTENSIVE SHOCK CHARACTERIZE THE
CLINICAL FINDINGS THAT AUTHORIZE AND REQUIRE
TREATMENT ACCORDING TO THIS PROTOCOL. THIS
PROTOCOL APPLIES TO PATIENTS 9 YEARS OF AGE OR
OLDER, OR PATIENTS WEIGHING MORE THAN 30 KG
(66 LBS).
January 4th, 2008
PSVAC Training
85
Epinephrine Auto Injector
1. Determine that the patient’s history includes a history of
anaphylaxis, severe allergic reaction and/or recent exposure
to an allergen or inciting agent.
NOTE: REQUEST ALS ASSISTANCE, IF AVAILALE. DO
NOT DELAY TRANSPORT TO THE HOSPITAL
2. Administer high concentration oxygen.
3. Assess the cardiac and respiratory status of the patient.
a. If both the cardiac and respiratory status of the patient are
normal, initiate transport.
b. If either the cardiac or respiratory status of the patient is
abnormal, proceed as follows:
January 4th, 2008
PSVAC Training
86
Epinephrine Auto Injector
i. If the patient is having severe respiratory distress or
shock and has been prescribed an Epinephrine autoinjector, assist the patient in administering the
Epinephrine (0.3 mg via an auto-injector). If the
patient’s auto-injector is not available or expired, and
the EMS agency carries an Epinephrine auto-injector,
administer the Epinephrine (0.3 mg via an autoinjector) as authorized by the agency’s Medical Director.
January 4th, 2008
PSVAC Training
87
Epinephrine Auto Injector
ii. If the patient has not been prescribed an Epinephrine
auto-injector, begin transport and contact On-Line
Medical Control for authorization to administer 0.3 mg
Epinephrine via an auto-injector, if available.
NOTE: IN THE EVENT THAT YOU ARE UNABLE TO
MAKE CONTACT WITH ON-LINE MEDICAL CONTROL
(RADIO FAILURE, NO COMMUNICATIONS) AND THE
PATIENT IS UNDER 35 YEARS OF AGE, YOU MAY
ADMINISTER 0.3 mg EPINEPHRINE (ONE DOSE
ONLY) VIA AN AUTO-INJECTOR IF INDICATED. THE
INCIDENT MUST BE REPORTED TO ON-LINE MEDICAL
CONTROL AND YOUR AGENCY’S MEDICAL DIRECTOR
AS SOON AS POSSIBLE
January 4th, 2008
PSVAC Training
88
Epinephrine Auto Injector
iii. Contact On-Line Medical Control for authorization to
administer a second administration of 0.3 mg
Epinephrine via an auto-injector, if needed.
iv. Refer immediately to the REMAC Prehospital
Treatment Protocol for Respiratory Distress/Failure
(#401), Obstructed Airway (#402), or Shock (#415) as
appropriate.
4. If cardiac arrest occurs, refer immediately to the REMAC
Prehospital Treatment Protocol for Non-Traumatic
Cardiac Arrest (#403).
January 4th, 2008
PSVAC Training
89
Epinephrine Auto Injector
So what is that magical thing
you call Epinephrine and what
can I do with it?
January 4th, 2008
PSVAC Training
90
Epinephrine Auto Injector
1. Medication name:
Generic – Epinephrine
Trade - Adrenalin
2. Indications - must meet all of the following three criteria
(1) Emergency medical care for the treatment of the patient
exhibiting the assessment findings of an allergic reaction IE.
Respiratory distress and/or wheezing
(2) Medication is prescribed for this patient by a physician
(3) Medical direction authorizes use for this patient
3. Contraindications - no contraindications when used in a life
threatening situation
4. Medication form - liquid administered via an automatically
injectable needle and syringe system
January 4th, 2008
PSVAC Training
91
Epinephrine Auto Injector
5. Dosage
(1) Adult - one adult auto-injector (0.3 mg)
(2) Pediatrics - one pediatrics auto-injector (0.15 mg)
7. Actions
(1) Dilates the bronchiole
(2) Constricts blood vessels
8. Side effects
(1) Increases heart rate
(2) Pallor
(3) Dizziness, excitability, anxiousness
(4) Chest pain
(5) Headache
(6) Nausea
(7) Vomiting
January 4th, 2008
PSVAC Training
92
Epinephrine Auto Injector
OK now I know what
Epinephrine is and what it does
so how do I give it to my
patient?
January 4th, 2008
PSVAC Training
93
Epinephrine Auto Injector
Administration
(1) Obtain order from medical direction either on-line or off-line
(2) Obtain patient's prescribed auto injector. Ensure:
(a) Prescription is written for the patient experiencing
allergic reactions
(b) Medication is not discolored, expired, vial is intact
(3) Remove safety cap from the auto-injector
(4) Place tip of auto-injector against the patient's thigh
(a) Lateral portion of the thigh
(b) Midway between the waist and the knee
(5) Push the injector firmly against the thigh to activate the
injector
(6) Hold the injector in place until the medication is injected
(7) Record activity and time
(8) Dispose of injector in biohazard container
January 4th, 2008
PSVAC Training
94
Epinephrine Auto Injector
To prepare the EpiPen for use, grasp the auto-injector
with the hand (forming a fist around the unit) with the
black tip facing downward. Immediately before use,
remove the gray activation cap with the other hand,
being careful not to touch the black tip, where the
needle is located, at any time.
January 4th, 2008
PSVAC Training
95
Epinephrine Auto Injector
January 4th, 2008
PSVAC Training
96
Epinephrine Auto Injector
After uncapping the auto-injector, place the black tip
near the fleshy outer portion of the thigh. Instruct the
patient that it is not necessary to remove any clothing;
the EpiPen auto-injector is designed to work effectively
through clothing. Reminded: do not to touch the black
tip of the auto-injector at any time.
Make a note of the site, which side (R/L) and look for
effects of the injection.
January 4th, 2008
PSVAC Training
97
Epinephrine Auto Injector
January 4th, 2008
PSVAC Training
98
Epinephrine Auto Injector
With a quick motion, swing out and jab firmly into the
outer thigh, so that the injector is at a 90 degree angle
to the thigh. Hold firmly in the thigh for several
seconds. During this time, a spring-activated
mechanism is released, and a dose of epinephrine is
administered. Remove the unit and massage the
injection site for an additional few seconds.
Once administration is complete, you should check the
black tip of the auto-injector. If the needle is exposed, a
dose of epinephrine was injected. If not, the above
steps should be repeated. Most of the liquid (90%)
stays in the auto-injector after the dose is administered
and cannot be reused.
Dispose used unit in the biohazard sharps container.
January 4th, 2008
PSVAC Training
99
Epinephrine Auto Injector
January 4th, 2008
PSVAC Training
100
Epinephrine Auto Injector
Medical Control Conversation
Telemetry: Hello this is Telemetry.
PS1:Hi this is Paramedic Jachyra with 93K Park Slope Volunteer
Ambulance Corp calling for meds order secondary to
anaphylaxis/severe allergic reaction.
Telemetry: Stand by for Dr. Silverman 80297
PS1: Good morning doctor this is Paramedic Jachyra. I have a 36 yo
female AO3 who after eating peanuts by mistake developed severe
allergic reaction. Pt is allergic to nuts and last time she had such
reaction she was admitted to the hospital and intubated. Pt speaks in
2-3 word dyspnea and I can see severe accessory muscle use. Vitals
are as follow 90/40, 120 heart rate and respirations are 24 labored, I
hear bilateral wheezing on expirations, skin is red and pt is covered in
hives. Pt has no medical problems and takes over the counter
benadryl. So far I’ve trated this patient for shock, gave them oxygen,
requested ALS and I’m preparing for transport. I would like to
administer Epi Pen Auto-Injector.
January 4th, 2008
PSVAC Training
101
Epinephrine Auto Injector
Telemetry: Sure go ahead and administer the Epinephrine and expedite
transport to nearest facility.
PS1: Repeating orders: I will administer one Auto Injector Epi Pen.
Thank you doctor.
Telemetry: Ten four goodbye.
Be ready to answer additional questions about patient medical history as
well as questions about history of present illness.
January 4th, 2008
PSVAC Training
102
Epinephrine Auto Injector
Now what about pediatrics?
January 4th, 2008
PSVAC Training
103
Epinephrine Auto Injector
ANAPHYLAXIS CAN BE A POTENTIALLY LIFE THREATENING SITUATION
MOST OFTEN ASSOCIATED WITH A HISTORY OF EXPOSURE TO AN
INCITING AGENT/ALLERGEN (BEE STING OR OTHER INSECT VENOM,
MEDICATIONS/DRUGS, OR FOODS SUCH AS PEANUTS, SEAFOOD, ETC.).
THE PRESENCE OF RESPIRATORY DISTRESS (UPPER AIRWAY
OBSTRUCTION [STRIDOR], LOWER AIRWAY DISEASE/SEVERE
BRONCHOSPASM [WHEEZING]) AND/OR CARDIOVASCULAR
COLLAPSE/HYPOTENSIVE SHOCK CHARACTERIZE THE CLINICAL
FINDINGS THAT AUTHORIZE AND REQUIRE TREATMENT ACCORDING TO
THIS PROTOCOL. THIS PROTOCOL APPLIES TO PATIENTS UNDER 9
YEARS OLD OR PATIENTS WEIGHING LESS THAN 30 KG (66 LBS). FOR
PATIENTS 9 YEARS OF AGE OR OLDER, OR OVER 30 KG (66 LBS) REFER
TO THE ADULT ANAPHYLAXIS PROTOCOL (#410).
January 4th, 2008
PSVAC Training
104
Epinephrine Auto Injector
1. Determine that the patient’s history includes a history of
anaphylaxis, severe allergic reaction and/or recent exposure
to an allergen or inciting agent.
NOTE: DO NOT DELAY TRANSPORT TO THE HOSPITAL
2. Administer high concentration oxygen.
3. Assess the cardiac and respiratory status of the patient.
a. If both the cardiac and respiratory status of the patient
are normal, initiate transport.
January 4th, 2008
PSVAC Training
105
Epinephrine Auto Injector
b. If either the cardiac or respiratory status of the patient
is abnormal, proceed as follows:
– i. If the patient is having severe respiratory distress or
shock and has been prescribed a pediatric (0.15 mg)
Epinephrine auto-injector, assist the patient in
administering the Epinephrine. If the patient’s autoinjector is not available or expired, and the EMS agency
carries a pediatric (0.15 mg) Epinephrine auto-injector,
administer the Epinephrine as authorized by the agency’s
Medical Director.
– ii. If the patient has not been prescribed a pediatric (0.15
mg) Epinephrine auto-injector, begin transport and contact
On-Line Medical Control for authorization to administer a
pediatric (0.15 mg) Epinephrine auto-injector, if available.
January 4th, 2008
PSVAC Training
106
Epinephrine Auto Injector
NOTE: IN THE EVENT THAT YOU ARE UNABLE TO MAKE
CONTACT WITH ON-LINE MEDICAL CONTROL (RADIO
FAILURE, NO COMMUNICATIONS), YOU MAY
ADMINISTER THE EPINEPHRINE AUTOINJECTOR (0.15
MG) IF INDICATED. THE INCIDENT MUST BE REPORTED
TO ON-LINE MEDICAL CONTROL AND YOUR AGENCY’S
MEDICAL DIRECTOR AS SOON AS POSSIBLE
iii. Contact On-Line Medical Control for authorization to
administer a second administration of a pediatric (0.15 mg)
Epinephrine auto-injector, if needed.
iv. Refer immediately to the REMAC Prehospital Treatment
Protocol for Respiratory Distress/Failure (#450), Obstructed
Airway (#451), or Shock (#458) as appropriate.
4. If cardiac arrest occurs, refer immediately to the REMAC
Prehospital Treatment Protocol for Non-Traumatic Cardiac
Arrest (#453)
January 4th, 2008
PSVAC Training
107
Epinephrine Auto Injector
EpiPen in Adult and Ped configuration.
January 4th, 2008
PSVAC Training
108
Epinephrine Auto Injector
Remember that the best source of information about
what’s going on with your patient at present time is
your patient himself. Also look for allergy alert tags,
bracelets and necklaces.
January 4th, 2008
PSVAC Training
109
New SCAM Report
Will Tung
110
Child Abuse and Neglect
Protocol: General Operating Procedures page A.13
Definition of abuse:
– improper or excessive action so as to injure or cause harm
Definition of neglect:
– giving insufficient attention or respect to someone who has
a claim to that attention
You must be able to recognize the problem
January 4th, 2008
PSVAC Training
111
Signs and Symptoms of
Abuse
Multiple bruises in various stages of healing
Injury inconsistent with mechanism described
Repeated calls to the same address
Fresh burns
Parents seem inappropriately unconcerned
Conflicting stories
Fear on the part of the child to discuss how the injury occurred
Shaken Baby Syndrome
January 4th, 2008
PSVAC Training
112
Signs and Symptoms of
Neglect
Lack of adult supervision
Malnourished appearance
Unsafe living environment
Untreated chronic illness;
– e.g., asthmatic with no medications
January 4th, 2008
PSVAC Training
113
What do you do?
Provide appropriate care
– Call PD if needed
Do not accuse in the field
– Accusation and confrontation delays transport
Report suspicions to the hospital attending physician
Reporting:
– Call NYS Child Abuse/Maltreatment Register
– File a SCAM Report
What you see and what you hear - NOT what you think
January 4th, 2008
PSVAC Training
114
SCAM Report
You MUST report suspected child abuse or
maltreatment you identify while performing your duties
– Only reasonable cause needed (no need for proof)
Reports to be made:
– immediately by phone
– within 48 hours in writing
Report must be made even if:
– only partial information is available
– there is no reason to suspect parental involvement
January 4th, 2008
PSVAC Training
115
PSVAC Procedures
Immediately notify an officer
Try and get as much info as you can while on the call or
in the hospital, but don’t delay patient care
Complete PCR and SCAM report while at hospital, prior
to coming available
Return to base and call NYS Child Abuse/Maltreatment
Register: 1-800-635-1522 (during tour)
Send or Fax SCAM Report (within 48 hours)
January 4th, 2008
PSVAC Training
116
Failure to Report
We are Mandated Reporters
If you fail to report, you will be:
– Guilty of Class A misdemeanor
– Civilly liable for the damages proximately caused by such
failure
When unsure… REPORT IT.
January 4th, 2008
PSVAC Training
117
New SCAM Report
Sample Case 1
You respond to a baseball field. The coach called when
one of his players had trouble catching his breath. The
child’s parents were also called, and they arrive at the
ball field just after you. You learn that the child has a
preexisting asthmatic condition. The parents report
that the child sees a specialist regularly. At the scene,
the parents administer the child’s inhaler and his
breathing becomes less labored.
Any need to report this? Why?
January 4th, 2008
PSVAC Training
119
Sample Case 3
You arrive at the home of a grandmother and her 4 year
old grandchild. The child appears to have multiple
injuries. The grandmother reports that she is
babysitting while the child’s mother is at work. The
child was difficult to wake from her afternoon nap. The
grandmother is concerned about the child. While
onscene, the child’s mother arrives to pick up the child.
You ask about the child’s injuries and mom says the
child is clumsy and frequently falls from her bicycle.
Any need to report this? Why?
January 4th, 2008
PSVAC Training
120
Sample Case 2
You respond to a call and find a woman with an injury to
her left eye. You see two small children in the room
with the woman. The woman reports that she was
struck by her drunk boyfriend while the children were
cowering behind her. She also states that he told her
he would kill her and the two children if she told
anyone.
Any need to report this? Why?
January 4th, 2008
PSVAC Training
121
Fill Out a SCAM Report
Use the last scenario:
– Mom: Jane Doe, 32 y/o, Black, Hispanic, Spanish Speaking
– Boyfriend: John Doe, 30 y/o, Asian, English Speaking
– Child 1: Junior Doe, 10 y/o, White, Hispanic, Sign Language
– Child 2: Baby Doe, 4 y/o, Unknown Race, English Speaking
January 4th, 2008
PSVAC Training
122
MOLST / DNR Orders
Will Tung
123
What do we recognize?
Protocols: Appendix C
What we recognize:
– NY State “Out of Hospital” DNR Form
• Home, hospice, clinic, etc.
– DNR Bracelet
– Now: MOLST
What we don’t recognize:
– Living Wills
– Health Care Proxys
– Facility DNRs
• Recognize only for txp from hospital/nursing home
January 4th, 2008
PSVAC Training
124
NYS “Out of Hospital”
DNR Form
When is it valid?
When presented to EMT
Good faith attempt to identify patient
– A witness who can reliably identify the patient is useful
Out of hospital DNRs do not expire
DNR form or bracelet should be taken with the patient
January 4th, 2008
PSVAC Training
126
When is it not valid?
If DNR order was revoked or cancelled
The patient states that they wish resuscitative measures
A confrontational situation with family
A physician directs that the order be disregarded
January 4th, 2008
PSVAC Training
127
What do you treat?
If in cardiac or respiratory arrest:
– NO chest compressions, ventilation, defibrillation.
If not in cardiac or respiratory arrest:
– full treatment including ventilations
If no DNR is presented:
– Start CPR
– If DNR is presented after CPR has started, call telemetry
For unusual situations or questions
– Contact officer or telemetry
January 4th, 2008
PSVAC Training
128
Documentation
Attach copy of DNR to Patient Care Report
– Note on the PCR that a DNR was present
– Include: physician name, date signed and other pertinent
info
DNR Form should accompany the patient
Leave DOAs onscene
January 4th, 2008
PSVAC Training
129
MOLST
Medical Orders for Life-Sustaining Treatment
Completed with the patient or patient’s designee and
physician
Provide Explicit direction for CPR, mechanical ventilation
and other life sustaining treatments
January 4th, 2008
PSVAC Training
130
MOLST Form
When is it important?
Most situations: Form will just need to go with the
patient to the hospital or back home
– Look for the form on the refrigerator, the back of the
bedroom door or in the patient’s chart
No breathing and no pulse:
– Locate form
– Determine if it’s valid
– Follow directions: DNR or CPR
Critically ill:
– Sections on “Life Sustaining Treatments” may apply
January 4th, 2008
PSVAC Training
132
MOLST Characteristics
Original is “MOLST Pink” and printed on heavy stock
– Copies and Faxes Accepted
Do Not Resuscitate or Full CPR is on page 1
Other Care decisions are documented on page 2
An “Out of Hospital DNR Form” is still valid if found
– Use form with latest date
January 4th, 2008
PSVAC Training
133
MOLST Video
Play MOLST Video
(7 minutes)
January 4th, 2008
PSVAC Training
134
Sexual Assault Forensic
Examiner (SAFE) Centers
Will Tung
135
SAFE Centers
Sexual Assault is any sexual contact without consent
– Not just Rape
Sexual assault can be perpetrated by anyone, to
anyone, and anywhere.
Your patient may feel overwhelmed, angry,
embarrassed, afraid, numb, in a state of disbelief, or
have a sense of profound loss
January 4th, 2008
PSVAC Training
136
SAFE Centers
Assume non-authoritative, non-controlling attitude.
Allow your patient to begin to regain control of her/his
body:
– Ask permission to take a history and examine your
patient; ask permission to touch your patient
– Explain all parts of the exam and all procedures
– Respond to your patient’s wish to talk or not to talk
– Maintain your patient’s modesty and privacy
January 4th, 2008
PSVAC Training
137
SAFE Centers
Tell the patient that you are there to help
– “I am sorry for what happened to you.”
– “No one deserves to be treated as you were.”
– “Nothing that you could have done or said could possibly
justify what has happened to you.”
Use a same sex EMT for care whenever possible
Be patient; move and act slowly
January 4th, 2008
PSVAC Training
138
SAFE Centers
Evidence Collection
– If your patient has changed clothing or underwear since
the assault, ask her/him to bring this with them in a paper
bag (plastic allows degradation of evidence).
– If possible, ask her/him to bring a change of clothing
– Discourage your patient from bathing, voiding, or douching
as it will destroy evidence
– If the patient must void, ask them to use a container and
bring the urine with them to the hospital
– Do not allow your patient to drink, brush their teeth, or
smoke
– Do not clean wounds unless necessary
January 4th, 2008
PSVAC Training
139
SAFE Centers
Document carefully
– Use a diagram to show the location of wounds
– Keep the written history brief; let the SAFE examiner do
the majority of the documentation
– The slightest misstatement (such as saying “boyfriend”
rather than “husband”) could cause significant difficulties
at a trial and hurt the legal case
– Use patient’s statements, if possible
– NYPD and the SAFE examiner will ask the difficult
questions and document them well
January 4th, 2008
PSVAC Training
140
SAFE Centers
Upon Arrival at the ED:
– Make certain that the triage nurse understands that your
patient is a states she was sexually assaulted
– Be sure to inform staff if weapons and/or other “evidence”
has accompanied the patient to the ED (condom, tampon,
clothing)
– You may be asked to take your patient to the “SAFE Room”
January 4th, 2008
PSVAC Training
141
SAFE Centers
SAFE Programs allow expert medical management of victims of
sexual assault and expert forensic examinations for evidence
collection and expert testimony.
The 24-hour availability of trained sexual assault examiners,
specialized equipment to detect and document injury, dedicated
examination and shower rooms, trained advocates and full-time
social workers for follow-up counseling services and emotional
support allow for seamless integration of all medical, forensic,
and counseling care.
January 4th, 2008
PSVAC Training
142
SAFE Centers
1. Upon identification of a stable adult (12 years or older) sexual
assault patient (based on patient self-report or
bystander/police report):
a. Provide appropriate treatment for any injuries/illnesses in
accordance with REMAC Prehospital Treatment Protocols. Physical
examination to identify or confirm sexual abuse shall not be
performed by EMS healthcare providers.
b. Advise the patient that transportation to an emergency
department with a SAFE Program is available and encourage the
patient to accept transport to the nearest SAFE facility.
c. If a stable patient accepts transport to a SAFE facility, transport
the patient to the nearest (or closest) SAFE hospital.
January 4th, 2008
PSVAC Training
143
Our Closest
SAFE Centers
BROOKLYN:
– Kings County Hospital Center (H 48)
– Coney Island Hospital (H 42)
– Woodhull Medical & Mental Health Center (H 45)
MANHATTAN:
– Bellevue Hospital Center (H 02)
– Beth Israel Medical Center - Petrie Campus (H 03)
January 4th, 2008
PSVAC Training
144