Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
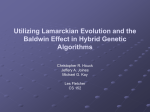
ORIGINAL ARTICLE Influence of chin prominence on esthetic lip profile preferences Grant G. Coleman,a Steven J. Lindauer,b Eser Tüfekçi,c Bhavna Shroff,d and Al M. Beste Charlotte, NC, and Richmond, Va Introduction: The purpose of this study was to determine the influence of chin prominence on preferred lip position in profile. Methods: Five “male” and 5 “female” silhouette profiles differing only in the degree of mandibular retrognathism or prognathism (⫺25°, ⫺18°, ⫺11°, ⫺4°, and ⫹3° facial contour angles) were created. Using a computer animation program, the evaluators moved the upper and lower lips independently into the positions they deemed to be the most esthetic for each profile. The evaluators included white male and female adolescent orthodontic patients, parents of patients, and orthodontists. Results: In general, no differences in preferred lip position were found between the ⫺11° and ⫺4° profiles or between the ⫺18° and ⫹3° profiles, but preferences for each of the 3 profile groupings (⫺11° and ⫺4°, ⫺18° and ⫹3°, and ⫺25°) were different. Fuller lip positions were preferred for the more extreme retrognathic and prognathic profiles, whereas more retrusive lip positions were preferred for the more average profiles. No differences were found among the 3 evaluator groups or between male and female evaluators. Scattered differences were found among lip preferences for male and female profiles. (Am J Orthod Dentofacial Orthop 2007;132:36-42) A n important aspect of orthodontic diagnosis and treatment depends on placing the dentition in the skeleton to achieve maximum soft-tissue esthetics. This is a paradigm shift from the standards of the specialty in the first half of the 20th century, when optimizing the angulation of the teeth in the underlying skeletal structures was the driving force behind orthodontic treatment planning. Early studies illustrate attempts to find the ideal dental and skeletal cephalometric relationships to produce balanced, stable results.1-3 However, early analyses paid little attention to the importance of the soft tissues of the face in maximizing facial harmony and esthetics. In a challenge to the belief that merely positioning the teeth and skeleton in the “ideal” positions would produce good facial esthetics, Burstone4 advocated that soft-tissue profile analysis should be an important a Private practice, Charlotte, NC. Professor and chair, Department of Orthodontics, School of Dentistry, Virginia Commonwealth University, Richmond. c Assistant professor, Department of Orthodontics, School of Dentistry, Virginia Commonwealth University, Richmond. d Professor, Department of Orthodontics, School of Dentistry, Virginia Commonwealth University, Richmond. e Associate professor, Department of Biostatistics, School of Dentistry, Virginia Commonwealth University, Richmond. Supported in part by grants from the Southern Association of Orthodontists and the Alexander Fellowship of Virginia Commonwealth University. Reprint requests to: Steven J. Lindauer, Department of Orthodontics, School of Dentistry, Virginia Commonwealth University, PO Box 980566, Richmond, VA 23298-0566; e-mail, [email protected]. Submitted, February 2005; revised and accepted, July 2005. 0889-5406/$32.00 Copyright © 2007 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2005.07.025 b 36 consideration in orthodontic treatment planning. Later, he stated that lip posture was a critical element not only of overall facial esthetics but also of posttreatment stability and function.5 Ricketts6 described his “esthetic plane” (E-plane), a line extending from the tip of the nose to the tip of the chin, and concluded that it was a convenient reference line for the analysis of lip position. He estimated from clinical observation that the lower lip of adults should be positioned 4 mm posterior to the E-plane ⫾ 3 mm.7 For children, he suggested that the lips should be slightly more full, on average 2 mm posterior to the E-plane ⫾ 3 mm. Ricketts stressed the importance of balance of the lips relative to the nose and the chin, pointing out that overly protruded or retruded lips were unharmonious and unesthetic. Subsequently, several studies evaluated the lip profile preferences of orthodontists and laypeople by having them choose what they considered to be the most pleasing profiles from groups of photographs or silhouettes. Peck and Peck,8 in 1970, found that the public preferred lip profiles that were consistently more full and protrusive than those considered to be ideal by orthodontists according to cephalometric standards. Yehezkel and Turley9 reported that the public now prefers a more full and more convex facial profile for black people than previously. Foster10 found that laymen chose fuller lip profiles for children than adults, consistent with the fact that lip profiles became more retruded with age,11 and that slightly fuller lips were preferred for women than for men. Czarnecki et al12 American Journal of Orthodontics and Dentofacial Orthopedics Volume 132, Number 1 also reported that subjects preferred fuller lips for females, but stated that lip esthetics was closely linked to nose and chin positions; subjects preferred a more protrusive lip profile with a larger nose and a more forward chin position. Nanda and Ghosh13 reiterated the importance of balancing the relationships of nose, lips, and chin for orthodontic patients and stressed that the concept was critical for extraction vs nonextraction decision making. These principles have become commonly accepted and are used in contemporary orthodontic treatment planning. Hier et al14 used a software program that animated the lip profile from retruded to protruded positions so that subjects could choose a range of profiles they considered acceptable as well as the most pleasing point in that zone. They found that female judges and subjects who had never received orthodontic treatment preferred fuller lip profiles than male judges and those who had been treated orthodontically. Several other studies used computer animation and the “zone of acceptability” concept in profile analysis.15-17 Giddon et al15 showed that animated methods for determining profile preferences were more discriminating than a series of static images from which to choose. To date, no studies have evaluated specifically the influence of chin prominence alone on preferred lip position in profile. A wide range of mandibular positions is encountered in the orthodontic patient population. It would be valuable to understand what lip positions are considered the most esthetic for different degrees of mandibular retrognathism and prognathism. Previous studies often required evaluators to select preferred lip positions from a fixed array of choices and did not permit upper and lower lip positions to be changed relative to each other. The purpose of this study was to determine specifically the influence of chin prominence on preferred lip position. MATERIAL AND METHODS The cephalometric soft-tissue profile of a white man treated in the orthodontic department at the Virginia Commonwealth University School of Dentistry was traced. The patient had a Class I dental and skeletal pattern with vertical and anteroposterior measurements in the normal range. Following the recommendations of Foster10 and Czarnecki et al,12 the profile was changed to an androgynous silhouette to reduce the influence of any distracting or sex-defining features. All vertical relationships were unaltered to evaluate only the anteroposterior aspects of the profile. To create a range of mandibular positions representing what might be encountered in clinical practice, the mandibular portion of the silhouette was initially posi- Coleman et al 37 Fig 1. ⫺11° “normal” profile without lips in place. tioned, without the lips in place, to create a “normal” facial convexity angle (G-Sn-Pg) of ⫺11° (Fig 1). From this midpoint, the mandible was moved horizontally in increments of 7° to create a series of profiles with facial convexity angles of ⫺25° (severe Class II), ⫺18° (moderate Class II), ⫺11° (Class I), ⫺4° (moderate Class III), and ⫹3° (severe Class III). The lower part of the profile was divided into the upper one third and the lower two thirds to define the point between the upper and lower lips. By using various facial photographs as references, upper and lower lips were drawn for each profile from a most retruded position to a protruded position extending several millimeters beyond Ricketts’ E-plane (Fig 2). The sequential images for each profile were scanned into a computer. By using the graphic design software Flash MX (Macromedia, San Francisco, Calif), the images were morphed and animated to create a smoothly flowing continuum of lip positions from the most retruded to the most protruded positions. The program was designed so that, with the keypad, the upper and lower lips could be moved independently to any position between retruded and protruded extremes. The evaluators were limited to white people and included 20 male and 20 female orthodontists, 20 male 38 Coleman et al American Journal of Orthodontics and Dentofacial Orthopedics July 2007 Fig 2. Stages of lip protrusion for ⫺11° profile scanned into computer before morphing. and 20 female adolescent orthodontic patients between the ages of 10 and 18 years, and 20 male and 20 female parents of orthodontic patients. Using the computer keypad, each evaluator moved the upper and lower lips to the positions he or she thought were the most pleasing for each profile. The profiles were presented individually in 2 sets. The evaluators were instructed to assume that the first set of profiles was of a man. The first male profile, the ⫺11° (Class I) profile, was repeated to evaluate intraexaminer reliability. The second set of profiles, unchanged but presented in a different order, was assumed to be of a woman. For each new profile shown, the program automatically moved the upper and lower lips separately from the most retruded to the most protruded position and back to demonstrate the full range of possible lip positions. The evaluator always began moving the lips from the most retruded position. The perpendicular distances from the E-plane to the upper and lower lips were measured by using a digital caliper and recorded to the nearest .01 mm for each preferred profile. Mixed-model repeated-measures ANOVA was used to determine differences in lip profile preference related to changes in mandibular position. Between-subject factors considered were evaluator group (patient, orthodontist, or parent) and evaluator sex. Within-subject factors considered were the 5 mandibular positions. Interactions considered were between evaluator group*mandibular position and evaluator sex*mandibular position. The Tukey HSD test was used to determine differences between the 5 profiles separately for upper and lower lip positions. A significance threshold of P ⬍.05 was used for all analyses. RESULTS To test intraexaminer reliability, the ⫺11° male profile was repeated in the series presented to the evaluators. Repeated-measures ANOVA was used to compare the identical profiles and showed that preferences for both upper and lower lip positions between the 2 differed significantly (P ⬍.001). The preferred upper and lower lip positions for the second ⫺11° profile were more full than the first. The lower lip averaged 0.72 mm fuller (P ⬍.001), and the upper lip averaged 0.55 mm fuller (P ⬍.005) in the second profile. This suggested that differences in preferred lip positions for the other profiles studied would have to be greater than 0.72 mm to be considered meaningful. A mixed-model repeated-measures ANOVA was used to determine differences in lip profile preference related to changes in mandibular position. Betweensubject factors considered were evaluator group (patient, orthodontist, or parent) and evaluator sex. Neither of these was found to be a statistically significant factor (P ⬎.20) influencing positioning preference for either the upper or the lower lip. Within individual subjects, mandibular position was found to significantly influence lip profile preferences for both the upper lip (P ⬍.0001) and the lower lip (P ⬍.0001). The effect of mandibular position on lip profile preference was different among evaluator groups for the upper lip (P ⬍.0001) and the lower lip (P ⬍.005) but was not different between male and female evaluators (P ⬎.40 and P ⬎.15 for upper and lower lips, respectively). Average upper and lower lip position preferences for each profile and evaluator group are shown in Figure 3 and the Table. All average preferred lip positions were posterior to the E-plane. In each evaluator group, there were significant differences in preferred lip position for the 5 mandibular positions (P ⬍.001). The Tukey HSD was used to determine the specific differences. ● For both upper and lower lips in the patient evaluator group, the ⫺11° and ⫺4° profiles were not different, Coleman et al 39 American Journal of Orthodontics and Dentofacial Orthopedics Volume 132, Number 1 Table. Mean lip positions in each evaluator group (all distances posterior to E-plane) Lower lip Profile (°) Mean (mm) Patient evaluators ⫹3 2.15 ⫺4 4.31 ⫺11 4.59 ⫺18 2.70 ⫺25 0.32 Orthodontist evaluators ⫹3 3.19 ⫺4 5.34 ⫺11 4.83 ⫺18 3.18 ⫺25 1.72* Parent evaluators ⫹3 2.12 ⫺4 4.66 ⫺11 5.05 ⫺18 3.06 ⫺25 0.21 Upper lip 95% CI (mm) Mean (mm) 95% CI (mm) 1.45-2.85 3.61-5.01 3.94-5.25 1.99-3.40 ⫺0.38-1.02 5.23 6.73 6.92 5.22 2.57 4.54-5.92 6.04-7.42 6.27-7.57 4.53-5.91 1.88-3.26 2.49-3.90 4.64-6.04 4.17-5.48 2.48-3.88 1.02-2.42 5.83 7.46 6.71 4.96 2.79 5.14-6.52 6.78-8.15 6.06-7.37 4.27-5.65 2.10-3.48 1.41-2.82 3.96-5.36 4.40-5.71 2.36-3.76 ⫺0.49-0.91 4.64 6.70 7.21 5.42 2.80 3.95-5.32 6.01-7.39 6.56-7.86 4.73-.11 2.11-3.49 *Orthodontists different from other evaluator groups (P ⫽ .0039). Fig 3. Mean upper lip and lower lip positions behind E-plane for each profile. ● ● the ⫺18° and ⫹3° profiles were not different, but each of the 3 profile groupings (⫺11° and ⫺4°, ⫺18° and ⫹3°, ⫺25°) were significantly different from each other. In the orthodontist evaluator group, lower lip position for the ⫺11° and ⫺4° profiles was not different, and the ⫺18° and ⫹3° profiles were not different, but each of the 3 profile groupings (⫺11° and ⫺4°, ⫺18° and ⫹3°, ⫺25°) was different from each other. For upper lip position, all 5 profiles differed significantly from each other. For the parent evaluators, lower lip position for the ⫺11° and ⫺4° profiles was not different, but each of the 4 profile groupings (⫺11° and ⫺4°, ⫺18°, ⫹3°, ⫺25°) was different from each other. For upper lip position, the ⫺11° and ⫺4° profiles were not different, and the ⫺18° and ⫹3° profiles were not different, but each of the 3 profile groupings (⫺11° and ⫺4°, ⫺18° and ⫹3°, ⫺25°) was different from each other. There were no significant differences in preferred upper or lower lip positions among patient, orthodontist, and parent evaluators for any of the 5 profiles with 1 exception: for lower lip position of the ⫺25° profile, patient and parent responses differed significantly from that of orthodontists (P ⬍.005). Patient and parent evaluators placed the lower lip in a more full position than did orthodontists. For lower lip position, 2 profiles in the patient evaluator group and 3 profiles in the parent evaluator group showed significant differences in lip preference between male and female profiles, whereas the orthodontist evaluators showed no significant differences in preferred lower lip position. For upper lip position, 1 profile in the patient evaluator group, 2 profiles in the orthodontist evaluator group, and 3 profiles in the parent evaluator group showed significant differences in lip preference between male and female profiles. In all cases when a significant difference was found, the evaluators preferred fuller lips for the female profiles than for the male profiles. There were no significant differences in preferred upper or lower lip positions between male and female evaluators in the 3 evaluator groups (P ⬎.16). DISCUSSION Orthodontists encounter various mandibular positions in their patients. Moderate to extreme retrognathic and prognathic mandibular positions are often found, and challenging treatment decisions must be made to maximize the esthetic and functional benefits to each patient. When surgical intervention is not a viable option, compromises in the orthodontic treatment plan must be 40 Coleman et al considered. Positioning of the lips is an important factor affecting overall facial balance in attempts to maximize facial esthetics, especially when jaw position cannot be altered. The results of this study showed that mandibular position does significantly impact preferred lip position relative to Ricketts’ E-plane and that different esthetic standards should be applied to the various profiles encountered in clinical practice. Androgynous silhouettes, as in this study, for evaluation of profile esthetics have been advocated by previous authors because this eliminates other possible esthetic variables such as hair, complexion, and eyes.10,12 However, it might also detract from the realism of the profile as perceived by evaluators. Similarly, using a silhouette might have challenged the evaluators’ imaginations when they were asked to distinguish between “male” and “female” profiles. It is likely that the lip position preferences for individual patients, whose other facial features are not obscured from view, can differ depending on the influence of these other factors. Because of this, our data are most useful for distinguishing trends in lip profile preference based on relative differences in chin prominence rather than for pinpointing ideal lip positions based on specific facial profile features. Therefore, the ideal lip positions for specific patients should be determined individually based on reasonable clinical judgment, rather than on formulas used to describe population means. Preferences for both upper and lower lip positions differed significantly between the 2 replicate profiles, with the examiners preferring fuller lips in the second replicate (P ⬍.001). Although these differences were statistically significant, they were small enough to be considered clinically unimportant. For this reason, later analyses involving the ⫺11° (Class I) profile averaged the responses for the 2 replicates. There are 2 possible explanations for the differences observed. First, the evaluators might have experienced a “learning curve” effect by which, as they progressed through the different profiles and perhaps because of the order in which the profiles were presented, their preferences and their skill at selecting the lip positions changed so that they intentionally selected fuller lips when viewing the replicate profile. The second possibility is that the evaluators were simply inconsistent in their choice of lip positions, resulting in the observed differences. Since, for the replicate profiles, lip position preferences differed by an average of 0.72 mm, any differences between profiles of less than 0.72 mm should be considered clinically insignificant. In comparison, significant differences in average lip position preferences among the profiles with varying mandibular positions were 3 to 6 times this magnitude American Journal of Orthodontics and Dentofacial Orthopedics July 2007 for the lower lip, and 2 to 6 times this magnitude for the upper lip. Figure 3 demonstrates a consistent trend among the 3 evaluator groups. For both upper and lower lips, the average preferred lip position generally did not differ between the ⫺18° (moderate Class II) and ⫹3° (severe Class III) profiles or between the ⫺11° (Class I) and ⫺4° (moderate Class III) profiles, whereas preferences in the ⫺25° (severe Class II) profiles always differed significantly from the others. This pattern was consistent in all 3 evaluator groups with 2 minor exceptions: for the orthodontist evaluators, all 5 profiles differed significantly from each other for upper lip position, and for the parent evaluators, the ⫺18° and ⫹3° profiles were different for lower lip position. Profiles representing the average lip positions selected by the evaluators are shown in Figure 4. In general, the evaluators preferred the fullest lips for the most retrognathic (⫺25°) profile, less full lips for the moderate Class II (⫺18°) and severe Class III (⫹3°) profiles, and the most retrusive lips for the Class I (⫺11°) and mild Class III (⫺4°) profiles (all relative to Ricketts’ E-plane). A possible explanation for this trend is that the evaluators were attempting to compensate for or distract from larger skeletal discrepancies in the profiles by making the lips more full. Another interpretation of these findings is that the use of Ricketts’ E-plane, which is partly defined by the soft-tissue chin point, is an unreliable method for determining the most esthetic lip positions in differing mandibular positions. Perhaps another reference line derived from other anatomical points and less greatly influenced by variations in chin position would yield more consistent lip position preferences among differing facial profiles. With the evaluators’ preferred lip positions, the nasiolabial angle became progressively more acute, and the labiomental fold became progressively more shallow as the profiles progressed from most retrognathic to most prognathic. These extremes are natural compensations that would be expected in severe Class II or Class III skeletal profiles. The finding that there were generally no differences in preferred lip position among the 3 evaluator groups for any of the 5 profiles agrees with a previous study by Cox and Van der Linden,18 in which no difference in the esthetic rating of profiles between orthodontists and laymen was found. The consistency in lip profile preferences among patients, orthodontists, and parents is quite remarkable because of the wide range of possible positions for the lips for each profile and the high degree of control the evaluators had over where to place the lips. This is an encouraging result when treatment planning is considered, suggesting that es- Coleman et al 41 American Journal of Orthodontics and Dentofacial Orthopedics Volume 132, Number 1 Fig 4. Mean lip positions preferred by all evaluators for each facial profile (⫺25°, ⫺18°, ⫺11°, ⫺4°, ⫹3°, respectively, from left to right). More protrusive lower lip outline shown for ⫺25° profile is mean preference of patient and parent evaluators. thetic goals of orthodontic clinicians with regard to lip position are generally in harmony with those of patients and their parents. The differences that were found between preferred lip positions for the male and female profiles were scattered and inconsistent, ranging from 0.77 to 1.75 mm. No trends could be identified to clarify why certain profiles in an evaluator group showed sex differences, but others did not. Whenever a significant difference was detected, the preference was always for fuller lips in the female profile. This agrees with previous findings by Foster10 and Czarnecki et al.12 There were no differences in preferred lip position between the male and female evaluators in the 3 evaluator groups (P ⬎.16). This contrasts with the findings of Hier et al,14 who determined that female subjects preferred a fuller lip position for the observed profiles than did male subjects. CONCLUSIONS The results of this study showed that mandibular position does significantly influence preferred upper and lower lip positions in profile. In general, preferred lip positions did not differ between the Class I (⫺11°) and moderate Class III (⫺4°) profiles or between the moderate Class II (⫺18°) and severe Class III (⫹3°) profiles, but lip positions were significantly different between the 3 profile groupings (⫺11° and ⫺4°, ⫺18° and ⫹3°, and ⫺25°). More full lip positions relative to Ricketts’ E-plane were generally preferred for the more extreme retrognathic and prognathic profiles, whereas more retrusive lip positions were preferred for the more average profiles. Nasiolabial angles became progressively more acute and labiomental folds more shallow with changing lip position preferences as the profiles progressed from most retrognathic to most prognathic. Preferred lip positions were generally similar among orthodontists, patients, and parents of patients, and between male and female evaluators. Differences in lip positions between male and female profiles were scattered and inconsistent but, when present, always showed a preference for fuller lips in the female profiles. These findings suggest that chin prominence should be considered by the orthodontic practitioner during treatment planning when determining the ideal lip position for a patient. By using Ricketts’ E-plane to analyze lip profiles, the amount of lip protrusion deemed most esthetic varies depending on the position of the mandible. More full lips relative to the E-plane might be considered more esthetic and necessary for the achievement of overall facial balance in patients with more extreme degrees of retrognathism or prognathism, whereas less full lips might be more acceptable for patients with average profiles. REFERENCES 1. Downs WB. Variations in facial relationships: their significance in treatment and prognosis. Am J Orthod 1948;34:812-40. 2. Steiner CC. Cephalometrics for you and me. Am J Orthod 1953;39:729-55. 3. Tweed CH. The Frankfort-mandibular incisor angle (FMIA) in orthodontic diagnosis, treatment planning, and prognosis. Angle Orthod 1954;24:121-69. 42 Coleman et al American Journal of Orthodontics and Dentofacial Orthopedics July 2007 4. Burstone CJ. The integumental profile. Am J Orthod 1958;44: 1-25. 5. Burstone CJ. Lip posture and its significance in treatment planning. Am J Orthod 1967;53:262-84. 6. Ricketts RM. Planning treatment on the basis of the facial pattern and an estimate of its growth. Angle Orthod 1957;27: 14-37. 7. Ricketts RM. Esthetics, environment, and the law of lip relation. Am J Orthod 1968;54:272-89. 8. Peck H, Peck S. A concept of facial esthetics. Angle Orthod 1970;40:284-318. 9. Yehezkel S, Turley PK. Changes in the African American female profile as depicted in fashion magazines during the 20th century. Am J Orthod Dentofacial Orthop 2004;125:407-17. 10. Foster EJ. Profile preferences among diversified groups. Angle Orthod 1973;43:34-40. 11. Forsberg CM, Odenrick L. Changes in the relationship between the lips and the aesthetic line from eight years of age to adulthood. Eur J Orthod 1979;1:265-70. 12. Czarnecki ST, Nanda RS, Currier GF. Perceptions of a balanced profile. Am J Orthod Dentofacial Orthop 1993;104:180-7. 13. Nanda RS, Ghosh J. Facial soft tissue harmony and growth in orthodontic treatment. Semin Orthod 1995;1:67-81. 14. Hier LA, Evans CA, BeGole EA, Giddon DB. Comparison of preferences in lip position using computer animated imaging. Angle Orthod 1999;69:231-8. 15. Giddon DB, Bernier DL, Evans CA, Kinchen JA. Comparison of two computer-animated imaging programs for quantifying facial profile preference. Percept Mot Skills 1996;82:1251-64. 16. Anderson NK, Evans CA, Giddon DB. Comparison of perceptions of computer-animated left- and right-facing profiles. J Prosthodont 1999;8:72-9. 17. Kitay D, BeGole EA, Evans CA, Giddon DB. Computeranimated comparison of self-perception with actual profiles of orthodontic and nonorthodontic subjects. Int J Adult Orthod Orthognath Surg 1999;14:125-34. 18. Cox NH, Van der Linden FPGM. Facial harmony. Am J Orthod 1971;60:175-83. ESTATE PLANNING & PLANNED GIVING Estate Planning: The AAO Foundation offers information on estate planning to AAO members and their advisors on a complimentary basis and at no obligation. Planned giving: Persons who are contemplating a gift to the AAO Foundation through their estates are asked to contact the AAOF before proceeding. Please call (800) 424-2481, extension 246. Please remember the AAO Foundation in your estate planning.