Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
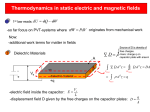
Dept of ENT Surgery - Antibiotic guidelines (May 2013) Condition First Line Intravenous Antibiotic Penicillin allergy Notes Severe Tonsillitis Benzyl Penicillin 1.2 g IV QDS plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to swallow) Clarithromycin 500mg IV BD plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to swallow) If patient has had more than 5 days of oral Penicillin V then use Co-amoxiclav 1.2g IV TDS. If patient has infectious mononucleosis (glandular fever) and >5 d oral Penicillin V use Cefuroxime 750mg IV TDS and Metronidazole 500mg IV TDS Peritonsillar abscess (Quinsy) Benzyl Penicillin 1.2 g IV QDS plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to swallow) Clarithromycin 500mg IV BD plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to take PO) If patient has had a course of oral Penicillin V then use Cefuroxime 750mg IV TDS and Metronidazole 500mg IV TDS Acute Epiglottitis (Paediatric) Ceftriaxone IV once daily (Dose calculation as per BNF) D/W Microbiology only if type 1 anaphylaxis Supraglottitis (Adult) Cefuroxime 1.5g IV TDS plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to swallow) D/W Microbiology only if type 1 anaphylaxis Neck abscess Co-amoxiclav 1.2g IV TDS Clarithromycin 500mg IV BD plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to take PO) Orbital cellulitis (Paediatric) Cefotaxime IV plus Metronidazole IV (Dose calculation as per BNF) D/W Microbiology only if type 1 anaphylaxis Pinna/Facial Cellulitis (superficial skin / soft tissue) Flucloxacillin 1g IV QDS plus BenzylPenicillin 1.2g IV QDS Clarithromycin 500mg IV BD Facial cellulitis – odontogenic and other deep soft tissue infections (Adult) Co-amoxiclav 1.2g IV TDS Cefuroxime 1.5g TDS IV plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to take PO) If severe type 1 hypersensitivity (anaphylaxis): Teicoplanin 400mg once daily plus Gentamicin 5mg/kg/day plus Metronidazole (as above). Severe pre-septal cellulitis and ALL orbital cellulitis (Adult) Co-amoxiclav 1.2g IV TDS Cefuroxime 1.5g TDS IV plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to take PO) If severe type 1 hypersensitivity (anaphylaxis): Teicoplanin 400mg once daily plus Gentamicin 5mg/kg/day plus Metronidazole (as above). IV Clarithromycin - risk of phlebitis. Switch to PO as soon as possible Gentamicin – risks of nephrotoxicity and ototoxicity Gentamicin duration should be kept <5 days wherever possible – review results of cultures and switch antibiotics according to sensitivities In renal impairment (eGFR <60ml/min), Gentamicin can be replaced with Ciprofloxacin 400mg IV BD (500mg BD PO if able to take oral medications) Gentamicin – risks of nephrotoxicity and ototoxicity Gentamicin duration should be kept <5 days wherever possible – review results of cultures and switch antibiotics according to sensitivities In renal impairment (eGFR <60ml/min), Gentamicin can be replaced with Ciprofloxacin 400mg IV BD (500mg BD PO if able to take oral medications) Acute Parotitis Co-amoxiclav 1.2g IV TDS Clarithromycin 500mg IV BD plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to take PO) IV Clarithromycin - risk of phlebitis. Switch to PO as soon as possible Acute Mastoiditis Co-amoxiclav 1.2g IV TDS Cefuroxime 1.5g TDS IV plus Metronidazole 400mg PO TDS (500mg IV TDS if unable to take PO) If severe type 1 hypersensitivity (anaphylaxis): Teicoplanin 400mg once daily plus Ciprofloxacin 500mg PO BD plus Metronidazole (as above). In paediatric patients consider Cefuroxime and Metronidazole if patient has had Amoxycillin or Co-amoxiclav orally Acute Otitis media Consider 2 or 3 d delayed antibiotics. Amoxicillin 500mg PO TDS For 5 days Clarithromycin 250-500mg PO BD. For 5 days Malignant Otitis externa Piperacillin/ tazobactam 4.5g IV TDS D/W Microbiology Acute Rhinosinusitis Amoxicillin 500mg PO TDS (double dose if severe) For 7 days Doxycycline 100mg PO BD. If persistent infection: use agent to cover anaerobes Co-amoxiclav 625mg PO TDS OR add Metronidazole 400mg PO TDS to Doxycycline for 7 days Chronic Rhinosinusitis Clarithromycin 500mg oral BD for 2 weeks followed by Clarithromycin 250mg oral BD for up to 8weeks Consider Azithromycin or Doxycycline in patients not tolerating / allergic to Clarithromycin. Antibiotics for Surgical prophylaxis Review microbiology results Recommended as per EPOS-2012 (European Position Paper on Rhinosinusitis) Oral Equivalent (see Trust guideline on IV to oral switching) Procedure Antibiotic Alternative Mastoid Surgery/ Ossiculoplasty Septorhinoplasty/ Septal reconstruction Co-amoxiclav 1.2g IV (single dose) Co-amoxiclav 1.2g IV (single dose) *Cefuroxime 1.5g (single dose) plus Metronidazole 500mg IV (single dose) *Cefuroxime 1.5g (single dose) plus Metronidazole 500mg IV (single dose) Benzylpenicillin Penicillin V 500mg Cefuroxime plus Metronidazole Neck dissection Co-amoxiclav 1.2g-3doses IV (three doses) *Cefuroxime 1.5g plus Metronidazole 500mg IV (3 doses) Cefotaxime Co-amoxiclav 625mg, if no penicillin allergy Cefalexin 500mg plus Metronidazole 400mg if penicillin allergic (not type 1 hypersensitivity) No oral equivalent *Do not use cefuroxime if there is a history of type1 anaphylaxis. In such cases use: Teicoplanin 400mg (single dose) plus Gentamicin 160mg (single dose) plus Mertronidazole 500mg IV (single dose) Ceftriaxone IV antibiotic Piperacillin/ tazobactam Oral switch agent No oral equivalent No oral equivalent. Consider oral Ciprofloxacin for pseudomonas if sensitive. Malignant otitis externa –D/W Microbiology