Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Guidelines Applied to Practice
(GAP)
American College of Cardiology,
Puerto Rico Chapter
GAP
Acute Coronary Syndrome
American College of Cardiology
Puerto Rico Chapter
San Juan Intercontinental; December 12: José R. Rivera del Río MD
Casa del Médico, Mayaguez; December 13: Anibal Lugo MD
Casa del Médico, Ponce; December 14: José Gómez Rivera MD
GAP
Management of Patient With
Unstable Angina and
Non-ST-Segment Elevation
Myocardial Infarction
ACC/AHA Guidelines
AHA/ACC Guidelines for Secondary
Prevention for Patients with Coronary and
Other Atherosclerotic Vascular Disease:
2006 Update
Gregg C. Fonarow, MD and Sidney Smith Jr, MD on
behalf of the Secondary Prevention Writing Group
TABLE OF CONTENTS
GAP
I.
Introduction
Purpose
Organization
Overview of the ACS
II. Initial evaluation and management
Clinical Assessment
Early Risk Stratification
Immediate Management
III. Hospital care
IV. Coronary revascularization
V. Hospital discharge
VI. Special Groups
Purpose
GAP
Major cause of ED visit and hospitalization
– 1997: 5,315,000 ED visits for CP
Increased morbidity:
– Mortality in hospital: 2- 8%
– Recurrent MI in first year: 20%
– Recurrent AP in first year has a mortality of 43%
Exposition to various physician other than
cardiologists
These guidelines were made for the medical
personnel managing these conditions with the
intention of decreasing the related morbidity
ACC
GAP in Michigan: Reliability Science
and Mortality Benefit
Kim A. Eagle, MD
On behalf of the ACC GAP Steering Committee, the
Michigan GAP Collaborators, and Partners
383 Cardiologists
33 Hospitals
30 Businesses
20 Health Plans
10 Health Systems
60 Nurse Project Leaders
45 Physician Champions
GAP Key Elements
Patient
ACC
Tool Kit
•
•
•
•
•
Patients
Providers
Hospitals
Health
Coalitions
MPRO
Standing Orders
Critical Pathways
Patient Information
Patient Discharge Contract
Hospital Data
Key
Care
Priorities
Nurse
Doctor
AMI GAP Collaborative Model
(12 month time frame)
Participants (19 teams)
Prework
Develop
Grand
Framework
Rounds
& Changes
November
2001
Oversight
Team
P
Jan-Mar 2002 A
Phone
Conference
12/6/01
LS 1
Workshop
Planning
A
S
LS 2
March
Implementation
P
P
D
D
A
S
D
S
LS 3
LS 4
April
May
Monitoring
tool use
Remeasurement
LS 5
November
Results &
Debriefing
Supports
Email
Visits
Monthly Team Reports
Phone calls
Assessments
12/12/01
*© 2001 Institute for Healthcare Improvement, Modified by Cecelia Montoye, RN, MSN, CPHQ
GAP IN MICHIGAN
Comparison of the Medicare diagnosis code
410.xx from patient treated the year before the
GAP implementation.
Records were copied and forwarded to
DynKePRO’ Centers for CMS Clinical Data
Abstraction Center.
Comparison pre GAP and post GAP were done
Lesson V: QI Saves Lives!
Medicare Patients with AMI before
and after GAP
JACC 2005
40
35
30
25
Before
After
20
15
10
5
0
Hosp Mort 30d Mort
RRR 24%
P< 0.017
23%
0.001
1 yr Mort
13%
0.004
Eagle KA et al. JACC 2005;46:1242-48.
Applying Classification of Recommendations
and Level of Evidence
Class I
Class IIa
Class IIb
Class III
Benefit >>>
Risk
Benefit >> Risk
Additional
studies with
focused
objectives
needed
Benefit ≥ Risk
Additional
studies with
broad
objectives
needed;
Additional
registry data
would be
helpful
Risk ≥ Benefit
No additional
studies
needed
Procedure or
treatment
SHOULD
be performed
or
administered
IT IS
REASONABLE
to perform
procedure or
administer
treatment
Procedure or
treatment
MAY BE
CONSIDERED
Level A
Multiple (3-5) population risk strata
evaluated (Multiple RCT’s)
General consistency of direction and
magnitude of effect
Level B
Procedure or
treatment
should NOT
be performed
or
administered
SINCE IT IS
NOT
HELPFUL
AND MAY BE
HARMFUL
Limited (2-3) population risk strata
evaluated (Limited RCT’s)
Level C
Very limited (1-2) population risk strata
evaluated (General consensus)
DEFINITION
GAP
UNSTABLE ANGINA (UA)
One of the Acute Coronary Syndromes (ACS)
Presents an AP lasting more than 20 minutes
Without S-T elevation in the EKG
Without cardiac enzymes elevation
Expressed as:
– a. New onset
– b. At rest
– c. Progressing effort angina
– d. Post myocardial Infarction (MI)
– e. After a revascularization process.
DEFINITION
GAP
NSTEMI is expressed similar to UA
but elevation of cardiac enzymes is
present. Usually ends as NQMI. Less
frequently as QwMI.
STEMI has the same clinical picture
as a NSTEMI but presents S-T
elevations in the EKG. Usually ends
as QwMI and less frequently as NQMI.
Hamm Lancet 358:1533,2001
Presentation
Ischemic Discomfort
Working Dx
Acute Coronary Syndrome
Davies MJ
Heart 83:361, 2000
ECG
No ST Elevation
NSTEMI
Biochem.
Marker
Final Dx Unstable Angina
ST Elevation
25%
10%
Myocardial Infarction
NQMI
Qw MI
PATHOGENESIS
GAP
Coronary artery narrowing caused by non
occluding thrombus on a disrupted
atherosclerotic plaque. Microembolization
explains the release of the markers.
(Most frequent)
Dynamic obstruction (spasm, Prinzmetal)
Severe narrowing
Arterial inflammation
Secondary UA (Increased demand)
GAP
The Matrix Skeleton of Unstable
Coronary Artery Plaque
Fissures in
the fibrous
cap
TM
Davies MJ. Circulation. 1996;94:2013-2020.
© 1999 Professional Postgraduate Services®
TABLE OF CONTENTS
GAP
I.
Introduction
Purpose
Organization
Overview of the ACS
II. Initial evaluation and management
Clinical Assessment
Early Risk Stratification
Immediate Management
III. Hospital care
IV. Coronary revascularization
V. Hospital discharge
VI. Special Groups
Clinical Assessment
GAP
Class I
– 1. Patients with possible ACS should not be
evaluated by telephone but referred to a
facility that allows evaluation by a physician
and record an ECG. (C)
– 2. Patients with suspected ACS with chest
discomfort at rest over 20 minutes,
hemodynamic instability or recent syncope
or presyncope should be referred to an ED
or a CPC. (C)
Early Risk Stratification
GAP
Class I
– 1. Patients with chest discomfort should
undergo risk stratification focused on anginal
Sx., physical findings, ECG findings and
biomarkers of cardiac injury. (C)
– 2. A 12 lead ECG should be done immediately
(in 10 min.) in ACS patients. (C)
– 3. Cardiac injury biomarkers should be done in
patients with ACS. Preferred Troponins. Other
options CK-MB. If in 6 hours no elevation need
at least another sample in 6-12 hours frame. (C)
Likelihood of CAD with increased
Risk of Death or Non Fatal MI
HIGH
MODERATE
LOW
ONE PRESENT:
NO “HIGH”;
MUST HAVE:
NO “HIGH”, “MOD.”;
MUST HAVE:
HX
HX: MI, CAD, SD,
age M >60, F > 70
Constant AP>20min;
Accelerated IHD Sx last
48 hrs
AP prolonged
>20min, rest,
resolved w/NTG
Increased AP(Freq,
severity, duration, or
at lower threshold)
PE
PE (w/IHD), new MR,
S3, new rales,
hypotension,
age > 75 y/o
Age > 70 years
GAP
ECG
MARKERS
AP,rest,ST >.05 mm, T T inversions > .2 mv
inversions > .2 mv
Pathological Q wave
LBBB, sustained VT
Elevation of TnI, TnT
or CK-MB
No elevations
Unchanged ECG or
normal ECG
No elevations
Search for non-coronary CP causes
GAP
Class I
Level C
GAP
PAINLESS MI
Old age
Females
Diabetes
Post coronary by pass surgery
Up to 33% in the National Registry of MI
{NRMI}-2 Study
GAP
Elderly:
Atypical presentation
Dyspnea 44%
Chest pain 33-60%
Sweating 14-23%
Syncope 18%
Confusion 8%
GAP
GAP
Troponins for Evaluation and
Management of ACS
Advantages
Risk Stratificaton
Sens/Spec > CKMB
Detect Recent MI
Selection of Rx
Detect Reperfusion
Disadvantages
Low sens. early (< 6h)
Repeat at 8-12 h if neg.
Limited ability to
detect late minor reinfarction
Recommendation
Useful as single test to efficiently Dx NSTEMI
Clinicians should familiarize themselves with Dx
“cutoffs” in local lab and other non CAD causes of its
elevation
Increase in CK-MB
GAP
IHD
Cardioversion
Miopericarditis
PCI
Fast tachycardia
Hypothyroidism
Small GI
RF
Dystrophies
Neuromuscular
diseases
Rhabdomyolisis
Tongue
Uterus
Diaphragm
Bladder
Malignancy
Increase in Troponins
GAP
IHD
Cardioversion
Pulmonary embolism
Tachycardia
Decompensated
heart failure
Ablation
Pericarditis
Sepsis
Myocardial trauma or
inflammation
Cold agglutinins
Aortic dissection
Immediate Management
GAP
Class I (see annexed chart)
– The Hx, PE, ECG and markers must be integrated to
assign patient in categories. (C)
– The patient with definitive or possible ACS must be
evaluated and observed in a special unit and
repeated ECG and markers after 6-12 hrs of Sx
repeated. (B)
– In suspected or present ACS with ECG and markers
non DX, a stress test (exercise or pharmacological)
should be performed in the ED or as outpatient
basis shortly after DH. (C)
Immediate Management
GAP
Class I (continued)
– Patient with definitive ACS, positive ECG or
markers, positive stress test or hemodynamic
instability must be admitted to hospital for further
management. (C)
– Patients with possible ACS and negative markers
unable to exercise should have a pharmacological
stress test. (B)
– Patients with S-T elevations and ACS must be
evaluated for urgent reperfusion therapy. (A)
Symptoms suggestive of ACS
Rapid Triage
Obtain Biomarkers
Non
Cardiac
Diagnosis
As Per
Other Dx
Assess 12 lead ECG
Chronic
Stable
Angina
Medical
Rx
Goal = 10 min
Possible
ACS
Definite
ACS
ASA
Antithrombin
Beta Blocker
ACS Protocol
Symptoms Suggestive of ACS
Possible ACS
Definite ACS
No ST elev.
Non dx ECG
Neg. card. markers
Observe
f/u studies
Neg
Neg
Outpt f/u
Stress
ST-Tw changes
Ongoing pain
Positive card markers
Hemodynamic abnl.
ST elev.
Evaluate for
reperfusion
Pos
Pos
Dx of ACS confirmed
Admit to hospital
Acute ischemia pathway
TABLE OF CONTENTS
GAP
I.
Introduction
Purpose
Organization
Overview of the ACS
II. Initial evaluation and management
Clinical Assessment
Early Risk Stratification
Immediate Management
III. Hospital care
IV. Coronary revascularization
V. Hospital discharge
VI. Special Groups
= Controversial issue
General Anti-Ischemic Therapy
GAP
Class I
– Bed rest and ECG monitoring. (C)
– NTG, sublingual or spray, followed by IV
Nitroglycerin for AP and relief of associated
symptoms. (C)
– Supplemental oxygen for cyanosis or
respiratory distress; finger pulse oximetry or
ABG to confirm adequate O2 saturation
(>90%) and continue oxygen in hypoxemic
presence. (C)
General Anti-Ischemic Therapy
GAP
Class I (continued)
– Morphine sulfate IV when AP can’t be controlled with
NTG or pulmonary congestion present. (C)
– Beta blocker therapy 2002 (IV first dose if ongoing
chest pain and no contraindications) followed by oral
administration. (B) Now (2004) its preferred oral MX (I)
and IV left for the pt with tachycardia or HTN. (IIa)
– In patients with ongoing AP and contraindications for
BB, diltiazem or verapamil can be used in absence of
contraindications or HF. (B)
– ACEI when BP have not be controlled after NTG and
BB and when patient in CHF or in ACS and DM. (B)
General Anti-Ischemic Therapy
GAP
Class IIa
– Oral long acting calcium antagonists for
recurrent ischemia in the absence of
contraindications and when BB and NTG
fully used. (C)
– An ACEI in all patients with ACS. (B)
– Intra-aortic balloon counterpulsation for
severe ischemia that is continuous or
recurrent or for hemodynamic instability
before or after coronary angiography. (C)
GAP
Antiplatelets and
anticoagulant therapy
Antiplatelets Therapy
GAP
Class I
– Give chewable ASA ASAP (If not allergic).
Initial dose of 162 - 325 mgr. Continue
indefinitely. (IA)
– Where no intervention is planned add
clopidogrel to ASA immediately and
continue it for one month (IA) at least or up
to 9 months (IB).
Aspirin Evidence: Dose and Efficacy
Indirect Comparisons of Aspirin Doses on Vascular Events
in High-Risk Patients
Aspirin Dose
No. of Trials
(%)
500-1500 mg
34
19
160-325 mg
19
26
75-150 mg
12
32
<75 mg
3
13
Any aspirin
65
23
0
Odds Ratio for
Vascular Events
P<.0001
0.5
Antiplatelet Better
Antithrombotic Trialists Collaboration. BMJ. 2002;324:71-86
1.0
1.5
2.0
Antiplatelet Worse
GAP
CLOPIDOGREL
Efficacy of Clopidogrel or Ticlopidine in
Reducing Coronary Events After Stenting
30-Day Major Adverse Cardiac Events
Trial
CLASSICS
TOPPS
Müller
CCF
Lenox Hill
Mayo
N. Memorial
S. Illinois
Wash. Hosp.
Wessex
Overall
Odds Ratio & 95% CI
N
Clopid. (%) Ticl. (%)
1020
1016
700
2369
2565
2827
1.3
2.6
3.1
5.7
2.4
0.6
0.9
3.5
1.7
8.9
3.8
1.6
1378
875
844
-361
13,955
0.8
2.1
2.0
3.4
2.0
2.2
1.4
0.5
5.2
3.9
OR=.73, P=.003
0.1
Clopidogrel
Better
1
Ticlopidine
Better
10
CLASSICS, Clopidogrel Aspirin Stent Intervention Coopoerative Study.
Bhatt DL, et al. J Am Coll Cardiol. 2002;39:9-14. (Copyright 2002, with permission from American College of Cardiology
Foundation)
CURE: Primary End Point
MI/Stroke/CV Death
Cumulative Hazard Rate
0.14
Placebo
+ Aspirin
0.12
0.10
0.08
Clopidogrel
+ Aspirin
0.06
20%
RRR
P=.00009†
(N=12,562)
0.04
0.02
0.00
0
3
6
9
Follow-up (mo)
12
CURE, Clopidogrel in Unstable Angina to Prevent Recurrent Ischemic Events; MI, myocardial infarction; CV, cardiovascular;
RRR, relative risk reduction.
† Plavix® [package insert]; 2002.
Adapted with permission (2002) from the Massachusetts Medical Society.
Yusuf S, et al. N Engl J Med. 2001;345:494-502.
CREDO: Benefits of Clopidogrel Plus Aspirin
to 1 Year Following PCI
CV Death, MI or Stroke
Combined Endpoint
Occurrence (%)
15
Placebo*
Clopidogrel*
11.5%
27% RRR
10
8.5%
P=.02
5
0
0
3
6
9
12
Months From Randomization
* Plus ASA and other standard therapies .
Steinhubl S, et al. JAMA. 2002;288:2411-2420. (Copyright 2002 American Medical Association. All rights reserved)
GAP
CLOPIDOGREL INITIAL DOSE
Clopidogrel
GAP
If surgery is contemplated hold
clopidogrel for 5-7 days.
In patients in whom PCI is planned add
clopidogrel and continue for at least for
one month at least (IA) or 9 months if no
risk of bleeding (IB)
GAP
Anticoagulant Therapy
Anticoagulant Therapy
GAP
Anticoagulation with subcutaneous
LMWH (Enoxaparin preferred, if no
surgery within 24 hours: IIA) or
unfractionated heparin (UFH) should be
added to antiplatelets therapy with ASA
and / or clopidogrel (IA)
Unstable Angina
Anti-coagulant Therapy
GAP
• Heparin
– recommendation is based on
documented efficacy in many trials of
moderate size
– meta-analyses (1,2) of six trials showed a
33% risk reduction in MI and death, but
with a two fold increase in major bleeding
– titrate PTT to 2x the upper limits of
normal
1. Circulation 1994;89:81-88
2. JAMA 1996;276:811-815
DATA FROM ESSENCE
• 54% of Heparin patients were still
outside the therapeutic range
12 to < 24 hours after drug
administration
• At 24 to < 48 hrs 48.7% of these
patients were still outside the
therapeutic range
D/MI/Urg Revasc (%)
TIMI Risk Score For UA/NSTEMI
50
40
•
•
•
•
•
•
•
Age > 65 y
> 3 CAD Risk Factors
Prior Stenosis > 50 %
ST deviation
> 2 Anginal events < 24 h
ASA in last 7 days
Elev Cardiac Markers
UFH
ENOX
40.9
30
20
10
28.8
26.2
4.7 3.5
13.214.1
19.9
14.9
3
4
20
8.3 8.6
0
0/1
2
5
6/7
Number of Risk Factors
Antman et al JAMA 284 : 835, 2000
GAP
GP IIb/IIIa BLOCKERS
GP IIb/IIIa Blockers
GAP
A platelet GP IIb/IIIa antagonist should be
administered, in addition to ASA and
heparin, to patients in whom
catheterization and PCI are planned.
The GP IIb/IIIa antagonist may also be
administered just prior to PCI (IA).
GP IIb/IIIa Blockers
GAP
Use of eptifibatide or tirofiban should be
considered, in addition to ASA, LMWH or
UFH, in patients with; persistent
ischemia, Troponins elevation, or any
other high risk features in which invasive
management is not planned (IIA).
GP IIb/IIIa Inhibitor During Medical Management
and After PCI: CAPTURE, PURSUIT, PRISM-PLUS
Post PCI
Medical Rx
10%
N=12,296
P=.001
Control
GP IIb/IIIa inhibitor
Death or MI
8%
N=2754
P=.001
8.0%
6%
4.9%
4.3%
4%
2.9%
2%
0%
0
+24 h
+48 h
+72 h
+24 h
+48 h
PCI
Boersma E, et al. Circulation. 1999;100:2045-2048. (with permission from Lippincott Williams & Wilkins, www.lww.com)
Meta-analysis of IIb/IIIa Inhibition in PCI for 30-Day
Mortality
IIb/IIIa Inhibitor Better
Placebo Better
N Ctrl
Trt
EPIC
EPILOG
RAPPORT
CAPTURE
Impact I
Impact II
Restore
Epistent
Espirit
ISAR 2
Admiral
Cadillac
2099
2792
483
1265
150
4010
2141
2399
2064
401
300
2082
1.7
0.7
2.1
1.3
2.0
1.1
0.7
0.6
0.6
4.5
6.6
2.3
1.5
0.4
2.5
1.0
1.0
0.7
0.8
0.5
0.4
2.0
3.4
1.9
Combined
0.73 (0.55,0.96) 20186
1.3
0.9
P=.024
0.1
1
10
OR
Kong DF, et al. Am J Cardiol. 2003;92:651-655. (Copyright 2003, with permission from Excerpta Medica, Inc.)
GAP
Unstable Angina
Anti-platelet Therapy
• Summary
– the four “P trials” (PRISM, PRISM-PLUS,
PARAGON, PURSUIT)
– all show reduction of death rate between
1.3% and 3.4% - in addition to the benefit of
aspirin
– useful in the management of patients with
unstable angina and MI without ST elevation
GAP
GP IIb/IIIa blockers
recommended when;
•Recurrent ischemia, despite meds
•Elevated Troponins I or T
•New ST-segment depression
•New CHF symptoms
•High-risk stress test findings
•LV dysfunction (EF <40%)
•Hemodynamic instability, sustained VT
ACC/AHA Class I Recommendations for
Antithrombotic Therapy*
Possible
ACS
Likely/Definite
ACS
Aspirin
Aspirin
+
SQ LMWH*
or
IV Heparin
Clopidogrel
Definite ACS With
Invasive Strategy
(Catheterization/PCI)
or High Risk (IIa)*
Aspirin
+
IV Heparin
+
IV Platelet
GP IIb/IIIa
Antagonist
Clopidogrel
* Class IIa: enoxaparin preferred over UFH unless CABG planned within 24 hours.
ACC, American College of Cardiology; AHA, American Heart association; ACS, acute coronary syndrome; PCI, percutaneous
coronary intervention; SQLMWH, subcutaneous low molecular-weight heparin; IV, intravenous.
Braunwald E, et al. J Am Coll Cardiol. 2000;36:970-1062.
Co adjuvant therapy
GAP
not recommended
Insulin and glucose
– DIGAMI and UKPDS: strict blood sugar control
decreased the mortality and incidence of MI
– GIPS: 30 days decreased mortality was seen in the
Killip class I patients using the insulin-glucosepotassium infusion
– Some consider the infusion in patients with IHDAMI and increased glucose levels
– BUT! In CREATE-ECLA JAMA 2005, Jan:
“There is no benefit to the addition of high dose
glucose-insulin-potassium infusion in patients
with ST segment elevation MI.” (20,201 patients)
Co adjuvant therapy
GAP
not recommended
Lidocaine prophylactically
Magnesium IV
HRT
ACC/AHA Guideline Summary
Risk Stratification post UA/NSTEMI
I
IIa IIb III
C
GXT for pts. w/o IHD/CHF symptoms /12- 24 hours @
C
GXT at intermediate risk Asx after 2-3 days @
B
Patients with low level capacity, limited motion,
COPD or @, do a pharmacological GXT
B
Angiography if instability or Sx persists
C
ECHO or MUGA for LV function if not scheduled for
angiography
@: Decide the GXT mode depending in the
ECG S-T changes, digoxin effect, LBBB,
delta wave and PPM presence.
Also depends on patient ability to perform
the test and the local expertise.
Braunwald E et al. J Am Coll Cardiol. 2002;40:1366-1474.
TABLE OF CONTENTS
GAP
I.
Introduction
Purpose
Organization
Overview of the ACS
II. Initial evaluation and management
Clinical Assessment
Early Risk Stratification
Immediate Management
III. Hospital care
IV. Coronary revascularization
V. Hospital discharge
VI. Special Groups
Invasive vs Conservative Strategy
for UA/NSTEMI
VANQWISH
2003
RITA-3
MATE
VINO
TIMI IIIB
TRUCS
Mortality p=0.001
N-F MI p=0.012
Re. hosp. p<0.0001
Conservative
No. of Patients: 920
ISARCOOL
TACTICSTIMI 18
FRISC II
Invasive
1674
7018
UA, unstable angina, NSTEMI, non–ST-segment myocardial infarction; ISAR, Intracoronary Stenting and
Antithrombic Regimen Trial; RITA, Randomized Intervention Treatment of Angina; VANQWISH, Veterans Affairs Non-QWave Infarction Strategies in Hospital study; MATE, Medicine vs Angioplasty for Thrombolytic Exclusions trial;
TACTICS-TIMI18, Treat Angina with Aggrestat® and Determine Cost of Therpay with Invasive or Conservative Strategy;
FRISC, Fragmin during InStability in Coronary artery disease.
ACC/AHA Guideline Summary
Early Conservative and/or Invasive Strategies
I
IIa IIb III
Early invasive strategy in high-risk patients
with any of the following:
•
•
•
•
•
•
•
•
A
Recurrent ischemia, despite meds
Elevated troponin I or T
New ST-segment depression
New CHF symptoms
High-risk stress test findings
LV dysfunction (EF <40%)
Hemodynamic instability, sustained VT
Prior CABG, PCI within 6 months
Either strategy in low- to moderate-risk patients
without contraindications to revascularization
B
C
Early invasive strategy for pts with repeated ACS
and without high-risk features or ongoing ischemia
EF=ejection fraction.
Braunwald E et al. J Am Coll Cardiol. 2002;40:1366-1474.
ACC/AHA Guideline Summary
CABG in patients post UA/NSTEMI
I
IIa IIb III
A
Significant LM disease
A
Three vessel disease and EF < 50%
A
Two vessel, LAD prox., w LVEF< 50 or ischemia in test
C
Repeat CABG for X’s SVG stenosis (Esp. LAD)
B
CABG w LIMA in MVD pts and RX DM
Braunwald E et al. J Am Coll Cardiol. 2002;40:1366-1474.
ACC/AHA Guideline Summary
PCI in patients post UA/NSTEMI
I
IIa IIb III
A
Pts. w MVD w suitable CAD and NL EF / w/o DM
A
IV GP IIb/IIIa in PCI
C
Focal SVG or multiple stenosis not for CABG
B
2-3 vessel CAD w LAD prox. / DM or dec. LVEF
with anatomy accessible for PCI
Braunwald E et al. J Am Coll Cardiol. 2002;40:1366-1474.
ACC/AHA Guideline Summary
PCI or CABG in patients post UA/NSTEMI
I
IIa IIb III
B
B
B
1-2 vessel CAD w/o LAD prox. but w large ischemic
territory at risk
1-2 vessel CAD w/o LAD prox. but w moderate
ischemic territory at risk
1 vessel disease with significant proximal LAD
Braunwald E et al. J Am Coll Cardiol. 2002;40:1366-1474.
TABLE OF CONTENTS
GAP
I.
Introduction
Purpose
Organization
Overview of the ACS
II. Initial evaluation and management
Clinical Assessment
Early Risk Stratification
Immediate Management
III. Hospital care
IV. Coronary revascularization
V. Hospital discharge
VI. Special Groups
AHA/ACC Guidelines for Secondary
Prevention for Patients with Coronary and
Other Atherosclerotic Vascular Disease:
2006 Update
Gregg C. Fonarow, MD and Sidney Smith Jr, MD on
behalf of the Secondary Prevention Writing Group
Cigarette Smoking Recommendations
Goal: Complete Cessation and No Exposure
to Environmental Tobacco Smoke
•Ask about tobacco use status at every visit.
•Advise every tobacco user to quit.
•Assess the tobacco user’s willingness to quit.
I IIa IIb III
•Assist by counseling and developing a plan for
quitting.
•Arrange follow-up, referral to special programs,
or pharmacotherapy (including nicotine
replacement and bupropion.
•Urge avoidance of exposure to environmental
tobacco smoke at work and home.
Blood Pressure Control Recommendations
Goal: <140/90 mm Hg or <130/80 if
diabetes or chronic kidney disease
I IIa IIb III
I IIa IIb III
Blood pressure 120/80 mm Hg or greater:
Initiate or maintain lifestyle modification: weight control,
increased physical activity, alcohol moderation, sodium
reduction, and increased consumption of fresh fruits vegetables
and low fat dairy products
Blood pressure 140/90 mm Hg or greater (or 130/80 or
greater for chronic kidney disease or diabetes)
As tolerated, add blood pressure medication, treating initially
with beta blockers and/or ACE inhibitors with addition of other
drugs such as thiazides as needed to achieve goal blood
pressure
Lipid Management Goal
I IIa IIb III
LDL-C should be less than 100 mg/dL
I IIa IIb III
Further reduction to LDL-C to < 70 mg/dL
is reasonable
If TG >200 mg/dL, non-HDL-C should be < 130 mg/dL*
*Non-HDL-C = total cholesterol minus HDL-C
Lipid Management Goals: NCEP
Risk Category
High risk:
CHD or CHD risk equivalents
(10-year risk >20%)
and
Very high risk:
ACS or established CHD
plus: multiple major risk
factors (especially diabetes) or
severe and poorly controlled
risk factors
Consider
Drug Therapy
LDL-C and non-HDLC Goal
Initiate TLC
<100 mg/dL
if TG > 200 mg/dL,
non-HDL-C should
be < 130 mg/dL
100 mg/dL
>100 mg/dL
(<100 mg/dL: consider drug
options)
<70 mg/dL,
non-HDL-C < 100
mg/dL
All patients
>100 mg/dL
(<100 mg/dL: consider drug
options)
ATP=Adult Treatment Panel, CHD=Coronary heart disease, LDL-C=Low-density lipoprotein cholesterol,
TLC=Therapeutic lifestyle changes
Grundy, S. et al. Circulation 2004;110:227-39.
Lipid Management Recommendations
Assess fasting lipid profile in all patients, and within 24 hours of hospitalization for
those with an acute event. For patients hospitalized, initiate lipid-lowering medication
as recommended below prior to discharge according to the following schedule:
I IIa IIb III
If baseline LDL-C > 100 mg/dL, initiate LDL-lowering
drug therapy
I IIa IIb III
I IIa IIb III
If on-treatment LDL-C > 100 mg/dL, intensify LDLlowering drug therapy (may require LDL lowering
drug combination)
If baseline is LDL-C 70 to 100 mg/dL, it is reasonable
to treat to LDL < 70 mg/dL
When LDL lowering medications are used, obtain at least a 30-40% reduction in LDL-C
levels.
Lipid Management Recommendations
I IIa IIb III
If TG are 200-499 mg/dL, non-HDL-C should be < 130
mg/dL
I IIa IIb III
Further reduction of non-HDL to < 100 mg/dL is
reasonable
I IIa IIb III
Therapeutic options to reduce non-HDL-C:
More intense LDL-C lowering therapy I (B) or
Niacin (after LDL-C lowering therapy) IIa (B) or
Fibrate (after LDL-C lowering therapy) IIa (B)
If TG are > 500 mg/dL, therapeutic options to prevent
pancreatitis are fibrate or niacin before LDL lowering
therapy; and treat LDL-C to goal after TG-lowering
therapy. Achieve non-HDL-C < 130 mg/dL, if possible
HMG-CoA Reductase Inhibitor: Secondary Prevention
Relationship between LDL Levels and Event Rates in Secondary Prevention Trials
of Patients with Stable CHD
Statin
30
4S
Placebo
Event (%)
25
4S
20
LIPID
15
LIPID
CARE
10
HPS
5
0
CARE
HPS
TNT (atorvastatin 10 mg/d)
TNT (atorvastatin 80 mg/d)
0
70
90
110
130
150
LDL-C (mg/dL)
170
190
210
LDL-C=Low density lipoprotein cholesterol; TNT=Treating to New Targets; HPS=Heart Protection Study;
CARE=Cholesterol and Recurrent Events Trial; LIPID=Long-term Intervention with Pravastatin in Ischaemic Disease;
4S=Scandinavian Simvastatin Survival Study.
LaRosa JC et al. NEJM. 2005;352:1425-1435
HMG-CoA Reductase Inhibitor: Secondary Prevention
Heart Protection Study (HPS)
20,536 patients with CAD, other occlusive arterial disease, or DM
randomized to simvastatin (40 mg) or placebo for 5.5 years
Event Rate Ratio (95% CI)
Baseline
LDL-C (mg/dL)
Statin
(n = 10,269)
Placebo
(n = 10,267)
<100
282 (16.4%)
358 (21.0%)
100–129
668 (18.9%)
871 (24.7%)
130
1083 (21.6%)
1356 (26.9%)
All patients
2033 (19.8%)
2585 (25.2%)
Statin Better
Statin Worse
0.76 (0.72–0.81)
P<0.0001
0.4
CAD=Coronary artery disease, CI=Confidence interval, DM=Diabetes mellitus,
HPS Collaborative Group. Lancet 2002;360:7-22
0.6
0.8
1.0
1.2
1.4
Physical Activity Recommendations
I IIa IIb III
Goal: 30 minutes 7 days/week,
minimum 5 days/week
Assess risk with a physical activity history and/or an
exercise test, to guide prescription
I IIa IIb III
Encourage 30 to 60 minutes of moderate intensity aerobic
activity such as brisk walking, on most, preferably all,
days of the week, supplemented by an increase in daily
lifestyle activities
I IIa IIb III
Advise medically supervised programs for high-risk
patients (e.g. recent acute coronary syndrome or
revascularization, HF)
Weight Management Recommendations
I IIa IIb III
Goal: BMI 18.5 to 24.9 kg/m2
Waist Circumference: Men: < 40 inches
Women: < 35 inches
Assess BMI and/or waist circumference on each visit and
consistently encourage weight maintenance/
reduction through an appropriate balance of physical activity,
caloric intake, and formal behavioral programs when indicated.
I IIa IIb III
I IIa IIb III
If waist circumference (measured at the iliac crest) >35 inches in
women and >40 inches in men initiate lifestyle changes and
consider treatment strategies for metabolic syndrome as
indicated.
The initial goal of weight loss therapy should be to reduce body
weight by approximately 10 percent from baseline. With success,
further weight loss can be attempted if indicated.
*BMI is calculated as the weight in kilograms divided by the body surface area in meters2.
Overweight state is defined by BMI=25-30 kg/m2. Obesity is defined by a BMI >30 kg/m2.
CV Risk Increases with Body Mass Index
Hazard Ratio
Hemorrhagic
Stroke
Ischemic
Stroke
Ischemic Heart
Disease
4.0
4.0
4.0
2.0
2.0
2.0
1.0
1.0
1.0
0.5
0.5
0.5
16 20 24 28 32 36
CV=Cardiovascular
16 20 24 28 32 36
Body Mass Index (kg/m2)*
Body mass index is calculated as the weight in kilograms divided by the
body surface area in meters2.
Mhurchu N et al. Int J Epidemiol 2004;33:751-758
16 20 24 28 32 36
Diabetes Mellitus Recommendations
Goal: Hb A1c < 7%
I IIa IIb III
Lifestyle and pharmacotherapy to achieve near
normal HbA1C (<7%).
I IIa IIb III
Vigorous modification of other risk factors (e.g.,
physical activity, weight management, blood
pressure control, and cholesterol management as
recommended).
I IIa IIb III
Coordinate diabetic care with patient’s primary
care physician or endocrinologist. )
HbA1c = Glycosylated hemoglobin
Antiplatelet Agents / Anticoagulation
Recommendations
Aspirin Recommendations
I IIa IIb III
I IIa IIb III
I IIa IIb III
Start and continue indefinitely aspirin 75 to
162 mg/d in all patients unless
contraindicated
For patients undergoing CABG, aspirin (100 to
325 mg/d) should be started within 48 hours
after surgery to reduce saphenous vein graft
closure
Post-PCI-stented patients should receive 325
mg per day of aspirin for 1 month for bare
metal stent, 3 months for sirolimus-eluting
stent and 6 months for paclitaxel-eluting stent
Clopidogrel Recommendations
Start and continue clopidogrel 75 mg/d
in combination with aspirin
I IIa IIb III
for post ACS or post PCI with stent
placement patients for up to 12
months
for post PCI-stented patients
>1 month for bare metal stent,
>3 months for sirolimus-eluting stent
>6 months for paclitaxel-eluting stent
*Clopidogrel is generally given preference over Ticlopidine because of a superior safety profile
Clopidogrel use post-PCI + stent: Mortality
n = 1501 drug-eluting stent (DES), n = 3165 bare-metal stent (BMS)
6
4
Cumulative
incidence
(%)
2
0
12
DES + CL
DES – CL
BMS + CL
BMS – CL
CL = clopidogrel
252
276
346
1644
18
Months
237
258
339
1627
24
230
244
331
1596
Eisenstein EL et al. JAMA. 2006;297.
4666 pts: 3156 BMS and 1501 DES. Duke Heart Center 2000-2006
Clopidogrel use post-PCI + stent:
Composite of death or MI
6
4
Cumulative
incidence
(%)
2
0
12
DES + CL
DES – CL
BMS + CL
BMS – CL
252
276
346
1644
18
Months
237
256
336
1621
24
230
240
327
1582
Eisenstein EL et al. JAMA. 2006;297.
4666 pts: 3156 BMS and 1501 DES. Duke Heart Center 2000-2006
Renin-Angiotensin-Aldosterone
System Blockers Recommendations
ACE Inhibitor Recommendations
I IIa IIb III
Use in all patients with LVEF < 40%,
and those with diabetes or chronic
kidney disease indefinitely, unless
contraindicated
I IIa IIb III
Consider for all other patients
ACE=Angiotensin converting enzyme, LVEF= left ventricular ejection fraction
ACE Inhibitor Evidence: Post MI with LVD or HF
AIRE
SAVE
Radionuclide
EF 40%
Probability of Event
TRACE
Clinical and/or
radiographic
signs of HF
Echocardiogram
EF 35%
0.4
0.35
Placebo
0.3
ACE-I
0.25
0.2
0.1
0.15
OR: 0.74 (0.66–0.83)
0.05
0
0
1
2
3
4
Years
ACE-I=Angiotensin converting enzyme inhibitors, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction,
OR=Odds ratio
Flather MD, et al. Lancet. 2000;355:1575–1581
ACE Inhibitor Evidence: CAD, CVD, PVD or DM
Heart Outcomes Prevention and Evaluation (HOPE) Study
CV death, MI, or
stroke (%)
9,297 patients with DM or vascular disease plus one additional CV risk factor, but
without HF or known LVSD randomized to ramipril (10 mg) or placebo for 5 years
0.20
Ramipril
0.15
Placebo
0.10
0.05
22% RRR, P<0.001
0.00
0
500
1000
1500
Days of Follow-Up
ACE-I=Angiotensin converting enzyme inhibitors, DM=Diabetes mellitus, CV=Cardiovascular, HF=Heart failure,
LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction
HOPE Investigators. NEJM 2000;342:145-153
Angiotensin Receptor Blocker
Recommendations
I IIa IIb III
Use in patients who are intolerant of ACE
inhibitors with HF or post MI with LVEF less
than or equal to 40%.
I IIa IIb III
Consider in other patients who are ACE
inhibitor intolerant.
I IIa IIb III
Consider use in combination with ACE
inhibitors in systolic dysfunction HF.
ACE=Angiotensin converting enzyme inhibitor, LVEF=Left Ventricular Ejection fraction, HF=Heart
failure, MI=Myocardial infarction
ARB Evidence: Post MI with LVD or HF
Valsartan in Acute Myocardial Infarction Trial (VALIANT)
All Cause Mortality
14,703 patients with post-MI HF or LVSD (EF <0.40) randomized to captopril (50 mg
three times daily), valsartan (160 mg twice daily), or captopril (50 mg three times
daily) plus valsartan (80 mg twice daily) over 2 years
0.4
Captopril
0.3
Valsartan
Valsartan and Captopril
0.2
0.1
Valsartan vs. Captopril: HR = 1.00; P = 0.982
Valsartan + Captopril vs. Captopril: HR = 0.98; P = 0.726
0.0
0
6
12
18
24
30
Months
EF=Ejection fraction, HR=Hazard ratio, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction,
RAS=Renin angiotensin system
Pfeffer M et al. NEJM 2003;349:1893-1906.
36
Aldosterone Antagonist
Recommendations
I IIa IIb III
Use in post MI patients, without significant
renal dysfunction or hyperkalemia, who are
already receiving therapeutic doses of an
ACE inhibitor and beta blocker, have an LVEF
< 40% and either diabetes or heart failure
*Contraindications include abnormal renal function (creatinine >2.5
mg/dL in men or >2.0 mg/dL in women) and hyperkalemia (K+ >5.0
meq/L)
ACE=Angiotensin converting enzyme inhibitor, LVEF=Left Ventricular Ejection fraction,
MI=Myocardial infarction
Aldosterone Antagonist: Post MI HF
and LVSD
Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and
Survival Study (EPHESUS)
All Cause Mortality (%)
6,644 patients with evidence of heart failure and LVSD (EF <0.40) after a MI randomized
to eplerenone (50 mg) or placebo for 16 months
Eplerenone
Placebo
25
20
15
10
5
0
RR = 0.85, P=0.008
0
6
12
18
Month
EF=Ejection fraction, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction
Pitt B et al. NEJM 2003;348:1309-21
24
30
36
b-blocker Recommendations
b-blocker Recommendations
I IIa IIb III
Start and continue indefinitely in all post MI, ACS, LV
dysfunction with or without HF symptoms, unless
contraindicated.
I IIa IIb III
Consider chronic therapy for all other patients with
coronary or other vascular disease or diabetes
unless contraindicated.
*Precautions but still indicated include mild to moderate asthma or chronic obstructive pulmonary
disease, insulin dependent diabetes mellitus, severe peripheral arterial disease, and a PR
interval >0.24 seconds.
MI=Myocardial infarction, HF=Heart Failure
b-blocker Evidence
Summary of Secondary Prevention Trials of b-blocker Therapy
Total #
Patients
RR (95% CI)
Acute
treatment
28,970
0.87 (0.77-0.98)
Secondary
prevention
24,298
0.77 (0.70-0.84)
Overall
53,268
0.81 (0.75-0.87)
Phase of
Treatment
0.5
CI=Confidence interval, RR=Relative risk
1.0
RR of death
b-blocker
Placebo
better
better
2.0
Antman E, Braunwald E. Acute Myocardial Infarction. In: Braunwald E, Zipes DP, Libby P, eds. Heart
Disease: A textbook of Cardiovascular Medicine, 6th ed., Philadelphia, PA: W.B. Sanders, 2001, 1168.
b-blocker Evidence: Post MI with
Left Ventricular Dysfunction
Proportion Event-free
Carvedilol Post-Infarct Survival Control in LV Dysfunction (CAPRICORN)
6,644 patients with LVEF <0.40 after a MI with or without HF randomized to
carvedilol or placebo for 24 months
1
0.95
n=975
0.9
Carvedilol
n=984
0.85
0.8
0.75
0.7
RR 0.77 P=.03
0
0.5
1
1.5
Years
The CAPRICORN Investigators. Lancet. 2001;357:1385–1390.
Placebo
2
2.5
Influenza Vaccination
I IIa IIb III
Patients with cardiovascular disease
should have influenza vaccination
TABLE OF CONTENTS
GAP
I.
Introduction
Purpose
Organization
Overview of the ACS
II. Initial evaluation and management
Clinical Assessment
Early Risk Stratification
Immediate Management
III. Hospital care
IV. Coronary revascularization
V. Hospital discharge
VI. Special Groups
GAP
Women
– should be managed similar as men (IB)
Elderly
– Consider health, comorbidities, cognitive status and
life expectancy (IC)
– Attention to pharmacokinetics and hypotensive
drugs (IB)
– Intensive therapy welcomed under close
observation (IB)
Diabetes Mellitus
– Is an independent risk factors (IA)
– CABG for MVD with LIMA (IB)
GAP
Variant AP
– Angiography to S-T elevations corrected by nitrates or
calcium blockers (IB)
– Patients with normal or non obstructive anatomy use
nitrates and /or Calcium blockers (IB)
– Provocative testing with non obstructing CAD (IIB)
Syndrome X
– Risk factors reduction (IC)
– Medical therapy with BB, Ca blockers and nitrates (IB)
GAP
POST CABG
– Same management as pre CABG patients (IC)
Lower threshold for diagnostic catheterization
– Imaging stress test better (IC)
– Repeat CABG for multiple lesions in the SVG
(IIC)
– PCI for focal SVG stenosis (IIC)
GAP
Cocaine related CAD
– NTG and calcium blockers for S-T
depression/elevation (IC)
– Angiography in AP not resolving with
nitroglycerine or calcium blockers. Add
lytics or PCI if needed (IC)
“I am convinced that we will save
more lives from cardiovascular
disorders over the next 10 years by
CONSISTENT USE of knowledge we
already have than by all the NEW
ADVANCES we discover…”
Kim Eagle, 2004
GAP
Management of Patient With
Unstable Angina and
Non-ST-Segment Elevation
Myocardial Infarction
ACC/AHA Guidelines
Guidelines Applied to Practice
(GAP)
American College of Cardiology,
Puerto Rico Chapter
JACC September 6, 2005:906-19
Clopidogrel Loading Dose
Clopidogrel Loading Dose
GAP
1. J Am Coll Cardiol September 5, 2006;48:931-8
In NSTE ACS clopidogrel more than 300 mgr (even 900 mgr)
provided faster onset of action, and greater reductions
in platelet activation during the first 24 hours.
2. J Am Coll Cardiol October 3, 2006;48:1339-45
In NSTE ACS 600 mgr loading of clopidogrel shows benefit
in platelet reactivity and clinical prognosis.
“A treatment gap between
therapy that is dictated by
evidence-based medicine and
therapy that occurs in practice
is not a deficit of knowledge;
rather, it is a deficit of
implementation.”
Sidney Smith, MD
Chief Scientific Officer
American Heart Association
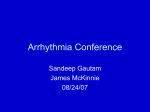
Use of Cardiac Markers in ACS
GAP
URL = 99th %tile of Reference Control Group
Multiples of the URL
50
20
Cardiac troponin after
“classical” AMI
(can last 10-14 days)
CK-MB after AMI
10
5
Cardiac troponin after
“microinfarction”
2
Upper reference limit
1
0
1
2
3
4
5
6
Days After Onset of AMI
Modified from:
ESC/ACC Comm “MI redefined…” JACC 36: 959,2000
7
8
Wu AH et al. Clin Chem 1999;45:1104.
Components of Secondary Prevention
Cigarette smoking cessation
Blood pressure control
Lipid management to goal
Physical activity
Weight management to goal
Diabetes management to goal
Antiplatelet agents / anticoagulants
Renin angiotensin aldosterone system blockers
Beta blockers
Influenza vaccination
JNC VII Lifestyle Modifications for BP Control
Modification
Recommendation
Approximate SBP
Reduction Range
Maintain normal body weight (BMI=18.524.9)
5-20 mmHg/10 kg weight
lost
Diet rich in fruits, vegetables, low fat
dairy and reduced in fat
8-14 mmHg
Restrict sodium
intake
<2.4 grams of sodium per day
2-8 mmHg
Physical activity
Regular aerobic exercise for at least 30
minutes on most days of the week
4-9 mmHg
Moderate alcohol
consumption
<2 drinks/day for men and <1 drink/day
for women
2-4 mmHg
Weight reduction
Adopt DASH
eating plan
BMI=Body mass index, SBP=Systolic blood pressure
Chobanian AV et al. JAMA. 2003;289:2560-2572
Exercise Evidence: Mortality Risk
Observational study of self-reported physical activity in 772 men
with established coronary heart disease
Light or moderate exercise is associated with lower risk
Wannamethee SG et al. Circulation 2000;102:1358-1363
Metabolic Syndrome: Risk of Developing DM
Diabetes Prevention Program (DPP)
Incidence of DM (%)
3,234 patients with elevated fasting and post-load glucose levels randomized to
placebo, metformin (850 mg twice daily), or lifestyle modification* for 2.8 years
Placebo
Metformin
Lifestyle modification
40
20
0
1
2
3
4
Lifestyle modification reduces the risk of developing DM
*Includes 7% weight loss and at least 150 minutes of physical activity per week
Knowler WC et al. NEJM 2002;346:393-403
Clopidogrel Evidence: ACS (Non-STEMI and UA)
Clopidogrel in Unstable Angina to Prevent Recurrent Events
(CURE) Trial
Rate of death,
myocardial infarction,
or stroke
12,562 patients with a NSTEMI-ACS randomized to daily aspirin (75-325 mg) or
clopidogrel (300 mg load, 75 mg thereafter) plus aspirin (75-325 mg) for 3-12
months (average 9 months)
0.14
Aspirin + Clopidogrel
Aspirin + Placebo
0.12
0.10
0.08
0.06
0.04
0.02
P<0.001
0.00
0
3
6
Months of Follow Up
NSTEMI-ACS=Non ST-segment elevation acute coronary syndrome
The CURE Trial Investigators. NEJM. 2001;345:494-502
9
12
Clopidogrel Evidence: Post PCI
Clopidogrel for the Reduction of Events during Observation
(CREDO) Trial
Risk of MI, Stroke,
or Death (%)
2,116 patients undergoing PCI randomized to 4 weeks of DAP* followed by
aspirin (75-325 mg) monotherapy vs persistent DAP* for 1 year
15
4 weeks of DAP
1 year of DAP
10
5
27% RRR, P=0.02
00
3
6
Months from Randomization
9
DAP=Dual antiplatelet therapy, PCI=Percutaneous coronary intervention, RRR=Relative risk reduction
*Dual antiplatelet therapy=Aspirin (75-325 mg daily) plus Clopidogrel (300 mg load followed by 75 mg daily).
Steinhubl S et al. JAMA 2002; 288:2411-20
12
b-blocker Evidence: Benefit in HF and LVSD
Study
Drug
HF
Severity
Patients
(n)
Follow-up
(years)
Mean
Dosage
Effects on Outcomes
CIBIS
Bisoprolol*
ModerateSevere
641
1.9
3.8
mg/day
All cause mortality
22% (p=NS)
CIBIS-II
Bisoprolol*
ModerateSevere
2,647
1.3
7.5
mg/day
All cause mortality
34% (P<0.0001)
BEST
Bucindolol*
ModerateSevere
2,708
2.0
152
mg/day
All cause mortality
10% (p=NS)
MERIT-HF
Metoprolol
succinate#
MildModerate
3,991
1.0
159
mg/day
All cause mortality
34% (P=0.0062)
MDC
Metprolol
tartrate*
MildModerate
383
1.0
108
mg/day
Death or Need for Tx
30% (P=NS)
CAPRICORN
Carvedilol
Mild
1,989
1.3
40
mg/day
All cause mortality
23% (P =0.03)
US Carvedilol
Carvedilol
MildModerate
1,094
0.5
45
mg/day
All-cause mortality†
65% (P=.0001)
COPERNICUS
Carvedilol
Severe
2,289
0.9
37
mg/day
All-cause mortality
35% (P =0.0014)
*Not an approved indication
†Not a planned end point.
#Not approved for severe HF or mortality reduction alone
Lesson I: Use of Tools Drives Improvement
100
80
85
94***
90***
91***
87*
81*** 82
Percent
71
73
76*
93***
92***
91***
86***
85**
84
87***
81
78*
77
74***
73
72 73
68***
68
60
51
40
20
0
ASA
Pre
Post
Post with tools
BB
LDL
Chol
ASA
BB
ACE
Smoking Chol
Counseling Rx
Dietary
Counseling
*p ≤ 0.05 **p ≤ 0.01 ***p ≤ 0.01
Eagle KA, et al. The Guidelines Applied in Practice (GAP)
Initiative to Improve MI Care in Michigan - Lessons Learned
from 3 Projects in 33 Hospitals. JACC 41:2003
Modified from Libby P
Circ 104:365,2001
Superficial
Erosion
GAP
Acute Coronary
Syndrome
Ruptured
Fibrous Cap
HMG-CoA Reductase Inhibitor: Secondary Prevention
Pravastatin or Atorvastatin Evaluation and Infection
Therapy (PROVE-IT)—TIMI 22 Study
4,162 patients with an ACS randomized to atorvastatin (80 mg) or
pravastatin (40 mg) for 24 months
Recurrent MI or
Cardiac Death
30
Atorvastatin
Pravastatin
25
16% RRR
20
15
10
5
P =0.005
0
3
6
9
12
15
18
21
24
27
30
Follow-up (months)
ACS=Acute coronary syndrome, CV=Cardiovascular, MI=Myocardial infarction, RRR=Relative risk reduction
Cannon CP et al. NEJM 2004;350:1495-1504
Anticoagulation Recommendations
I IIa IIb III
Manage warfarin to international normalized
ratio 2.0 to 3.0 for paroxysmal or chronic
atrial fibrillation or flutter, and in post-MI
patients when clinically indicated (e.g., atrial
fibrillation, LV thrombus.)
I IIa IIb III
Use of warfarin in conjunction with aspirin
and/or clopidogrel is associated with
increased risk of bleeding and should be
monitored closely
ACE Inhibitor Evidence: CAD
European Trial on Reduction of Cardiac Events with
Perindopril in Stable Coronary Artery Disease (EUROPA)
13,655 patients with CAD and presumed normal left ventricular function
randomized to perindopril (8 mg) or placebo for 4.2 years
Cardiovascular death (0.86; 0.72-1.03)
Non-fatal MI (0.78; 0.20-0.90)
Cardiac arrest (0.54; 0.20-1.47)
Combined endpoint (0.80; 0.71-0.91)
0
0.5
Favors Perindopril
1
1.5
2
Favors Placebo
ACE-I=Angiotensin converting enzyme inhibitors, CAD=Coronary artery disease, CV=Cardiovascular,
MI=Myocardial infarction
EUROPA Investigators. Lancet 2003;362:782-788
ACE Inhibitor Evidence: CAD
Prevention of Events with Angiotensin Converting Enzyme
Inhibition (PEACE) Trial
8,290 patients with stable coronary artery disease and normal left ventricular
function randomized to trandolapril (4 mg) or placebo for 4.8 years
Primary End Point (%)*
30
Placebo
Trandolapril
25
20
15
10
5
0
0
1
2
3
4
5
6
Years After Randomization
*Includes death from cardiovascular causes, myocardial infarction, or coronary revascularization
PEACE Trial Investigators. NEJM 2004;351:2058-2068
ARB Evidence: Heart Failure
Candesartan in Heart Failure Assessment of Reduction in
Mortality and Morbidity (CHARM) Added Trial
2,548 patients with symptomatic HF and LVSD (EF <40%) randomized to
candesartan (32 mg) or placebo in addition to an ACE-I over 34 months
CV Death of
Hospitalization
for HF
50
Placebo
40
Candesartan
30
20
10
HR 0.85, p=0.011
0
0
1
2
Years
3
3.5
ACE-I=Angiotensin converting enzyme inhibitors, ARB=Angiotensin receptor blockers, EF=Ejection fraction, HF=Heart
failure, LVSD=Left ventricular systolic dysfunction, RAS=Renin angiotensin system
McMurray JJ et al. Lancet. 2003;362:767-71
ARB Evidence: Heart Failure
Candesartan in Heart Failure Assessment of Reduction in
Mortality and Morbidity (CHARM) Alternative Trial
2,028 patients with symptomatic HF, LVSD (EF <40%), and intolerance to ACE-I
randomized to candesartan (32 mg) or placebo over 34 months
CV Death of
Hospitalization
for HF
50
Placebo
40
Candesartan
30
20
10
HR 0.77 p=0.0004
0
0
1
2
Years
3
ACE-I=Angiotensin converting enzyme inhibitors, ARB=Angiotensin receptor blockers, EF=Ejection fraction, HF=Heart
failure, LVSD=Left ventricular systolic dysfunction
Granger CB et al. Lancet. 2003;362:772-777
Aldosterone Antagonist: Heart Failure
Randomized Aldactone Evaluation Study (RALES)
1,663 patients with NYHA Class III or IV HF and LVSD (EF <0.35) randomized
to spironolactone (25 mg) or placebo (50 mg) for 24 months
Survival (%)
1.00
Spironolactone
Placebo
.90
.80
.70
.60
.50
RR = 0.70, P<0.001
0
0
3
6
9
12 15 18 21 24 27 30 33
36
Months
EF=Ejection fraction, HF=Heart failure, LVSD=Left ventricular systolic dysfunction, NYHA=New York Heart Association
Pitt B et al. NEJM 1999;341:709-717
Secondary Prevention Conclusions
• Evidence confirms that aggressive
comprehensive risk factor management
improves survival, reduces recurrent events and
the need for interventional procedures, and
improves the quality of life for these patients.
• Every effort should be made to ensure that
patients are treated with evidence-based,
guideline recommended, life-prolonging
therapies in the absence of contraindications or
intolerance.
Likelihood of having CAD
HIGH RISK
MOD RISK
LOW RISK
GAP
ANY OF:
NO “HIGH”,
ANY OF:
NO “HIGH”,
“MOD.”, ANY OF:
Definitive AP:M<60,
F<70 or Probable
AP;M>60, F>70
CP, not AP
HX
Hx: MI, SD, CAD,
Classical AP,
AP:
M>60, F>70 Variant
AP
PE(w/IHD), new MR,
S3, new rales,
hypotension
Extracardiac
vascular disease,
Male, DM
Chest pain
reproduced by
palpation
New STE >.05 mv;
T inv. >.2 mv, W/ sX
Fixed Q waves;
Abn.new ST/Twaves
Normal ECG
T flat or inv
Elevation of TnI,
TnT (>.1) or CK-MB
No elevations
No elevations
PE
ECG
MARKERS
Aspirin Evidence: Secondary Prevention
Effect of antiplatelet therapy* on vascular events**
Category
% Odds Reduction
Acute myocardial infarction
Acute stroke
Prior myocardial infarction
Prior stroke/transient ischemic attack
Other high risk
Coronary artery disease
(e.g. unstable angina, heart failure)
Peripheral arterial disease
(e.g. intermittent claudication)
High risk of embolism (e.g. atrial fibrillation)
Other (e.g. diabetes mellitus)
All trials
*Aspirin was the predominant antiplatelet agent studied
**Vascular events include MI, stroke, or death
Antithrombotic Trialist Collaboration. BMJ 2002;324:71–86.
0.0
0.5
1.0
1.5
2.0
Antiplatelet better Control better
Enoxaparin preferred (IIa)
If no surgery in 24 hours
(IIa) Use eptifibatide or tirofiban should be considered, in addition to ASA,
LMWH or UFH; in patients with persistent ischemia, Ti elevations or any
Other high risk feature, in which invasive Mx is not planned.