Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
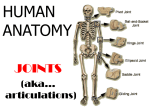
Introduction The shoulder complex Functional anatomy of the upper extremity The elbow and radioulnar joints The wrist and fingers Introduction Anatomical and functional characteristics of the joint Movement characteristics Muscular actions The shoulder complex Strength Conditioning Sport skills Injury The shoulder complex Sternoclavicular joint Acromioclavicular joint (AC joint) Scapulothoracic joint Sternoclavicular joint ◎This gliding synovial joint has a fibrocartilaginous. ◎The joint is reinforced by three ligaments and muscles : The interclavicular ligament The costoclavicular ligament -- the main support for the joint Glenohumeral joint (GH joint) The sternoclavicular ligament 1 Sternoclavicular joint Sternoclavicular joint Three degrees of freedom (3-DOF) The clavicle can move superiorly and inferiorly in movement referred to as elevation and depression. (30°~40°) The clavicle can move anteriorly and posteriorly via movement termed protraction and retraction. (30°) The clavicle can rotate anteriorly and posteriorly along its long axis through approximately 40°~50°. Acromioclavicular joint (AC joint) Acromioclavicular joint (AC joint) It is a small gliding synovial joint that is not present in all individuals. This joint that most of the movements of the scapula on the clavicle occur. Acromioclavicular joint (AC joint) Acromioclavicular joint (AC joint) This joint is reinforced with a dense capsule and a set of acromioclavicular ligaments lying above and below the joint. Close to the AC joint is the important coracoclavicular ligament, which assists scapular movements by serving as an axis of rotation. 2 Acromioclavicular joint (AC joint) Acromioclavicular joint (AC joint) Scapula protraction (abduction) and retraction (adduction) (30°~50°) –occurs as the acromion process moves on the meniscus in the joint and as the scapula rotates about the medial coracoclavicular ligament. Scapula elevation and depression (30°) – at acromioclavicular joint and is not assisted by rotations about the coracoclavicular ligament. The range of motion at the acromioclavicular joint for elevation and depression is approximately 30°. Scapula upward and downward rotation (60°) –clavicle moves on the meniscus in the joint and as the scapula rotates about the trapezoid portion of the lateral coracoclavicular ligament. Scapulothoracic joint The scapula interfaces with the thorax via the scapulothracic joint . This is not a typical articulation connecting The movements at the sternoclavicular joint are opposite to the movements at the acromioclavicular joint for elevation and depression, protraction and retraction. Glenohumeral joint (GH joint) Glenohumeral joint (shoulder joint) is a synovial ball-and-socket joint, offering the greatest range of motion and movement potential of any joint in the body. bone to bone. It is a physiological joint. Serratus anterior and subscapularis Glenohumeral joint (GH joint) Glenohumeral joint (GH joint) The joint contains a small, shallow socket called the glenoid fossa. It is only onefourth the size of the humeral head. The joint cavity is deepened by a rim of fibrocartilage referred to as the glenoid labrum. 3 Glenohumeral joint (GH joint) Ligament There is minimal contact between the glenoid fassa and the head of humerals, the shoulder joint largely depends on the ligamentous and muscular structures for stability. Ligament –Anterior side Ligament –Posterior side Joint support is provided The capsule - The coracohumeral ligament - Fibers of the subscapularis - The pectoralis major The glenoid labrum The glenohumeral ligament The joint is reinforced by: The capsule The glenoid labrum Fiber from the teres minor and infraspinatus Ligament Movement characteristics Superior aspect The glenoid labrum The coracohumeral ligament The supraspinatus Long head of the biceps brachii Inferior aspect Capsule Long head of the triceps brachii Flexion (~180°) - Be limited if the shoulder joint is external rotation. (in max. ER just only 30°). - Passive flexion and extension, there is accompanying anterior and posterior translation. Hyperextension (~60°) 4 Movement characteristics Internal rotation and external rotation Abduction (~180°) - Be limited by the internal rotation. (in max IR just only 60°) externally 90°, for a total of 180° of rotation. - Be limited by abduction Hyperadduction (~75°) Movement characteristics Horizontal flexion (~135°) Movement characteristics Past 30° of abduction or 45~60°of flexion, the ratio of glenohumeral to scapular movement become 5:4. Horizontal extension (~45°) - There is 5° of humeral movement for every 4° of scapular movement on the thorax. For the total range of motion through 180° of abduction or flexion, the glenohumeral to scapula ratio is 2:1. - Muscular actions Deltoid - Generates 50% muscular force for elevation of the arm in Abd or flexion - The deltoid increases with increases abduction - Most active through 90~180° The 180° range of motion is produced by 120° of glenohumeral motion and 60° of scapular motion. Muscular actions Rotator cuff - teres minors, subscapularis, infraspinatus, supraspinatus - Whole is capable of generating flexion or abd with about 50% of the force - In the early stages of abduction and flexion through 90°,the rotator cuff applies a force to the humeral head that keeps the head depressed and stabilized in the joint 5 Rotator cuff Muscular actions Deltoid and rotator cuff for the resting arm Trapezius and serratus anterior, which work together to abduction, elevation, upward rotation of scapula in arm flexion and abduction Levator scapulae and rhomboid, which assist in elevation of the scapula Muscular actions Shoulder girdle concentric adduction or extension (ex: swimming), creating these joint action are latissimus dorsi, teres major, sternal portion of the pectoralis major. The rhomboid muscle downward rotation the scapula and work with the teres major and the latissmus dorsi. The pectoralis minor depression and downward rotate the scapula. The middle and lower portions of the trapezius contribute to the retraction of the scapula with the rhomboid. Strength The adduction strength of the shoulder muscles is twice that fot abduction Muscular actions External rotation –infraspinatus and teres minor Internal rotation –subscapularis, latissimus dorsi, teres major, portions of the pectoralis major. Horizontal flexion –pectoralis major, anterior head of the deltoid Horizontal extension –infraspinatus, teres minor, posterior head of the deltoid. Conditioning Flexor and abductor - Flexibility - Manual resistance - Weight training Strength - Adduction – Extension – Flexion – Abduction – Internal rotation – External rotation 6 Conditioning Extensor and adductor - Flexibility - Manual resistance - Weight training Conditioning Shoulder gridle - Flexibility - Manual resistance - Weight training Sport skills - Freestyle swimming Conditioning Rotator cuff - Flexibility - Manual resistance - Weight training Sport skills -Activities of daily living Chair or wheelchair muscle Chair raise Long sit elbow flex Long sit elbow flex+abd Latissimus dorsi ☆ ☆☆ ☆☆☆ Pectoralis major ☆☆ ☆ ☆☆☆ Triceps brachii ☆☆☆ ☆☆☆ ☆☆☆ Sport skills -Overhand throwing pull-through (propulsion) recovery 7 Sport skills -Golf swing Injury ◎Trauma –external object ◎Repetitive joint actions –inflammatory The sternoclavicular joint –Strain, dislocate and Subluxation Clavicle –fracture Acromioclavicular joint –disruption, dislocate and Subluxation. Ectopic calcification (overuse), degeneration (cartilage). Injury Coracoid process –fracture Scapula –fracture, bursitis Shoulder joint –trauma, repeated overuse, dislocation, tearing the capsule or glenoid, soft tissue injuries, impingement syndrome, bicipital tendinitis… The elbow and radioulnar joints Ulnar-humeral joint Radiohumeral joint The elbow and radioulnar joints Ulnar-humeral joint Ulnar-humeral joint is the articulation between the ulna and the humeral and is the major joint to flexion and extension of the forearm. Trochlea, coronoid process, coronoid fossa, olecranon process, olecranon fossa… Radioulnar joint Medial and lateral epicondyles 8 Ulnar-humeral joint Ulnar-humeral joint Carrying angle –In the extended position, because of asymmetry in the trochlea. The carryint angle is measured as the angle between a line describing the long axis of the ulna and line describing the long axis of the humeral. From 10~25°. Radiohumeral joint Radioulnar joint The second joint participating in flexion Establishes movement between the radius and extension of the forearm is the radiohumeral joint. and the ulna in pronation and supination. 2 radioulnar articulations - Proximal – radial notch of ulna - Distal – ulnar notch of radius Radioulnar joint Ligament Collateral ligament –offer support and resistance to valgus stresses In the neutral position, the Annular ligament –important for support radius radius and ulna lie next to each other, but in full pronation the radius has crossed over the ulna diagonally. Interosseous membrane – connecting the radius and ulna. 9 Movement characterisitics Movement characterisitics The fully extended position the close- An extension movement is limited by the packed position for the ulnarhumeral joint. The proximal radioulnar joint is its closepacker position in the semiprone position. Flexion (~145°), dality action required 100140°. Passive flexion (~160°) Hyperextension (5~10°) Pronation (70°) Supination (85°) joint capsule and the flexor muscles, boneto-bone contact of the olecranon process. Flextion movement is limited by soft tissue, the posterior capsule, the extensor muscles, and the bone-to-bone contact of the coronoid process. Pronation/Supinarion is limited by the ligament, joint capsule, soft tissue. Muscular actions Muscular actions The elbow flexor - Biceps brachii, brachialis, brachioradialis, pronator teres, extersor carpi radialis - The strongest flexor of the group is the brachialis. - Biceps brachii is a two-joint muscle (flexion, supination, pronation) - Brachioradialis – rapid elbow flexion movement and against resistance The elbow extensor - Triceps brachii (long head, medial head, lateral head) is the strongest arm muscle of all. Pronator quadratus and pronator teres - Pronarot quadratus is the greater than teres Supinator Strength Conditioning Biceps brachii Flexibility Manual resistance - Weight training The flexor muscle group is almost twist as strong - as the extensors at all joint position, making us better pullers than pushers. The extensor muscle strength is greatest from a position of 90° of flexion. In semiprone elbow position : the maximum strength in flexion Is most commonly use in daily activities Pronation and supination strength greatest - - 10 Conditioning Conditioning Triceps brachii Pronator and supinator Flexibility - Manual resistance - Weight training - - Flexibility Manual resistance - Weight training - The wrist and fingers Radiocarpal joint Distal radioulnar joint The wrist and fingers Midcarpal and intercapal joint Carpometacarpal joint Metacarpophalangeal joint Interphalangeal joint 11 Carpals The wrist and hand Two rows of carpals - - Scaphoid (Most important carpals, support the weight of the arm. When wrist flexion , the midcarpal joint for 60%, the scaphoid for 40%.) Lunate Triquetrum Pisiform Trapezium Trapezoid Capitage (wrist extension, move quickly and close scaphoid) Hamate Carpometacarpal joint (CMC joint) Wrist deviation – these movement are The CMC joint providing the most movement for created as the proximal row of carpals glides over the distal now. The close-packed position for the wrist, is in a hyperextension position. - The close-packed position for the - the thumb, offers very little movement for the four fingers . At first ray, or thumb, is a saddle joint. Between the trapezium and the first metacarpal. For the thumb (CMC joint) Flexion/extension (50~80°) Abduction/adduction (40~80°) Rotation (10~15°) midcarpal joint is radial flexion. Metacarpophalangeal joint Metacarpophalangeal joint Metacarpophalangeal joint (MCP joint) of the four fingers are the condyloid (髁狀) joint. Movement in two plane (for four fingers): - flexion-extension (Flexion 70~90°, most flexion MCP joint for the thumb is a hinge (鉸鏈) joint allowing motion in only one plane. Flexion (30~90°) Extension (~15°) in the little finger and least in the index finger. Extension 25°, is limited wrist hyperextension and enhanced with the wrist flexion) - abduction-adduction (~20°, abduction is limited the fingers flexion, because the collateral ligament become tight) 12 Interphalangeal (IP) joint Muscular actions Most of the muscle acting at the wrist and Interphalangeal (IP) joint –thumb - Flexion (~90°) finger joint originate outside the hand in the region of the elbow joint. The wrist flexion - Flexor carpi ulnaris, flexor carpi radialis, palmaris longus - Medial epicondyle - Flexor carpi ulnaris (strongest flxor) and flexor carpi radialis are the most to wrist flexion Muscular actions Muscular actions Proximal interphalangeal (PIP) joint - Flexion (~110°) Distal interphalangeal (DIP) joint The wrist extension - Extensor carpi ulnaris, extensor carpi radialis longus, extensor carpi radialis brevis - Lateral epicondyle Ulnar deviation - Flexor carpi ulnaris - Extensor carpi ulnaris Radial deciation - Flexor carpi radialis - Extensor carpi radialis longus and brevis Finger flexion - Flexor digitorum profundus /superficialis - Medial epicondyle Lumbricales and Interossei (at MCP joint) - Flexor (in the palm) - Extensor (in the dorsal) Strength The wrist in ulnar flexion increases the strength output of the PIP and DIP flexor muscles to the greatest extent, followed by wrist hyperextension and lastly wrist flexion. The grip can be loosened if the wrist is put in a flexion position. 13 Conditioning Conditioning Wrist extensor and flexor Finger Flexibility - Manual resistance - Weight training - - Flexibility Manual resistance - Weight training Power grip - Precision grip Injury Injury Colles’ fracture - Distal end of the radius fracture Bennett’s fracture - Fracture to the thumb at the base of the first metacarpal Mallet finger Aculsion injury to the extensor tendon at the distal phalanx Boutonniere deformity By aculsion or stretching of the middle branch of the extensor mechanism, creates a stiff and immobile PIP articulation Jersey finger (Flexor Digitorum Profundus Rupture) Avulsion of the finger flexor, cause by forced hyperextension of the distal phalanx Trigger finger - 指的是指頭因為深屈肌(deep flexor)肌腱 (tendon),由於在指頭基部形成結節 (nodule),使得手指頭在彎曲而想伸直時會卡 在肌腱滑車(pulley),以致尾端指節無法完全 伸直;或者在伸直時會有阻力,形成類似扣板 機的情形,所以稱之為板機指 - Carpal tunnel syndrome Tenosynovitis is the inflammation of the fluid-filled sheath (called the synovium) that surrounds a tendon. Symptoms of tenosynovitis include pain, swelling, and difficulty moving the particular joint where the inflammation occurs. Carpal tunnel syndrome - is a medical condition in which the median nerve is compressed at the wrist, leading to paresthesias, numbness and muscle weakness in the hand. - 14 ~The end~ 15