Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
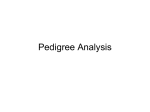
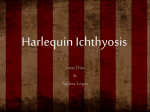
Diagnosis of X-Linked Recessive Ichthyosis Names of all authors were previously in this spot Susquehanna University Affected I Normal 1 2 Based on the general symptoms, Psoriasis, Hyperkeratosis lenticularis perstans, and Ichthyosis were considered to be three possible genetic diseases that the patient’s family members could be diagnosed with. Psoriasis is an “inflammatory skin disease that affects 2% of the population” (Matthews, 1996) and is characterized by “red, scaly skin patches.”(Matthews, 1996) Hyperkeratosis lenticularis perstans, also known as Flegel’s Disease, is an autosomal dominant disease in which lesions are mostly present on the lower extremities (Beveridge, 1973), however they may be found all over the body. Hyperkeratosis lenticularis perstans is often associated with the presence of skin tumors and mostly appears during the third and fourth decades of one’s life. Ichthyosis is characterized as having large, dark brown scales (Hernandez-Martin, 2005) that are first present between ages three to six months. Ichthyosis has multiple modes of inheritance. Materials and Methods • Once the symptoms were assessed, possible genetic diseases were considered. • A family history was determined through a genetic questionnaire and a pedigree was created. • DNA samples were taken from the patient, her mother and father, the maternal grandparents and the paternal grandparents. • These DNA samples were run through agarose gel electrophoresis. The agarose gel, containing 5mLof EtBr, was poured and set into the gel mold. Once it was set, a buffer solution was added. The appropriate wells of the set gel were loaded with 5mL of the dyed DNA samples from the family and gel was run. The gel was removed from the buffer solution and viewed under UV light. •The gel was analyzed and the carriers of the allele for the disease were determined. 3 4 5 6 patient 1 2 3 4 III-4 II-3 II-4 I-1 Figure 1. Pedigree of patient’s family which revealed the genetic disease as an xlinked recessive trait. Family member I-3 and I-4 were identified to be XaY and XAXa respectively. Family member II-3 and II-4 were identified to be XAY and XaXa respectively. Family members III-1, III-2, and III-3 were identified to be XAXa, XaY, and XaY. The patient, III-4, was determined to be XAXa and thus carries the allele. 1-4 None of the patient’s family members died from their symptoms, so it was assumed that the genetic disease is not life-threatening. The symptoms were clinically examined and characterized to be thick, dark scales with an irregular to rhombic shape. When the scales were removed, a bright red base with pinpoint bleeding was revealed. The family members described the affected skin areas as very dry with mostly mild itching and only the paternal grandfather reported basal cell carcinomas. The first sign of symptoms in each case was approximated to be between birth and the first four months of life. 2 III Marker A 16-year-old woman from Syracuse, New York came to a genetic counselor with a history of family members having scaly skin on the scalp, ears, neck, abdomen, legs and feet. She was concerned with her likelihood of acquiring these symptoms and then someday passing them on to her children. In order to address the patient’s concerns, the symptoms of the family members were examined through a family history and several possible genetic diseases were considered and compared. 4 II 1 Introduction 3 I-2 Genetic testing is very important when determining the inheritance of a genetic disease. In this case, a patient came to a genetic counselor explaining a possible disease appearing to run through parts of her family. The symptoms were assessed, a family history was taken, a pedigree was made from the family history, and a gel electrophoresis was run containing the DNA of several family members to determine the alleles of those in the pedigree. Through analysis of the gel and pedigree, the genetic disease was determined to be X-linked ichthyosis. Because of the transmittance of this genetic disease, the patient was determined that she will never show signs of the disease because she is only a carrier of the recessive allele, and she has no chance of having an affected daughter, but a 50% chance of having a daughter carrying the gene. The patient also would have a 50% chance of having a son with the disease and a 50% chance of having a son without the gene. Discussion & Conclusions Results I-3 Abstract Figure 2. Agarose gel containing DNA of family members I-4, I-3, I-2, I-1, II-4, II-3, and III-4. With the help of the pedigree, it was possible to identify the alleles of those family members along with other family members who’s DNA were not run through the gel. Family member 1-4 and III-4 both have two bands visible in the gel, but do not express the trait in the pedigree, so are both heterozygous for Xlinked Recessive Ichthyosis. Family members I-3 and II-4 each only has one band with the smaller allele visible on the gel and express the trait in the pedigree, so both only have the recessive allele. Family members I-2, I-1, and II-3 all have only one band on the gel with the larger allele and do not express the trait in the pedigree, so all only have the dominant allele. •The pedigree (Figure 1) showed an X-linked inheritance pattern for the disease with the maternal grandfather, mother, and two sons showing symptoms of the disease, but the two daughters of the affected mother showed no symptoms •The gel (Figure 2) made it evident that the disease was recessive because family members that showed symptoms of the disease only showed the recessive allele and carriers of the disease had both alleles present •The disease Ichthyosis was determined to be the correct disease based on the symptoms and pattern of inheritance (X-linked recessive) because Psoriasis had no apparent form of inheritance and Hyperkeratosis lenticularis perstans was an autosomal dominant inheritance X-linked ichthyosis is a relatively common genetic genodermatosis with a recessive X-linked mode of inheritance, affecting 1:6000 males. (Hernandez-Martin, 2005) Most cases of X-linked ichthyosis are caused by deletions of the steroid sulfatase gene (STS). (Hazan, 2005) •Symptoms of X-linked ichthyosis include onset at birth, and scaling on the scalp, ears, neck, abdomen, front of legs, and dorsum of feet (OMIM) •Joanna is a carrier of the disease because her mother is homozygous recessive for the disease (XaXa) and her father is unaffected, which means Joanna received a dominant allele from her father and the recessive allele, which carries the disease, from her mother •Joanna will never show symptoms of the disease, but it is a possibility that the recessive allele will be passed onto her children •Joanna has a 50% chance of having a daughter that is a carrier of the disease, but a daughter would not be affected (Figure 3) A son of Joanna has a 50% chance of being affected by the disease •No known cure (Rubeiz & Kibbi, 2003) •Social discrimination and psychological affects are common to those who suffer from the disease (Rubeiz & Kibbi, 2003) •Possible therapies/ treatments: (Traup & Burgdorf, 2007) •Newborns in intensive care watch skin for infection monitor temperature and fluids (should be in lower temperatures) apply non-medicated cream to body check vision and hearing •Infants bathe in sodium bicarbonate rub affected areas with a cloth or towel apply non-medicated cream to rash area keep external area of ear clean physical therapy •Children/Adults same treatments as newborns and infants but a urea cream should be applied to the affected area (stronger concentration on scalp) on warm or hot days exposure to sun should be kept at a minimal, and avoid warm climates References Beveridge, G.W. “Familial Hyperkeratosis Lenticularis Perstans Associated with Tumors of the Skin.” British Journal of Dermatology, 88: Page 453-457. Department of Dermatology, The Royal Infirmary, Edinburgh. Nov. 1972 Hernandez-Martin, A. “X-linked Ichthyosis in a Girl: Strategy for Identifying the Casual Mechanism.” British Journal of Dermatology, vol: 152, iss:1, page 191. 2005 XA XA Y XAXA XAY Xa XAXa XaY Figure 3. Punnet square revealing the probability of the patient passing the trait on to her children. If she has a daughter, there is a 50% chance that she will carry the gene and a 50% change she will not carry it at all. There is no chance of the patient having a daughter expressing the disease. There is a 50% chance of the patient having a son having the disease and a 50% chance that the son will only have the dominant gene. Hazan, C. “X-linked Recessive Ichthyosis.” Dermatology Online Journal, 11(4), page 12. Department of Dermatology, New York University School of Medicine. Dec. 2005. Matthews, D. “Evidence that a Locus for Familial Psoriasis Maps to Chromosome 4q.” Natural Genetics, 14(2): pages 231-233. Department of Biochemistry and Molecular Genetics, Imperial College School of Medicine at St Mary’s, Paddington, London, UK. Oct. 1996. <http.//www.ncbi.nlm.nih.gov/ Online Mendelian Inheritance in Man. (2007). Ichthyosis, X-linked. National Center for Biotechnology Information. Retrieved September 27, 2007, from http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=308100 Rubeiz, N. & Kibbi, A-G. (2003). Management of Ichthyosis in Infants and Children. Clinics in Dermatology, 21, 325-328. Traup, H. & Burgdorf, W.H.C. (2007). Treatment of ichthyosis- There is always something you can do! In Memoriam: Wolfgang Küster. Journal of American Academy of Dermatology, 57, 542-547.