Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
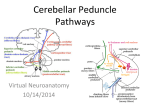
Video J Neurol 2016;1:1–4. www.videojournalofneurology.com Desai et al. CASE REPORT CLINICAL VIDEO 1 ACCESS PEER REVIEWEDOPEN | OPEN ACCESS Vertical upbeat nystagmus with isolated acute middle cerebellar peduncle stroke Kinjal Desai, Thomas Bullock, Rahul Damani, Eric Bershad CASE REPORT A 68-year-old female with diabetes mellitus, hypertension, hyperlipidemia presents with hypertensive urgency, severe nausea, vomiting, and visual impairment. Initial blood pressure was 236/110 mmHg. She had a Glasgow Coma Scale of 15 and National Institute of Health Stroke Scale (NIHSS) of 3 (1 gaze impairment, 1 face weakness and 1 sensory loss). Neurological examination was significant for binocular vertical diplopia in all directions of gaze, worse on far gaze. She also had left lateral rectus weakness, left skew deviation, right hypertropia and a characteristic vertical upbeat nystagmus (left eye more than right eye), which was mostly evident in up and leftward gaze (Video 1). Routine laboratory testing for complete blood count, basic metabolic panel, and cardiac enzymes was unremarkable except for blood glucose of 260. Head computed tomography scan showed no acute abnormality. Brain magnetic resonance imaging scan (Figure 1) demonstrated an acute infarct in the medial aspect of left middle cerebellar peduncle. Her remaining workup, including magnetic resonance angiogram of head and neck and cardiac echo was unremarkable. The etiology of her ischemic stroke were thought to be related to small vessel disease. Kinjal Desai, MD, MPH1; Thomas Bullock, MD2; Rahul Damani, MD, MPH1; Eric Bershad, MD1 Affiliations: 1Baylor College of Medicine, Division of Neurocritical Care; 2Baylor College of Medicine, Department of Neurology. Corresponding Author: Kinjal Desai, Baylor College of Medicine, Division of Neurocritical Care, 6301 Almeda Road, Apt 728, Houston, Texas 77021; E-mail: Kinjal.desai@bcm. edu Received: 03 June 2016 Accepted: 03 August 2016 Published: 05 November 2016 Video 1: Vertical upbeat nystagmus video in a patient with middle cerebellar peduncle stroke. [Video URL at: http://www.videojournalofneurology.com/ archive/early-view-videos/01_VNP01_2016060001_CV_ EV/01_VNP01_2016060001_CV_EV.php]. Figure 1: Diffusion weighted imaging/Apparent diffusion coefficient images of ischemic stroke in the left middle cerebellar peduncle. Anatomy and Localization Cerebellum is connected to brainstem by three bilaterally paired cerebellar peduncles [1]. The superior cerebellar peduncle which connects to Midbrain contains efferent fibers from the dentate, emboliform, globose and fastigial nucleus. The superior cerebellar artery supplies it. The inferior cerebellar peduncle is located medial to middle cerebellar peduncle (MCP) and comprised of an outer restiform body and medial juxtarestiform body. The inferior cerebellar peduncle connects to medulla oblongata and is supplied by posterior inferior cerebellar artery. The MCP connects to Pons and is the most lateral and largest of three peduncles [2]. It contains corticopontine fibers from contralateral side that crosses in pons as transverse pontine fibers and enters MCP to form the mossy fiber pathway. It also receives fibers from pontine tegmental nuclei [1]. The superior cerebellar and anterior inferior cerebellar artery supplies MCP. In our case, given the location of acute ischemic stroke, i.e. medial aspect of MCP, the vertical nystagmus Video Journal of Neurology, Vol. 1, 2016. Video J Neurol 2016;1:1–4. www.videojournalofneurology.com Desai et al. is likely related to fibers traversing through it. The MCP carries information to and from cerebellum (between flocculus and nucleus reticularis tegmenti pontes), which contains vertical pursuit signals encoded with a torsional component [14, 15]. Per Dr Cogan, vertical eye movement disorders can be seen with lesions of anterior vermis, middle vermis, roof nuclei and ocular motor centers located in the floor of the fourth ventricle. The neocerebellum i.e., pontocerebellum contains the declive, folium and tuber which are parts of the midline cerebellar vermis. These tracts then extend into lateral cerebellar hemisphere. A lesion to the roof of the fourth ventricle will often result in skew deviation, as can been seen on the MRI images [2–6]. DISCUSSION Ocular findings are common in cerebellar disease in association with brainstem involvement; however, those that are isolated due to purely cerebellar involvement are not common [3]. The classic ocular manifestation of cerebellar disease is nystagmus, skew deviation, dysmetria and flutter-like oscillations of the eye. Nystagmus is often seen in acute cerebellar disease but is not uncommon in chronic conditions affecting cerebellum [3]. Horizontal nystagmus is more common than vertical or rotatory nystagmus [3]. Vertical nystagmus is greatest when gaze is directed upward. It is associated with jerky rhythmic eye movements [7] and gross weakness of conjugate gaze to the side of lesion [8, 9]. Nystagmus due to lesions of the vermis is usually vertical but less conspicuous [3]. Upbeat nystagmus from a lesion in brainstem usually involves the ventral tegmental tract in the pons and caudal medulla [10]. The ventral tegmental tract originates from superior vestibular nucleus and courses through ventral pons and transmits excitatory upward vestibular signals to the oculomotor nerve nucleus [10]. Gaze-evoked upbeat nystagmus localizes to interstitial nucleus of Cajal in upper midbrain and occasionally to the nucleus intercalatus of Staderini [11, 12]. The nucleus prepositus hypoglossi, medial vestibular nuclei, interstitial nucleus of Cajal and vestibulocerebellum are important for holding the eyes steady in eccentric gaze and form the neural integrator for eye movements [13]. Damage to any of these structures could potentially result in an upbeat or downbeat vertical nystagmus. Diseases involving bilateral middle cerebellar peduncle have been described, for example, degenerative diseases, metabolic diseases (adrenoleukodystrophy, Wilson disease, hypoglycemic coma), neoplasms (brainstem glioma, meningeal carcinomatosis), cerebrovascular disease due to AICA infarction, hypertensive encephalopathy and demyelinating disorders [16]. 2 CONCLUSION A similar case has not been reported before based on our literature search. We present an interesting case of vertical upbeat nystagmus in a patient with isolated middle cerebellar peduncle acute ischemic stroke. Keywords: Brainstem, Cerebellar disease, Erebellar peduncle stroke, Middle cerebellar peduncle, Vertical upbeat nystagmus How to cite this article Desai K, Bullock T, Damani R, Bershad E. Vertical upbeat nystagmus with isolated acute middle cerebellar peduncle stroke. Video J Neurol 2016;1:1– 4. Article ID: 100001VNP01KD2016 ********* doi:10.5348/VNP01-2016-1-CV-1 ********* Author Contributions Kinjal Desai – Substantial contributions to conception and design, Acquisition of data, Analysis and interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published Thomas Bullock – Analysis and interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published Rahul Damani – Analysis and interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published Eric Bershad – Analysis and interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published Guarantor The corresponding author is the guarantor of submission. Conflict of Interest Authors declare no conflict of interest. Copyright © 2016 Kinjal Desai et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original Video Journal of Neurology, Vol. 1, 2016. Video J Neurol 2016;1:1–4. www.videojournalofneurology.com Desai et al. publisher are properly credited. Please see the copyright policy on the journal website for more information. 9. 10. REFERENCES 1. Standring S. Gray’s Anatomy: The anatomical basis of clinical practice, 41ed. Philadelphia: Churchill Livingstone/Elsevier; 2016. 2. h t t p : / / w w w . h u m a n n e u r o p h y s i o l o g y . c o m / cerebellum.htm 3. Cogan DG. Neurology of the ocular muscles, 2ed. US: Charles C. Thomas; 1966. p. 1908–93. 4. Spiegel FA, Scala NP. Positional Nystagmus in cerebellar lesions. J Neurophysiology 1942;5:247. 5. Hare WK, Magoun HW, Ranson SW. Localization within the cerebellum of reactions to faradic cerebellar stimulation. J Comp Neurol 1937;67:145. 6. Ferrier D. Experimental Researches in Cerebral Physiology and Pathology. Br Med J 1873 Apr 26;1(643):457. 7. Cords R. For Pathology of Fuhrungsbewegungen. Archives of Ophthalmolgy 1929:123–73. 8. Holmes G. Symptoms of acute cerebellar injury due to gun shot injuries. Brain 1917;40:461. 11. 12. 13. 14. 15. 16. 3 Bucy PC, Weaver TA Jr. Paralysis of conjugate lateral movement of the eyes in association with cerebellar abscess. Arch Surg 1941;42:839. Pierrot-Deseilligny C, Milea D. Vertical nystagmus: clinical facts and hypotheses. Brain 2005 Jun;128(Pt 6):1237–46. Paul W. Brazis. Localization in Clinical Neurology. 6ed. Philadelphia: Lippincott Williams & Wilkins; 2011. Leigh RJ, Zee DS. The Neurology of Eye Movements, 5ed. New York: Oxford University Press; 2015. Daroff RB. et al. Bradley’s Neurology in Clinical Practice. 6ed. Philadelphia: Elsevier Saunders; 2012. Miller NR. et al. Walsh & Hoyt’s Clinical NeuroOphthalmology, Volume 1, 6ed. Philadelphiaed: Lippincott Williams & Wilkins; 2004. Angelaki DE, Dickman JD. Premotor neurons encode torsional eye velocity during smooth-pursuit eye movements. J Neurosci 2003 Apr 1;23(7):2971–9. Okamoto K, Tokiguchi S, Furusawa T, et al. MR features of diseases involving bilateral middle cerebellar peduncles. AJNR Am J Neuroradiol 2003 Nov-Dec;24(10):1946–54. ABOUT THE AUTHORS Article citation: Desai K, Bullock T, Damani R, Bershad E. Vertical upbeat nystagmus with isolated acute middle cerebellar peduncle stroke. Video J Neurol 2016;1:1–4. Kinjal Desai is a Neurocritical Care Senior Fellow at Baylor College of Medicine in the Department of Vascular Neurology and Neurocritical Care in Houston, Texas, USA. He earned undergraduate Medical Degree MBBS from India at Smt. NHL Municipal Medical College and Residency Training from University of Mississippi Medical Center in Jackson, MS after a Graduate Degree in MPH from University of Southern Mississippi in Hattiesburg, MS. He has published multiple posters, given multiple oral presentations and has worked on book chapters, peer review journals including publications. His research interests include status epilepticus, neuroradiology, stroke and bedside ultrasound. He intends to pursue further training to complete his Doctorate in Public Health upon completion of his neurocritical care training. E-mail: [email protected] Thomas Bullock is a faculty in Baylor College of Medicine, Department of Neurology. Rahul Damani is a faculty in Baylor College of Medicine, Division of Neurocritical Care. Video Journal of Neurology, Vol. 1, 2016. Video J Neurol 2016;1:1–4. www.videojournalofneurology.com Desai et al. Eric Bershad is a faculty in Baylor College of Medicine, Division of Neurocritical Care. Access full text article on other devices Access PDF of article on other devices Video Journal of Neurology, Vol. 1, 2016. 4