Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
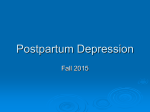
m2Health Application, a Consumer Health Informatics Tool for Evidence-based Self-Management Against Postpartum Infection Mary O. 1,2 Ejiwale , Timothy 2 Patrick , Jake 2 Luo 1. Biomedical and Health Informatics, PhD Program; UWM-Milwaukee, 2. Department of Health Informatics and Administration, UWM-Milwaukee. GOALS ABSTRACT Maternal morbidity and mortality is a public health concern for both the developed and developing nations. At the global level, infection (sepsis) is the second leading cause of postpartum complications, and death surrounding childbirth, abortion or miscarriage. It persistently remains the third cause of pregnancy-related death in the United States (Center for Disease Control and Prevention [CDC]. 2012, 2017). It is also the first leading cause of women’s death in the United Kingdom (Acosta et al., 2014). The occurrence of maternal sepsis is independent of the mode of delivery, natural or caesarean section, although, the latter has a higher predisposition. SIGNIFICANCE OF THE PROBLEM Pregnancy-related death takes the lives of over 600 women per year, (Centers for Disease Control and Prevention, [CDC]. 2012), 99 % of such death takes place in the developing countries (World Health Organization, [WHO]. 2016). At least, half of maternal deaths are of preventable causes, which include puerperal infection (Bingham, Strauss, & Coeytaux, 2011); (Shamshad, Shamsher, & Rauf, 2010). Every 90 seconds, a woman succumbs to needless death of this nature (American Public Health Association, 2011) [APHA], 2011). Additionally, Isabey, Poliquin, Schneider, & Morris (2015) assert that postpartum infection is cost-ineffective, as it accounts for one third of maternal re-admission, and emergency room visit after the initial discharge, with, Urinary Tract Infection (UTI), and surgical site infection (SSI) being the most reported childbirth-related sepsis (Bommarito, Fraser, & Olsen, 2015). Early detection and reporting are lifesaving strategies for this problem (WHO, 2016). DATA SPEAKS! The aim aim od od this this study study is is to:: to:: The Introduce Introduce aa novel novel approach approach to to the the prevention, prevention, early early recognition and reporting of postpartum sepsis. recognition and reporting of postpartum sepsis. Develop Develop aa consumer-centric consumer-centric mobile mobile health health application, called, called, “m2Health” “m2Health” (Maternal (Maternal Mobile Mobile application, Health), thatofprovides provides evidence-based self-care Comparison: Summary Pregnancy-related Mortality Data in USA, Health), that evidence-based self-care 2011–2012, and 2011-2013 (The latest data available, Jan, 2017). information to women ofdue both the developed developed and information women of both the and Observation: Percentageto of Maternal Death to Infection Remains Unchanged developing nations. developing nations. Enhance Enhance women’s women’s health health decision decision making making power power through the the concept of self-monitoring, and selfthrough management, so they become co-producers of postpartum quality outcome with their providers. Ultimately support the World Health Organization Source:Safe CenterMotherhood for Disease Control and Prevention (CDC) (WHO)’s global Initiative FUNCTIONALITIES The aim of this study is, To: Introduce a novel approach to the prevention, early recognition and reporting of postpartum sepsis. Develop a consumer-centric mobile health application, called, “m2Health” (Maternal Mobile Health), that provides evidence-based self-care information to women of both the developed and developing nations. Enhance women’s health decision making power through the concept of self-monitoring, and selfmanagement, so they become co-producers of postpartum quality outcome with their providers. Ultimately support the World Health Organization (WHO)’s global Safe Motherhood Initiative m2Health “app” has dual phases of functionality: Early Start Phase: This is the antenatal phase. The main goal of this phase is to prepare for a healthy postpartum outcome, through a “good” prenatal self-management. Users also get acquainted with the application, build selfconfidence in navigating and interacting with the “app” before their pregnancy is over. Latter Phase: The pregnancy is over (childbirth, abortion or miscarriage) at this stage. m2Health “app” users interact with the “app” for the first six weeks after pregnancy (puerperium). Active self-management and monitoring activities kicks in against clinical signs and symptoms of maternal sepsis etc. Both phases work towards the realization of a healthy postpartum outcome. METHODOLOGY This is a cohort and prospective study. Fifty pregnant women would be recruited during their first antenatal care visit. The participants would be divided into experimental and control group. The control group would continue with the current antenatal and postpartum care protocol, practices and guidelines, while the experimental group uses the m2Health “app”, both also at the antenatal and postpartum period (after childbirth, abortion or miscarriage). Every participant in the latter group would be given one free digital body thermometer of the same brand for temperature measurement. The attending nurse would demonstrate how to measure, and record the values of three cardinal vital signs that are pertinent to maternal sepsis (temperature, respiration, and heart rate). The “app” includes the normal range of these measurements, and flags any aberrant, so, the patient can promptly seek medical intervention. This self-monitoring exercise continues till the end of the first six-weeks after pregnancy (puerperal phase). Other Evidence-based information related to nutrition during and after pregnancy, personal hygiene (hand, vulva and breast), and other self-care activities related go pregnancy and puerperium are also available through the “app”. WHY AN “APP” ? Paper-based Postpartum Health Information Internet-based Postpartum Health Information “Hard to narrow down internet-based postpartum health information. Wish there’s an “app” focusing on maternal sepsis” –Hypothetical postpartum woman. Extensive research proves the acceptance (Willcox et al., 2015) and effectiveness of patient-facing application as a medium for disseminating maternal health education (Zurovac, D., Talisuna, A. O., & Snow, R. W., 2012). Evidence also exists supporting self-care as a efficient approach to promoting postpartum quality outcome (Jung ES, 2002); (Troy & DalgasPelish, 2003); (de Vaate, Coleman, Manneh, & Walraven, 2002), and safe motherhood (Vincent De Brouwere and Wim Van Lerberghe., 2004). mHealth application ameliorates the shortcomings of paper-based maternal health education(e.g. loss of material), breaks the barrier of location/ distance to tested-and-proven postpartum care information, making it readily available and accessible to women of both the developed and developing nations, enhances women’s health decision making power, and promotes safe motherhood at the global level. Additionally, this application supports the concept of self-monitoring by enabling women to measure and record their vital signs, know the normal range of values and promptly identify and report an aberrant. Cardinal Signs and Symptoms of Puerperal Infection: Fever: Temperature >100.4 F (38.0 C ), rigors / chills, tachycardia (Heart rate >= 90bpm), respiration rate >20 breaths/min, pain / tenderness (Lower abdominal, breast, episiotomy or surgical site) (Royal College of Obstetricians and Gynecologists, 2012). CONCLUSION Postpartum infection turns tragic so quickly, early detection is the key. This formidable work-in progress is an innovative strategy against this global health problem.m2Health application would save the cost associated with readmission due to peurperal sepsis, and it would save women’s lives throughout the world. m2Health “APP” IN A FLASH! . REFERENCE Acosta, C. D., Kurinczuk, J. J., Lucas, D. N., Tuffnell, D. J., Sellers, S., & Knight, M. (2014). Severe maternal sepsis in the UK, 2011-2012: A national case-control study. PLoS Medicine, 11(7), e1001672. doi:10.1371/journal.pmed.1001672 2. American Congress Of Obstetrics and Gynecologist, [ACOG]. (2016, May 24,). Ob-gyns stress the importance of postpartum care: The fourth trimester. Targeted News Service (TNS) 3. American Public Health Association. (2011). Reducing US maternal mortality as a human right (policy number: 201114). Retrieved from https://www.apha.org/policies-andadvocacy/public-health-policy-statements/policy-database/2014/07/11/15/59/reducing-usmaternal-mortality-as-a-human-righ 4. Bingham, D., Strauss, N., & Coeytaux, F. (2011). Maternal mortality in the united states: A human rights failure. Contraception, 83(3), 189-193. doi:10.1016/j.contraception.2010.11.013 5. Bommarito, K. M., Fraser, V., & Olsen, M. (2015). 743The incidence of postpartum infections at delivery, post-discharge emergency department (ED) visit, and six week readmission. Open Forum Infectious Diseases, 2(suppl_1), S35. doi:10.1093/ofid/ofv131.96 6. Centers for Disease Control and Prevention, [CDC]. (2012). Pregnancy-related deaths. Retrieved from https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancyrelatedmortality.htm 7. Center for Disease Control and Prevention. Pregnancy Mortality Surveillance System (2014, 2017). Retrieved October 23, 2016 from http://www.cdc.gov/reproductivehealth/MaternalInfantHealth/PMSS.html 8. Conroy, K., Koenig, A. F., Yu, Y., Courtney, A., Lee, H. J., & Norwitz, E. R. (2012). Infectious morbidity after cesarean delivery: 10 strategies to reduce risk. Reviews in Obstetrics & Gynecology, 5(2), 69-77. 9. de Vaate, A. b., Coleman, R., Manneh, H., & Walraven, G. (2002). Knowledge, attitudes and practices of trained traditional birth attendants in the Gambia in the prevention, recognition and management of postpartum haemorrhage. Midwifery, 18(1), 3-11. doi:10.1054/midw.2001.0289 10. Jung ES, Y. E. (2002). A study for the development of standardized management manuel in sanhujoriwon: Centered on the management of women & newborn. "Korean J Women Health Nurs" [JTI], 8(2), 301-313. 11. Khaskheli, M., Baloch, S., & Sheeba, A. (2013). Risk factors and complications of puerperal sepsis at a tertiary healthcare centre. Pakistan Journal of Medical Sciences, 29(4), 972. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/24353670 12. Royal College of Obstetricians and Gynecologists. Green-top Guideline No.64b. April 2012. Sepsis Following Pregnancy: Retrieved October 16, 2016 from https://www.rcog.org.uk/en/guidelines-research-services/guidelines/gtg64b/ 13. Shamshad, Shamsher, S., & Rauf, B. (2010). Puerperal sepsis--still a major threat for parturient. Journal of Ayub Medical College, Abbottabad : JAMC, 22(3), 18. 14. Troy, N. W., & Dalgas-Pelish, P. (2003). The effectiveness of a self-care intervention for the management of postpartum fatigue. Applied Nursing Research, 16(1), 38-45. doi:10.1053/apnr.2003.50001 15. Vincent De Brouwere and Wim Van Lerberghe. (2004). Safe motherhood strategies: A review of the evidence. Reproductive Health Matters, 12(24), 234. 16. Willcox, J. C., van der Pligt, P., Ball, K., Wilkinson, S. A., Lappas, M., McCarthy, E. A., & Campbell, K. J. (2015). Views of women and health professionals on mHealth lifestyle interventions in pregnancy: A qualitative investigation. JMIR mHealth and uHealth, 3(4), e99. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/26510886 17. World Health Organization, [WHO], (2016). Maternal mortality (fact sheet no. 348). Retrieved from http://www.who.int/mediacentre/factsheets/fs348/en/ 18. Zurovac, D., Talisuna, A. O., & Snow, R. W. (2012). Mobile phone text messaging: Tool for malaria control in Africa.(essay)(report). PLoS Medicine, 9(2)