Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
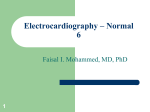
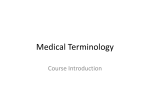
PSIO 603, BME 511 February 21, 2007 1 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] The Electrocardiogram and Arrhythmias READINGS: Boron and Boulpaep pages 483-507 OBJECTIVES: After completion of this lecture and after reading the associated materials, you should be able to: 1. Define dipole. Draw pictures of the heart (frontal plane) indicating areas of polarized and depolarized tissue corresponding to each wave of the ECG. Using vectors, for each picture indicate the orientation and magnitude of the net dipole. 2. Indicate the electrocardiographic conventions of leads I, II and III (Limb Leads). For each net dipole drawn for objective 1 indicate whether a positive or negative voltage would be recorded for each limb Lead. 3. Draw a typical ECG labeling the waves and intervals and indicating their approximate durations. 4. Draw a typical ECG record and on the same time axis indicate the timing of electrical activation of cells in the SA node, atria, AV node, Bundle of HIS, Purkinje network, and ventricle (apex and base). 5. Define 1o, 2o, and 3o heart block and recognize them in ECG records. List the two conditions necessary for a reentrant arrhythmia to occur. LECTURE OUTLINE I. The Electrocardiogram (ECG) A. ECG provides information about 1. Sequence of activation (rhythm and axis) 2. Quantity of tissue activated as a function of time (hypertrophy) 3. Healthiness of tissue (ischemia, infarction) B. Principles of Electrocardiography – Figure 2 1. A dipole is created by current flow between polarized and depolarized regions of the heart. 2. The dipole has orientation and magnitude, which can be represented by a vector with direction and length, respectively. 3. By convention, the vector points towards extracellular positive (intracellular negative). 4. The magnitude of the dipole is determined by the mass of the electrically active tissue and the magnitude of the charge difference. 5. The dipole can be recorded as a voltage by a set of electrodes, one connected to the positive terminal of a voltmeter the other(s) to the negative terminal, and together they form a “lead”. a. A line connecting the electrodes defines the recording axis b. When the dipole is parallel to the recording axis its magnitude is fully detected by the voltmeter, when the dipole is perpendicular to the recording axis it is not detected by the voltmeter. c. When the vector points to the positive electrode, a positive voltage is detected; when the vector points to the negative electrode, a negative voltage is detected. d. When the vector is perpendicular to the recording axis, no voltage is detected. e. The voltage can be recorded as a function of time. During periods when no potential difference exists in the tissue (rest and plateau phase), no voltage is recorded, at all other times a voltage is recorded. C. Vectors and the sequence of activation – Figure 3-5 PSIO 603, BME 511 February 21, 2007 2 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] 1. A clock face can be used to represent the frontal plane of the body; 3 o’clock is arbitrarily assigned a value of 0o, 6 o’clock = 90o, 9 o’clock= ±180, 12 o’clock=-90o 2. Atrial depolarization: vectors at 65o (~5 o’clock) 3. Early ventricular depolarization: vectors between 150o and -200o net vector 175o a. When multiple vectors describe an instant an time, they are summed to determine the net vector b. To sum vectors place them head to tail, maintaining orientation. Connect the tail of the first to the head of the last to depict the net vector (Ptot) 4. Depolarization of apex and LV free wall: vectors between 90o and –30o. repolarization of atrium: vectors at –150o Net vector at 60o 5. Late ventricular depolarization: net vector at –60o 6. Repolarization of ventricle: net vector at 45o D. Electrodes and recording leads 1. Standard ECG uses 9 electrodes, which are used to form 12 "leads", or recording axes 2. Six of these recording axes are in the frontal plane, 6 in the horizontal plane 3. The frontal plane electrodes include the limb leads (I, II, III) a. Lead I - horizontal axis, positive electrode on left arm, negative on right b. Lead II- axis at 60o, positive electrode on lf leg, negative on right arm c. Lead III- axis at 120o, positive electrode on lf leg, negative on lf arm E. Recording the dipole in a specific lead - e.g. lead I 1. Any vector whose tip lies between -90o clockwise to +90o will be detected as a positive voltage by Lead I. Any vector whose tip lies between +90o clockwise to -90o will be detected as a negative voltage by Lead I. 2. To determine the actual voltage detected, make a line perpendicular to the lead axis that passes through the tip of the vector. The distance between the origin of the vector and this perpendicular indicates the voltage detected by the lead. F. Generating the Lead I ECG – Figures 3-5 1. SA node depolarization cannot be detected in the ECG: insufficient tissue mass 2. Atrial depolarization: net vector at 65o; vector length starts small, increases to a moderate length as actively depolarizing tissue mass increases, then decreases to zero as depolarizaing mass decreases to zero 3. AV node depolarization is not detected as a wave in the ECG because of insufficient tissue mass. However, normal function of the AV node is evident in the timing of atrial and ventricular events. 4. Depolarization of the Bundle of His, Bundle branches, and purkinje system is not detected in the ECG as distinct waves due to insufficient mass. However, normal function of the ventricular conduction system is evident in the short duration of the QRS complex. 5. The net vector for ventricular depolarization sweeps from the origin to -175o around to 60o, where its length is maximum, on to –60o and finally returns to the origin. 6. Repolarization of ventricle: vector at 45o II. The ECG A. Definitions: 1. Waves begin and end at 0 mV, or baseline 2. Segments contain no waves originating in the chamber designated by the segment label, e.g. ST segment (end of S to beginning of T) and TQ segment (end of T to beginning of QRS) 3. Intervals contain a segment and one or more waves, e.g. PR (beginning of P-wave to beginning of QRS complex) and QT interval (beginning of QRS to end of T wave) PSIO 603, BME 511 February 21, 2007 3 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] 4. The activity of the conduction system can be detected in the timing of ECG. B. Timing 1. P wave requires 0.05 - 0.10s 2. PR interval requires 0.12 - 0.20s 3. QRS complex requires 0.06 - 0.10s 4. ST segment requires 0.12s (varies considerably with heart rate) 5. T wave requires 0.20s 6. QT interval requires 0.40s (varies considerably with heart rate) III. Arrhythmias A. Heart Block 1. 1o Heart Block - PR interval >0.2s 2. 2o Heart Block - Not all pulses from SA node traverse the AV node. 3. 3o Heart Block - no events from the SA node traverse the AV node B. Sudden Death 1. Reentry can occur when two conditions exist a. Bifurcating path for activation that converges distally on the same tissue. b. Unidirectional block of conduction in one pathway (or greatly differing conduction velocities in the two pathways), e.g. antegrade block 2. Tachyarrhythmia (very fast beat rate) can result. Sustained tachyarrhythmias “decay” into fibrillation, the most common cause of sudden death LECTURE NOTES I. The Electrocardiogram (ECG) Figure 1 depicts the sequence of cardiac depolarization, which begins at the SA node and ends with the last cell of the ventricle and requires ~0.2-0.3 sec (dependent on beat rate and neural modulation). The sequence and timing of depolarization reflect the electrical characteristics of the cells in the different parts of the heart as we have discussed previously and Figure 1- Electrical activation of the heart. (Modified from reference 4) SA node 50 0 50 60 210 70 Atrium -100 0 Atrium -100 0 90 190 190 -100 220 AV node Purkinje Fiber 200 0 -100 160 170 mV 0 0 -100 0 “Endocardial” Ventricle -100 “Epicardial” Ventricle 0 -100 200ms PSIO 603, BME 511 February 21, 2007 4 as shown towards the right of Figure 1. The ECG provides information on the sequence of activation, the quantity of tissue activated (hypertrophy), the health state of the tissue (ischemia and infarction), and the rhythmicity of the tissue. The goal of this presentation, the EGG lab and the ECG small group session is for you to gain an understanding of how the electrical events of the heart are dectected and result in the ECG, and how to recognize rate, rhythm, axis, hypertrophy and ischemia in an ECG. Principles of Electrocardiography As electrical depolarization spreads through a tissue, current flows between adjacent depolarized and polarized regions. This separation of charges across a finite resistance is a dipole, which is detected as a voltage by a voltmeter. (The ECG machine and chart recorders are sophisticated voltmeters.) The dipole has both orientation and magnitude; consequently it can be represented with a vector (or arrow). The direction in which the arrow points denotes the orientation of the underlying dipole, the length of the arrow corresponds to the magnitude of the dipole. The dipole generated during depolarization of a strip of tissue is illustrated in Figure 2a.. Depolarization was initiated on the left and proceeds to the right. The tissue in the shaded region of the strip is the electrically active region and therefore the region generating the dipole. The dipole, represented as a vector, is shown in the middle of the strip – it points towards the polarized tissue. Note that in parts B and C of this figure, the magnitude of the dipole is unchanged (arrow length) but the orientation is reversed because the orientation of polarized and depolarized tissues is reversed. The dipole can be detected by a pair of electrodes (a “lead”) connected to the positive and negative poles of a voltmeter. If these electrodes are placed at either end of the strip, the line connecting the electrodes defines the recording axis (lead axis). The magnitude of a dipole whose orientation is parallel to the recording axis is fully detected by the voltmeter, as observed in A & B. In A the positive electrode detects a positive voltage of +0.25V, the negative electrode detects a negative voltage of -0.25V; the difference between the two electrodes (+0.25V - -0.25V) is displayed on the voltmeter (+0.5V). In B the positive electrode detects - Dr. Janis M. Burt MRB 422; 626-6833 [email protected] Figure 2. Adjacent depolarized and repolarized regions (shaded region) generate signals that can be detected by extracellular electrodes. E F 0 200 msec 50mV 0.5mV PSIO 603, BME 511 February 21, 2007 5 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] 0.25V and the negative electrode detects +0.25V, the difference between the positive and negative electrodes (-0.25V - +0.25V) is displayed on the voltmeter (-0.5V). The dipole in C is oriented perpendicular to the recording axis, it is not detected by the voltmeter because the net current detected by both electrodes is zero. In D the magnitude of the dipole is doubled (relative to that shown in A) due to the doubling in active tissue mass. In this case, the voltmeter detects twice the voltage detected in part A of the figure. (Would the voltage be doubled if the strip were twice as long rather than twice as wide?) Thus, the recording system (voltmeter in this example) displays a voltage whose magnitude is determined by the orientation of the dipole relative to the recording axis, as well as, the magnitude of the dipole (mass of tissue generating dipole). This voltage can be recorded as a function of time on paper to make a permanent record of the electrical events in the tissue. In 2E the depolarization and repolarization events depicted in 2A and 2B are shown as parts of stereotypic ventricular action potentials that might be measured from cells on the left (solid line) vs. right (dashed line) ends of the strip. The output of the voltmeter is shown below the action potentials. Prior to depolarization all cells in the strip are at the same membrane potential; subtracting the voltages measured at either end of the strip produces zero voltage and the voltmeter records zero voltage. With depolarization at the left end of the strip, the potential difference between left and right is detected by the voltmeter as a positive voltage. During the plateau phase, there is no potential difference between the left and right ends and the voltmeter output reads 0. With depolarization there is again a difference between the right and left ends of the strip, but the polarity of the difference is opposite what it was during depolarization and so a negative voltage is recorded. The diffence in shape and amplitude of voltmeter output reflects the slower speed of repolarization vs. depolarization; the slower speed means fewer cells are actively changing potential at each moment of the record. In 2F the appearance of the voltmeter output is altered as the repolarization sweeps across the tissue in the opposite direction of depolarization. Vectors and the Sequence of Activation To see how these principles apply to the depolarization and repolarization of the heart, five time points (depicted in Figure 3) in the cardiac cycle are used: 60 msec - early in atrial depolarization (A), 160, 190 and 210 msec - early (B), middle (C) Figure 3 - Distribution of depolarized and polarized (blue) tissue and late (D) ventricular at five instants during the cardiac cycle (white areas represent the depolarization, and 350 msec - ventricular chambers). Vectors representing orientation and repolarization of the ventricle magnitude of dipoles associated with each time point. (E). Using the principles presented in association with Figure 2, the vectors that represent adjacent regions of polarized and depolarized tissue can be predicted. 60 160 When multiple dipoles with different orientations and magnitudes are present, they have to be summed to determine the direction of the "net dipole" the dipole whose magnitude and orientation are detected by a voltmeter. Figure 4 illustrates how this is done, using instant C from figure 3 as the example. After drawing vectors to depict 190 210 350 the mass and orientation of PSIO 603, BME 511 February 21, 2007 6 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] Figure 4 - Determining the net dipole. 2 -90 1 3 2 3 4 4 o 5 6 1 o 0 ±180 Ptot o +I 7 5 o 90 6 7 adjacent regions of polarized and depolarized tissue, the vectors are summed by placing the tail of second vector at head of first (and of the third on the second) until all vectors are represented. Then connect tail of first vector to head of last vector to derive the "net vector" - labeled Ptot in the figure. The resulting net dipole can be displayed graphically on a polar coordinate system as shown on the right of Figure 4. By convention 0o in the polar coordinate display corresponds to the 3 o'clock position, +90o to the 6 o'clock position, ±180o to the 9 o'clock position, and -90o to the 12 o'clock position. This convention allows us to communicate with people around the world, because when you say the dipole (or more commonly the "axis of depolarization") points towards 60o, everyone knows the vector points towards 5 o'clock. Net Vectors and the Sequence of Activation Activation of the heart begins with depolarization of the SA node. The mass of the SA node is so small that this event produces no detectable potential difference at the surface of the body. Depolarization spreads from the SA node to the surrounding atrial tissue and then through the atria, proceeding from the right side of the heart towards the left, see Figure 5A. The amount of atrial tissue in adjacent depolarized and polarized regions starts out small, swells to a maximum, and then falls back to zero as all cells in the atrium are depolarized (all in plateau phase of the action potential). Throughout the depolarization process, the orientation of the depolarized:polarized tissue can be represented by a vector pointing towards “5 o’clock”, or approximately 65o. However, because the mass of the adjacent depolarized and polarized tissue increases to a maximum and falls back to zero, the vector's length increases to a maximum and decreases back to nothing. Only one instant (60msec time point) of the many required to depolarize the atria (0.1sec required) is depicted in Figure 5A. During depolarization of the atria, the excitatory event reaches the AV node. As was true with the SA node, the mass of the AV node is so small that its depolarization produces no detectable potential difference at the surface of the body. Its normal function, however, is evident from the timing between atrial and ventricular events. After the 0.1 seconds or so required for depolarization of the AV node, the excitatory event spreads to the bundle of HIS, the bundle branches and the purkinje system. Again, the mass of these specialized conduction systems is so small that their depolarization produces no detectable potential difference at the surface of the body. However, they conduct the excitatory event to the endocardial surfaces of both ventricles after which rapid, coordinated depolarization of the ventricles occurs. Thus, normal function of the conduction system (AV node and HIS-purkinje system) is evident from the delay between the conclusion of atrial activation and the beginning of ventricular depolarization. PSIO 603, BME 511 February 21, 2007 7 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] Figure 5 - The net vector at five instants in the cardiac cycle displayed on polar coordinates. A B o -90 o -90 o o 0 ±180 +I o o 0 ±180 o 90 C o 90 D E o -90 o -90 o 0 ±180 o 90 +I +I o o o -90 0 ±180 o 90 o +I o o 0 ±180 +I o 90 The first portion of the ventricle to depolarize is the interventricular septum, beginning in the left ventricle and proceeding towards the right. This depolarization event produces (in some individuals) a potential difference that can be represented as a vector of moderate length oriented towards 8-9 o’clock, or +170o (Figure 5B). Very shortly after initiation of septal depolarization the excitatory event begins to spread through the apex of the ventricles (Figure 5C). Depolarization of the apex can be represented by an arrow of significant length pointed towards 4 o'clock, or +45o. The long length of this arrow reflects the significant mass of the ventricles. Depolarization of the ventricles continues from endocardium to epicardium and from apex to base, such that late in the depolarization event only the LV base remains to be depolarized (Figure 5D). The depolarization event at the base of the heart can be represented by an arrow pointing towards 2 o’clock or -30o. While the ventricles are depolarizing, the atria repolarize. Repolarization proceeds from right to left, which produces a potential difference oppositely oriented to the depolarization event in the atria. This potential difference is not detected as a distinct event by the electrodes on the surface of the body under normal conditions because of the much larger potential difference generated simultaneously by depolarization of the ventricles. The final event in the sequence is repolarization of the ventricles (Figure 5E). This proceeds PSIO 603, BME 511 February 21, 2007 8 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] from the epicardium towards the endocardium; consequently, the polarity of the potential difference is identical to the depolarization event and can be represented by an arrow that points towards 4:30 o'clock (hour hand), or +45o. Depolarization sweeps across the ventricle with a continuously changing net vector that cannot be completely represented by the three time points depicted in figures 3 and 5. As a function of time, a plot of the net vector for the ventricles on a polar coordinate grid reveals a vector loop – Figure 6. It is important to realize that the orientation of the heart influences the direction of the individual dipoles (and the vectors that represent them), the net dipoles, and the vector loop. Electrodes and Recording leads (Objective 2) Figure 6 – The net vector for the ventricle traces a loop that sweeps counter-clockwise as a function of time -90 o Late events ±180 o 0o Early events The ECG depicts the depolarization and repolarization events of the cardiac cycle as a function 90o of time. Nine electrodes (Figure 7 A,C) are used to form 12 leads. For the bipolar limb leads (7A), electrodes are placed on the right arm (RA), left arm (LA) and the left leg (LL). Lead I records between the LA (+) and RA (-), which defines a horizontal recording axis that is positive at 0o. Lead II records between the LL (+) and the RA (-), which defines an axis that is positive at +60o. Lead III records between the LL (+) and the LA (-), which defines an axis that is positive at +120o. Figure 7B shows how the triangular placement of these leads can be "collapsed" inwards to form a polar coordinate system that has the heart at its center. In addition to the three bipolar limb leads, there are 9 unipolar leads, which make use of Figure 7 - Positions of the limb(A) and chest (B) positive electrodes placed on the electrodes, the recording axes for pair of limb electrodes surface of the body and a "virtual" lead (C) and each chest electrode(D), and (E) QRS complexes at the center of the heart. This virtual lead is created electronically by the from each chest lead. (From references 1&2) equipment used to record the ECG and A B I + behaves as if there were an electrode in RA LA the center of the heart. Thus, the axes I + for these unipolar leads extend from the II III surface electrode through the center of II III + + the heart. The precordial leads (V1-V6) define the horizontal or transverse -120 -60 plane. The unipolar limb leads and + + bipolar limb leads define the frontal LL ±180 0 I+ plane. The unipolar limb leads make use of the same electrodes placed on the C right arm (aVR), left arm (aVL), and left +120 +60 leg (aVF) that were used for the bipolar III + II + limb leads. These unipolar electrodes record relative to the center of the heart, so aVF is positive at +90o (negative at –90o), aVR is positive at –150o (negative at +30o) and aVL is positive at –30o (negative at +150o). PSIO 603, BME 511 February 21, 2007 9 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] t P to Lead I (Objectives 1 & 2) If the vectors illustrated in Figures 3 Figure 8 - Determination of component vectors from & 5 are projected onto the axes that the net vector (Ptot). (Modified from Reference 3) I define the frontal plane, as is done in the + polar coordinate graphs of Figure 5, the voltages measured by each recording lead o can be predicted. By way of illustration ±180o 0 +I (Figure 8), consider Lead I. Any vector II III whose tip lies anywhere between -90o clockwise to +90o (shaded region of 8 + + left) will cause a positive voltage to be measured by lead I. Any vector lying between +90o clockwise to -90o will cause a negative voltage to be measured by lead I. Where are the positive and negative domains of Leads II and III? To determine how large the positive voltage measured by lead I will be, you have to determine the component of the net vector that lies in the orientation of lead I. To do this, draw perpendicular lines from the axis to both ends of the vector. Then draw a new vector, along the axis whose ends are defined by these perpendicular lines. As shown on the left in Figure 8, the tail of the net vector is on the lead axis, the dashed line connects the tip of the net vector to the lead axis, forming a right angle with the lead axis. The lead I component vector is formed by connecting the tail of the net vector to the point of intersection of the dashed line with the lead axis. This same strategy can be used for all three leads, as shown in the right panel of figure 8. P to t Lead I ECG With these principles in mind, it can be seen (Figure 9 – next page) that atrial depolarization will produce a positive voltage (deflection) in Lead I. Septal depolarization will produce a negative voltage (deflection), apex depolarization a positive voltage (deflection), and base depolarization a negative voltage (deflection). Ventricular repolarization will produce a positive voltage (deflection) in Lead I. II. The ECG In Figure 10 (two pages distant), the relationship between the visible ECG events and electrical activation of the various areas of the heart, including the conduction system, is illustrated. The ECG is labeled in the boxed inset. The P wave results from depolarization of the atrium, the QRS from depolarization of the ventricles, the T wave repolarization of the ventricles. Each wave begins and ends at 0 volts. A segment begins at the end of one wave and stops at the beginning of another, typically with no intervening waves. Thus, the ST segment begins at the end of the QRS and stops at the beginning of the T wave. Intervals are portions of the ECG that contain a segment and one or more waves. For example, the PR interval extends from the beginning of the P wave to the beginning of the QRS complex (whether or not it has a Q wave). The QT interval extends from the beginning of the QRS complex to the end of the T wave. With these definitions in mind you may wonder why the TQ segment is a segment since the P-wave intervenes. The reason, the P wave arises from a chamber other than the chamber that gives rise to the T and Q waves. Although activity of the conduction system does not produce detectable events in the ECG, its activity can be inferred from the timing of the events that are detected. Thus, if conduction through the AV node, bundle of HIS, bundle branches or purkinje system is slowed,then the PR interval will be prolonged. Similarly, if the ventricle is activated by a means other than the conduction system, the QRS duration will be prolonged. The ranges of normal for each wave, complex, segment and interval are noted below (next page) for a heart rate of ~60 beats per minute. P wave PR interval 0.05 - 0.10sec 0.12 - 0.20 PSIO 603, BME 511 February 21, 2007 QRS complex ST segment T wave QT interval TQ segment 10 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] 0.06 - 0.10 0.1 (decreases with increasing heart rate) 0.15 0.31 (decreases with increasing heart rate) 0.6 (decreases a lot with increasing heart rate) Figure 5 - The net vector at five instants in the cardiac cycle displayed on polar coordinates. A B o -90 o -90 o o 0 ±180 +I o o 0 ±180 o 90 C o 90 D E o -90 o -90 o 0 ±180 o 90 +I o o o -90 0 ±180 o 90 o +I o o 0 ±180 o 90 +I +I PSIO 603, BME 511 February 21, 2007 11 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] Figure 10 - Timing of the sequence of activation, correlation of cellular electrical events to ECG. (modified from Reference 3&4) SA node 50 0 50 70 60 210 Atrium -100 0 Atrium -100 0 90 190 190 mV 0 -100 220 AV node 0 -100 160 Purkinje Fiber 170 0 -100 0 “Endocardial” Ventricle -100 200 “Epicardial” Ventricle 0 -100 QRS Waves P T ST PR TQ Segments Intervals QT 200ms Heart Block First degree heart block occurs when conduction through the AV node is abnormally long (PR interval >0.2 sec). In the example to the right, the PR interval is 0.28 seconds in duration. Second degree block occurs when some impulses traverse the AV node while others do not. This usually occurs in one of two patterns. In Mobitz type I (also known as Wenckebach) second degree block, the PR interval increases in duration with each successive beat until transmission fails (P wave does not elicit a QRS). Following the dropped beat, the pattern repeats itself, with the first impulse after the dropped beat displaying a normal PR interval. PSIO 603, BME 511 February 21, 2007 12 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] In Mobitz type II second degree block, the duration of the PR interval is fixed, but not every P wave elicits a QRS complex. The ratio of P waves to R waves is used to characterize this type of block, for example 3:1 block, illustrated below, tells you that every 3rd P wave elicits a QRS complex. Third degree bl ock indicates that no events are traversing the AV node (or bundle of HIS) into the ventricles. In third degree block, a site other than the SA or AV node initiates ventricular activation, an ectopic site. In the case illustrated below, the large QRS complexes (indicated by arrows) arise from an ectopic site in the left free wall (see picture). Note the slow heart rate. Reentry and Sudden Death Many arrhythmias involve a reentrant mechanism. Reentry can occur when two conditions are present. First, the conduction pathway must diverge into two pathways (A & B Figure 12) and reconverge distally (C). Second, there must be unidirectional block of conduction in one pathway (or greatly differing conduction velocities in the two pathways). This can occur when blood flow to an area of the heart is Figure 12 – Reentry circuit. (from blocked, as occurs during a heart attack. The resulting Reference 3) ischemia causes multiple changes at the cellular level, most importantly depolarization (at least with respect to reentrant arrhythmias). The magnitude of the depolarization reflects the extent of the damage. The result of such depolarization is illustrated in Figure 12 and is A known as a reentry circuit. In conduction pathway B an area of damage is present - bracket labeled AB. The extent of the damage is greatest at the distal edge (near bracket point B), i.e. cells are depolarized to a greater extent at the C distal edge than at the proximal edge. An impulse of normal magnitude arrives at the bifurcation into paths A & B B and is conducted down each path. In the path B, as increasingly damaged (depolarized) cells are encountered, the amplitude of the impulse is diminished, until the impulse fails to propagate any further → thus block occurs. In the path A, the impulse is conducted normally. When the impulse reaches C and the distal side of the area PSIO 603, BME 511 February 21, 2007 13 Dr. Janis M. Burt MRB 422; 626-6833 [email protected] of damage the impulse is conducted retrograde up path B. Retrograde conduction through this path is successful because a normal magnitude impulse reaches the most damaged cells first. The larger stimulus that this normal magnitude impulse represents successfully activates these cells, which in turn activate their less damaged neighbors and conduction proceeds retrograde up the pathway. However, the rate of conduction through the damaged pathway is slow so that by the time the impulse reaches the proximal bifurcation the cells there are no longer refractory and can be reexcited. Thus a repetitive cycling can be established (proceeding A→C→B→A), referred to as a circus rhythm. Each time the impulse makes the cycle the entire ventricle is activated. This type of arrhythmia can frequently be resolved by drug therapy designed to alter the speed of conduction in one or both conduction pathways resulting in a bi-directional block through the damaged region. While the conditions described above for reentrant arrhythmias may seem contrived, they account for the majority of individuals dying from sudden death. Reentrant circuits can also be established when accessory conduction pathways exist between the atrium and ventricle, i.e. pathways other than the AV node (e.g. Wolff Parkinson White Syndrome). References Cited in Figures: 1. Review of Medical Physiology, 13th edition, by W.F. Ganong. Appleton & Lange, Norwalk, 1987. 2. Rapid Interpretation of EKG’s, 4th Ed., by D. Dubin COVER Pub. Co., Tampa, 1989. 3. Physiology of the Heart, 2nd Ed. by A.M. Katz. Raven Press, N.Y., 1992. 4. Physiology, 2nd Ed. By L.S. Costanzo, Saunders, Philadelphia, 2002.