Survey
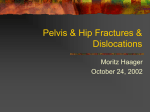
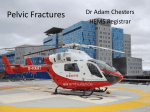
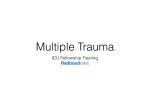
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Classification of pelvic fractures, conservative and operative treatment Acetabular fractures Traumatic hip dislocation Ferenc Urbán 1 Anatomy of the pelvis ► The pelvic ring is made up of two innominate bones and the sacrum, joined posteriorly at the right and left sacroiliac (SI) joints and anteriorly at the symphysis pubis. The innominate bones are formed at maturity by the union of the ilium, ischium, and pubis through the triradiate cartilage 2 The pelvic ring and it’s positioning 3 The most important ligaments ► Posterior & anterior sacroiliac ligaments! ► Sacrospinous ligament ► Sacrotuberous ligament ► Symphysis 4 Anatomical structures of the pelvis 1. ► ► ► ► ► ► ► ► ► ► ► The Greater Sciatic Foramen SEVEN NERVES THREE VESSEL SETS Sciatic nerve (L4-S3) Superior gluteal artery/vein Superior gluteal nerve Inferior gluteal nerve Inferior gluteal artery/ vein Internal pudendal nerve Posterior femoral Internal cutaneous nerve pudendal artery/ vein Nerve to quadratus femoris Nerve to obturator externus ONE MUSCLE Piriformis 5 Anatomical structures of the pelvis 2 6 Functions of the pelvis ► Connects the spine to the lower limbs ► Supports trunk ► Transmits forces applied to trunk on limbs ► Protects organs ► Provides passage for vessels, nerves, and muscles 7 Integrity and stability of pelvic ring are essential 8 High energy trauma Dashboard injury Motor vehicle accident Falling from a height It takes high energy to create such damage... 10 ...so bone is not of primary importance. Life is! Therefore assessment in suspected pelvic ring fracture is according to ATLS (advanced trauma life support) 11 The pelvis is a shock organ! Loss of blood 500-5000 ml 12 13 Diagnostics ► Anamnesis ► Physical examination* ► Native X-ray ► CT scan ► X-ray with contrast material – cystography, angiogr. ► Ultrasound ► Inspection (wound, suffusion, swelling, shortening of the lower limb) ► Palpation Tenderness Stability Pathological movements ► Circulation & innervation of the leg 14 Primary assessment 15 Primary assessment ►Inspection and physical examination 16 Primary assessment ►- ray Standard X- ►- Reveals up to 90% of fractures 17 X-ray of the pelvis AP view 18 Classification of the pelvic fractures by Tile 19 Tile A fractures ► Marginal fractures ► Stable fractures of the pelvic ring 20 Classification of the pelvic fractures by Tile 21 Sagittal forces Lateral forces Tile B fractures 24 Classification of the pelvic fractures by Tile 25 Tile C fractures 26 Müller AO Fracture Classification 61- A type – stable pelvic ring B type – horizontal instability C type – horizontal and vertical instability 27 If the pelvis is the source, then its… Massive blood loss is: ►mostly venous ►due to posterior disruption ►supported by enlarged compartment 28 Emergency treatment Reduce compartment - Stabilize pelvis pelvic clamp external fixator - Surgical tamponade ►- Embolization ►- MAST (military antishock trousers) 29 Pelvic clamp or external fixator 30 Acute phase ► Pelvic clamp 31 External fixator for pelvic injuries ► Shocktherapy! ► Bleedingcontrol ► Avoidance of continous traction ► Conversion ► Rarely definitive method 32 Fracture treatment 33 Emergency treatment ► Stop bleeding otherwise - Stabilize pelvis - - Surgical tamponade laparotomy ► (dcs) retroperitoneum ► ► - Embolization - MAST 34 Stable patient, closed fracture ►There is time for additional ►diagnostics including: ►- X-rays ►- Pelvic organs ►- Neurology 35 Special X-ray views ► Pennal inlet Roentgen tube is turned 45o in cranial direction – brim ► Pennal outlet Roentgen tube is turned 45o in caudal direction - sacrum ► Ala view – 45o contralateral – posterior column and ventral margin ► Obturator view – 45o ipsilateral – anterior column and posterior margin 36 Additional radiology INLET OUTLET 37 Additional radiology CT scan ? 38 3D reconstruction CT scan of the pelvis For planning! 39 Accompanied injuries - Urethra/prostate - Rectum - Vagina - Sphincter/others 40 Accompanied injuries - Urethra/prostate - Rectum - Vagina - Sphincter/others 41 Ultrasound Cystogram Conservative treatment ► Functional treatment ► Continous traction ► Böhler-bed Symphyseolysis < 2 cm 1/7 body weight in the level of the bed in abduction 44 Continous traction •In the level of the bed – without Braun splint •Abduction •1/7 body weight •If tibial tuberosity extension was started after 3 weeks it has to be moved to the femoral condyle 45 Operative treatment 46 Operative treatment 47 Operative treatment 48 Operative treatment 49 Treatment of accompanied injuries and complications ► Urine deviation – catheter and epicystostomy ► Reconstruction of the bladder and urethra ► Treatment of the retroperitoneal haematoma ► Treatment of vessel and nerve injuries 50 Dislocations of the hip Iliacal Suprapubic Ischiadic Obturatorious 51 Dislocations of the hip Central dislocation Post.inf. – ischiadic disl. Sup. Ant. – pubic dislocation Inf.ant. – obturatorious disl. Post. Sup. – iliac dislocation The limb is inversed, the hip extended 52 X-ray of a hip dislocation Iliacal dislocation 53 Treatment of dislocation Closed reduction in narcosis & relaxation Emergency – AVN!!! 54 Retention In case of instability – continous traction or ORIF in fracture dislocations 55 Fractures of the acetabulum 56 Diagnostics of the acetabular fx Ala-felvételview Obturator-view Foramen obturatorium Anterior columnlinea terminalis Posterior margine Acetabular roof Ala Posterior column – linea ilioischiadica Elülső vápapereAnterior marginem Bottom of the acetabulum Continous traction of acetabular fx ► In central dislocation additional lateral pulling is needed 58 Operative treatment of acetabular fractures 59 Surgery Posterior approach by Kocher-Langenbeck Preparation of the schiatic nerve 60 Stable OS – congruency!!! 61 Fractures of the femur head Pipkin IV. 62 Epiphyseolysis of the femoral head Pin fixation is prefered in growing bone!!! 63 Treatment principles in pelvic injuries ► Resuscitate patient (ATLS) ► Evaluate pelvic organs ► Thorough examination of fracture(s) ► Make a plan 64 Treatment options nonoperative/operative Operation rarely needed Anterior stabilization Stabilization of entire ring 65 Operative treatment options ► External fixation ► Internal fixation screws plates ► Combinations 66 Conclusions Due to high-energy trauma: ► First, save patient’s life ► More than just a bony injury ► Stabilization of paramount importance ► Many might be treated nonoperatively 67 Take five or continue? 68