Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
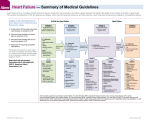
New CHF Patient in my Office: What Should I Do? Joseph Mishkin MD FACC Advanced Heart Failure, Transplantation and Mechanical Circulatory Support Disclosures • No disclosures Clinical Presentation • 38 year old man presents with 3 week history of abdominal discomfort, postprandial nausea, early satiety. Also reports fatigue, dyspnea and difficulty sleeping • Past Medical History – GERD – Irritable bowel syndrome – Appendectomy Additional History • Medications – Famotidine – Ibuprofen as needed • Social History Non smoker Occasional alcohol Office manager Father is medical malpractice attorney – Married, 2 children – – – – • Family History – – – – Father MI age 77 Mother healthy age 75 Brother healthy age 35 Sister healthy age 42 Physical Examination Appears tired, pale/ashen. No respiratory distress Temp 97.9 F HR 122 BP 92/60 mmHg Jugular venous distension present Lungs clear Tachycardic, 2/6 apical holosystolic murmur, third heart sound? • Abdomen soft, mild RUQ tenderness, no rebound/guarding • No edema, cool extremities • • • • • Next Step in Management? A) Referral to General Surgery to evaluate for cholecystectomy B) Referral to GI for EGD C) Rx for furosemide, carvedilol and digoxin; check some labs, follow up in 3 weeks D) Outpatient Cardiology referral for a stress test E) Inpatient admission for further evaluation and management How to Recognize Heart Failure? • A syndrome caused by cardiac dysfunction – Results from myocardial muscle dysfunction or loss – Characterized by left ventricular dilatation or hypertrophy – Neurohormonal and circulatory abnormalities leading to characteristic symptoms: Fluid retention Shortness of breath Fatigue, especially on exertion • Left untreated, usually progressive • Severity of clinical symptoms may vary substantially during course of the disease process and may not correlate with changes in underlying cardiac function HFSA Guidelines 2010 Braunwald. NEJM 2008 Clues From the History and Physical Examination Features that increase the likelihood of heart failure: • Presence of paroxysmal nocturnal dyspnea (greater than 2‐fold likelihood) • Presence of an S3 (11 times greater likelihood) • Bendopnea (shortness of breath when bending over) – Indicative of elevated filling pressures HFSA Guidelines 2010 Thibodeau, et al. JACC HF 2013 Definition of Heart Failure Classification Ejection Fraction Description I. Heart Failure with Reduced Ejection Fraction (HFrEF) ≤40% Also referred to as systolic HF. Randomized clinical trials have mainly enrolled patients with HFrEF and it is only in these patients that efficacious therapies have been demonstrated to date. II. Heart Failure with Preserved Ejection Fraction (HFpEF) ≥50% Also referred to as diastolic HF. Several different criteria have been used to further define HFpEF. The diagnosis of HFpEF is challenging because it is largely one of excluding other potential noncardiac causes of symptoms suggestive of HF. To date, efficacious therapies have not been identified. a. HFpEF, Borderline 41% to 49% These patients fall into a borderline or intermediate group. Their characteristics, treatment patterns, and outcomes appear similar to those of patient with HFpEF. b. HFpEF, Improved >40% It has been recognized that a subset of patients with HFpEF previously had HFrEF. These patients with improvement or recovery in EF may be clinically distinct from those with persistently preserved or reduced EF. Further research is needed to better characterize these patients. Updated ACC Guidelines 2013 Heart Failure Patient Evaluation • Assess clinical severity and functional limitation by history, physical examination, and determination of functional class* • Assess cardiac structure and function • Determine the etiology of HF • Evaluate for coronary disease and myocardial ischemia • Evaluate the risk of life threatening arrhythmia • Identify any exacerbating factors for HF • Identify co‐morbidities which influence therapy • Identify barriers to adherence *Metrics to consider include the 6‐minute walk test,NYHA functional class HFSA 2010 Practice Guideline Adapted from: New York Heart Association Classes • I: Ordinary physical • III: Comfortable at rest, activity does not cause but less than ordinary undue fatigue, activity causes fatigue, palpitation, or dyspnea palpitation, or dyspnea. (shortness of breath). • IV: Symptoms of cardiac • II: Comfortable at rest, insufficiency at rest. If but ordinary physical any physical activity is activity results in fatigue, undertaken, discomfort palpitations, or dyspnea. is increased. Objective Clinical Classification of Heart Failure Syndrome A L B C How do you determine stability in a patient with suspected HF? • • • • • History and physical Laboratory assessment Cardiac imaging Biomarkers HF Risk scores Signs and Symptoms Necessitating More Urgent Evaluation • • • • • • Hypotension Tachycardia Orthopnea, paroxysmal nocturnal dyspnea Syncope Unstable angina Unintentional weight loss/early satiety Biomarkers and Diagnosis Maisel, et al. NEJM 2002 Biomarkers and Prognosis ‐Val‐HeFT Investigators Prognostic value of changes in N‐ terminal pro brain natriuretic peptide in Val‐HeFT (Valsartan Heart Failure Trial) ‐Prognostic value of baseline plasma amino‐terminal pro‐brain natriuretic peptide and its interactions with irbesartan treatment effects in patients with heart failure and preserved ejection fraction: findings from the I‐PRESERVE trial Masson S., Latini R., Anand I.S., et al. J Am Coll Cardiol. 2008 Anand I.S., Rector T.S., Cleland J.G., et al. Circ Heart Fail. 2011 Risk Scores to Predict Outcomes in HF Risk Score Chronic HF All patients with chronic HF Seattle Heart Failure Model Heart Failure Survival Score CHARM Risk Score CORONA Risk Score Specific to chronic HFpEF I-PRESERVE Score Acutely Decompensated HF ADHERE Classification and Regression Tree (CART) Model American Heart Association Get With the Guidelines Score EFFECT Risk Score ESCAPE Risk Model and Discharge Score OPTIMIZE HF Risk-Prediction Nomogram Reference/Link http://SeattleHeartFailureModel.org http://handheld.softpedia.com/get/Health/Calculator/HFSS-Calc-37354.shtml http://www.heart.org/HEARTORG/HealthcareProfessional/GetWithTheGuidelinesHFStr oke/GetWithTheGuidelinesHeartFailureHomePage/Get-With-The-Guidelines-HeartFailure-Home- %20Page_UCM_306087_SubHomePage.jsp http://www.ccort.ca/Research/CHFRiskModel.aspx Less Complex Risk Prediction • Initial heart rate and systolic blood pressure predict outcomes in chronic heart failure • Heart rate > 100 • SBP < 100 Aranda JM Jr, et al. Clin Cardiol. 2007 McMurray. NEJM 2010 LCZ696? Back to Our Patient • 38 year old man presents with 3 week history of abdominal discomfort, postprandial nausea, early satiety. Also reports fatigue, dyspnea and difficulty sleeping – Dyspnea – Orthopnea and PND – Early satiety Physical Examination Appears tired, pale/ashen. No respiratory distress HR 122 BP 92/60 mmHg Jugular venous distension present Lungs clear Tachycardic, 2/6 apical holosystolic murmur, third heart sound? • Abdomen soft, RUQ tenderness • No edema, cool extremities • • • • • What’s the Next Step in Management ? A) Referral to General Surgery to evaluate for cholecystectomy B) Referral to GI for EGD C) Rx for furosemide, carvedilol and digoxin; check some labs, follow up in 3 weeks D) Outpatient Cardiology referral for an echocardiogram and stress test E) Inpatient admission for further evaluation and management Take Home Points • Presence of dyspnea on exertion, orthopnea and paroxysmal nocturnal dyspnea increase likelihood of heart failure • Presence of jugular venous distension and a third heart sound are concerning physical exam findings • Beware of atypical presentations (GI symptoms) • Rule out ischemia in patients with risk factors, history of angina • High risk features warrant inpatient evaluation Thank You A New PARADIGM in Heart Failure? • LCZ696 • In this double‐blind trial, we randomly assigned 8442 patients with class II, III, or • IV heart failure and an ejection fraction of 40% or less to receive either LCZ696 (at • a dose of 200 mg twice daily) or enalapril (at a dose of 10 mg twice daily), in addition • to recommended therapy. The primary outcome was a composite of death from • cardiovascular causes or hospitalization for heart failure, but the trial was designed • to detect a difference in the rates of death from cardiovascular causes. McMurray, et al. NEJM 2014 Noninvasive Cardiac Imaging I IIa IIb III Patients with suspected or new‐onset HF, or those presenting with acute decompensated HF, should undergo a chest x‐ray to assess heart size and pulmonary congestion, and to detect alternative cardiac, pulmonary, and other diseases that may cause or contribute to the patients’ symptoms. I IIa IIb III A 2‐dimensional echocardiogram with Doppler should be performed during initial evaluation of patients presenting with HF to assess ventricular function, size, wall thickness, wall motion, and valve function. I IIa IIb III Repeat measurement of EF and measurement of the severity of structural remodeling are useful to provide information in patients with HF who have had a significant change in clinical status; who have experienced or recovered from a clinical event; or who have received treatment, including GDMT, that might have had a significant effect on cardiac function; or who may be candidates for device therapy. Noninvasive Cardiac Imaging (cont.) I IIa IIb III Noninvasive imaging to detect myocardial ischemia and viability is reasonable in patients presenting with de novo HF who have known CAD and no angina unless the patient is not eligible for revascularization of any kind. I IIa IIb III Viability assessment is reasonable in select situations when planning revascularization in HF patients with CAD. I IIa IIb III Radionuclide ventriculography or magnetic resonance imaging can be useful to assess LVEF and volume when echocardiography is inadequate. Recommendations for Invasive Evaluation Recommendation COR LOE Monitoring with a pulmonary artery catheter should be performed in patients with respiratory distress or impaired systemic perfusion when clinical assessment is inadequate I C Invasive hemodynamic monitoring can be useful for carefully selected patients with acute HF with persistent symptoms and/or when hemodynamics are uncertain IIa C When coronary ischemia may be contributing to HF, coronary arteriography is reasonable IIa C Endomyocardial biopsy can be useful in patients with HF when a specific diagnosis is suspected that would influence therapy IIa C Routine use of invasive hemodynamic monitoring is not recommended in normotensive patients with acute HF III: No Benefit B III: Harm C Endomyocardial biopsy should not be performed in the routine evaluation of HF • Ouwerkerk W., Voors A.A., Zwinderman A.H.; Factors influencing the predictive power of models for predicting mortality and/or heart failure hospitalization in patients with heart failure. J Am Coll Cardiol HF. 2014;2:429‐436. • Pocock S.J., Ariti C.A., McMurray J.J., et al; Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J. 2013;34:1404‐1413. • Wang T.J., Gona P., Larson M.G., et al; Multiple biomarkers for the prediction of first major cardiovascular events and death. N Engl J Med. 2006;355:2631‐2639. • Levy W.C., Mozaffarian D., Linker D.T., et al; The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006;113:1424‐1433.