Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
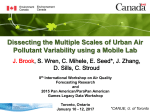
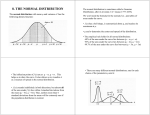
17/10/2012 Health Canada’s Blood Lead Response Guidelines: implications for medical practice, public health and occupational medicine Tom Kosatsky, BCCDC OEMAC 2012 Trends in action level for childhood lead poisoning (1970–1990, CDC, USA) Also, Canada 1994 CDC lowers blood lead limits for young children In May 2012, the U.S. Centers for Disease Control and Prevention (CDC) updated its guidance on the level of lead in a child’s blood it considers harmful. Children with a blood lead level of 5 micrograms per deciliter (μg/dL) are considered by CDC to have more exposure to lead than 97.5% of their peers. This policy changed CDC’s long-standing guidance, which had recommended action at 10 μg/dL. 1 17/10/2012 “ Draft 2011Guidelines “ “No safe level of lead exposure has been identified” Linear models for each cohort study in the pooled analysis, adjusted for maternal IQ, HOME score, maternal education, and birth weight. The figure represents the 5th to 95th percentile of the concurrent blood lead level at the time of IQ testing. “No safe level of lead exposure has been identified” Log-linear model for concurrent blood lead concentration along with linear models for concurrent blood lead levels among children with peak blood lead levels above and below 10 μg/dL. 2 17/10/2012 “Lead has toxic effects on many organ systems at all life stages” “Lead has toxic effects on many organ systems at all life stages” (Needleman, 1990) Population significance of a 5 point IQ reduction 3 17/10/2012 “Current levels of environmental lead exposure in Canada can be harmful” “Subpopulations already experiencing health inequalities are the most vulnerable to lead” Childhood Lead Poisoning from Commercially Manufactured French Ceramic Dinnerware --- New York City, 2003 Lead Poisoning Associated with Ayurvedic Medications --- Five States, 2000-2003 “Simple and inexpensive actions can reduce lead exposure” 4 17/10/2012 With regulation of lead in gasoline, child BLLs have plummeted “The role of the physician is to identify and manage those individuals who are not fully benefiting from the efforts of government and public health agencies to reduce lead exposure in the general population. In order to identify patients with atypical blood lead levels, it is necessary to select those for testing who are most likely at risk. This practice is equivalent to case finding where a “case” is a patient who has a blood lead concentration that is greater than or equal to the 95th percentile of the expected age specific distribution of blood lead in the general population”. “Who and When to Test? Patient reveals potential for lead-related health concerns Patient expresses concern about lead exposure Patient reveals presence of (selected) risk factors Housing/Residence Living in or regularly visiting older homes or buildings with chipping paint or ongoing renovations or remodelling. Infrequent or ineffective housekeeping that results in the accumulation of dust. Family and Behavioural Factors Having a sibling, housemate or playmate known to have had an atypical blood lead level. Living in poverty. Newcomer from at risk countries Food/Consumer Products Use of leaded crystal or pewter food ware. Vegetarian or vegan diet (risk of low iron and calcium status). Use of foreign made food, candies, cosmetics or holistic, herbal, and alternative medicines or folk remedies that are not licensed for sale in Canada (these items generally do not meet English and French labelling requirements).” 5 17/10/2012 “What is the health risk? Concentrations above 20 μg/dL (0.96 μmd/L) are associated with overt symptoms and clinically relevant outcomes. An increase in blood lead levels from 1 to 15 mg/dL: Average reduction of 7 (95% confidence intervals 4 to 10) full scale IQ points in school-aged children. Average increase in adult systolic blood pressure of 4-7 mm Hg An increase in blood lead levels from 1 to 10 mg/dL: Average reduction of 6 (95% confidence intervals 4 to 9) full scale IQ points in school-aged children. Average increase in adult systolic blood pressure of 3-4 mm Hg An increase in blood lead levels from 1 to 5 mg/dL: Average reduction of 4 (95% confidence intervals 3 to 6) full scale IQ points in school-aged children. Average increase in adult systolic blood pressure of 1-2 mm Hg Few data on the potential health effects associated with blood lead concentrations < 1 μg/dL since, until recently, few people had low blood lead concentrations”. Figure illustrates the estimate of the 95th percentile of the blood lead concentration in the general population (solid line) and the 95th percentile upper confidence limit of the estimate (dashed line). Management by Blood Lead Level 6 17/10/2012 “Follow these actions for all individuals: Provide nutritional advice on the value of adequate calcium, iron, and vitamin C intake to reduce absorption or increase the excretion of lead. Provide patient with educational materials on sources of environmental lead exposure and reduction strategies. Check with your local public health unit for their educational materials”. Age-specific estimates of the 95th Percentile Blood Lead Concentrations Note: The data include US NHANES 2007-2008 for ages 2 to 6 years combined with Canadian CHMS data from 6 to 79 and considered representative of the general Canadian population. 7 17/10/2012 If blood lead concentration ≥ the 95th percentile based on the age of your patient, and <20 μg/dL (0.96 μmol/L), follow the recommendations for all individuals and: Take an environmental lead exposure history in order to identify and begin to manage risk factors for elevated blood lead levels. Re-test blood lead in 90 days to determine any temporal trend in the patient's blood lead concentration. If blood lead concentration persists ≥ the 95th percentile for age of your patient, follow the recommendations for all individuals and: Assess patient for iron status. Continue to monitor (every 90 days) until the blood lead level is no longer > 95th percentile. Test blood lead concentrations of others living in the same household. Notify the local public health authority if community exposure source is suspected”. For children of 5-18 years the 95th percentile blood lead is at or slightly over the laboratory detection limit “The challenge for the physician is to help the individual identify the potential source(s) of lead that may be causing the atypical blood lead levels.” “Local public health inspectors have the skills and training to assess community spaces, including child care centres and schools, rental units and community housing to identify potential sources of environmental lead exposure.” 8 17/10/2012 Toxicokinetics of lead Elimination of transferred maternal lead Equilibrium with bone lead stores “Exposure” is largely historic The bad old days 9 17/10/2012 The many residual sources of lead Challenge of source identification Cochrane Summariesbeta Independent high-quality evidence for health care decision making Many educational and environmental household interventions to prevent lead exposure in children have been studied. This review of 14 studies found that educational and dust control interventions are not effective in reducing blood lead levels of young children. There is currently insufficient evidence that soil abatement or combination interventions reduce blood lead levels and further studies need to address this. Household interventions for preventing domestic B, Woolfenden S, Lanphear B, Ridley GF, Livingstone N lead exposure in children Yeoh Published Online: April 18, 2012 Ineffectiveness of interventions Follow these actions for all individuals: Provide nutritional advice on the value of adequate calcium, iron, and vitamin C intake to reduce absorption or increase the excretion of lead. Managing a Child’s Nutrition Although the effectiveness of nutritional interventions has not been established, the following recommendations are common sense and are appropriate advice for all children, including those with elevated BLLs: • Consume adequate amounts of bioavailable calcium and iron. • Consume at least two servings daily of foods high in vitamin C, such as fruits, vegetables, and juices. • Eat in areas that pose a low risk for lead exposure; for example, at a table rather than on the floor. • Participate in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) if the family is eligible. Recommendations from the Advisory Committee on Lead Poisoning Prevention. CDC, 2002 10 17/10/2012 Low Blood Lead Levels Do Not Appear to Be Further Reduced by Dietary Supplements We found no statistically significant relationships between the PbB concentrations and micronutrient ((calcium, magnesium, sodium, potassium, barium, strontium, phosphorus, zinc, iron (limited data), and copper)). In adults and older children with low PbB concentrations and minimal exposure to Pb, microntrient supplementation is probably unnecessary. Brian L. Gulson,1 Karen J. Mizon,1 Michael J. Korsch,2 and Alan J. Taylor3 Environ Health Perspectives 2006 August; 114(8): 1186–1192. ALSO Two-thirds of calcium supplements failed to meet the 1999 California criteria for acceptable lead levels (1.5 µg/daily dose of calcium) in consumer products. What went awry? “ “ Why not treat at the 95th percentile? 1. Low analytic precision around the current 95th percentile BLL for critical age groups 2. BLL does not simply represent current exposure 3. Effective source identification is unlikely at suboutlier BLLs 4. Recommended educational and environmental household interventions to prevent lead exposure in children are ineffective 5. Dietary supplementation is unlikely to reduce and may raise BLL 11 17/10/2012 Potential implications for occupational practice • Inconsistency between action levels (ACGIH) for workers versus the general population • May spur more testing of current and former workers as part of general medical practice • Ineffective advice to workers to manage nonoccupational exposures • Movement of occupational blood lead management from regulatory to the medical practice/public health domains alternatives to the “n rmative approach” • • • • • • Limit recommendations for testing to individuals likely to have a must-intervene blood lead level (20 mcg/dL in the draft document) . In advising physicians, other than for patients with must-intervene blood lead levels, emphasize universal rather than individual measures to lower blood lead. Provide physicians with the population distribution of blood lead by age and gender. Suggest practical ways that patients who wish to do so can recognize sources and reduce their lead exposure; differentiate this advice for infants, children, workers and older adults. Target for intervention those groups at highest levels of exposure, or in whom the consequences of exposure are greatest. An example of the former would be new Canadians, and of the latter women of childbearing age, where nutritional mitigation, and occasionally environmental investigation and remediation, can prevent inter-generation transmission of lead. Surveys are likely to be more effective than screening as a guide to finding these groups and developing ways to reduce their exposure. Identify new and unusual sources by investigating children with blood lead levels over 10 mcg/dL and adults over 20-25mcg/dL, as at these levels there is a reasonable expectation that an exposure source can be identified. Develop a national database to promote recognition of emerging patterns. Support lead source identification and mitigation at the community level. Tom Kosatsky* BCCDC and NCCEH [email protected] 604 7072447 * Opinions expressed here are those of the author 12