Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
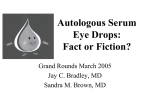
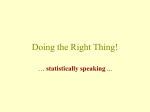
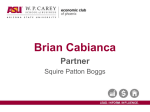
Clinical Science (1999) 97, 377–383 (Printed in Great Britain) Discrepancies between echocardiographic measurements of left ventricular mass in a healthy adult population Jenny A. DEAGUE*†, Catherine M. WILSON†, Leeanne E. GRIGG† and Stephen B. HARRAP* *Department of Physiology, University of Melbourne, Parkville, Victoria 3052, Australia, and †Department of Cardiology, The Royal Melbourne Hospital, Parkville, Victoria 3052, Australia A B S T R A C T Increased left ventricular (LV) mass is associated with increased cardiovascular morbidity and mortality. LV mass is commonly estimated from echocardiography according to the Penn or ASE (American Society of Echocardiography) conventions. No formal statistical test of agreement between these methods has been published. Therefore we compared M-mode echocardiographic LV mass estimates by the Penn and ASE methods in a normal adult population. M-mode echocardiographic tracings were obtained in 169 healthy volunteers and used to calculate LV mass using the Penn and ASE methods. Median values of the estimates were similar [Penn, 126 g (interquartile range 96–170 g) ; ASE, 129 g (105–164 g) ; P l 0.08] and were highly intercorrelated (r l 0.98, P 0.0001). However, the Bland–Altman analysis of agreement revealed significant inconsistencies between Penn and ASE LV mass values. The difference between Penn and ASE values was correlated significantly with heart size (P 0.0001), such that, for small hearts, the Penn LV mass was lower than the ASE LV mass ; in contrast, for large hearts, Penn estimates were greater than ASE values. In the upper 5 % of the LV mass distribution, the median value for the Penn LV mass index was 132.4 g/m2, compared with 116.5 g/m2 for ASE values (2P l 0.017). Thus the two most common methods of echocardiographic estimation of LV mass differ significantly at the upper and lower ends of the heart size distribution. These results have important implications for both cardiac research and clinical evaluation. INTRODUCTION Left ventricular (LV) hypertrophy is the single most important cardiovascular risk factor [1–7] after age. This is explained in part by the association of LV hypertrophy with high blood pressure, ischaemic heart disease and obesity. However, LV hypertrophy also appears to exert an independent contribution to cardiovascular risk. The association between LV mass and cardiovascular morbidity and mortality shows no threshold, being evident across the full range of heart sizes [7]. Furthermore, regression of LV hypertrophy as a result of antihypertensive medication has been associated with a reduction in cardiovascular events [8–10]. Estimation of LV mass in epidemiological studies, the diagnostic classification of LV hypertrophy and studies of the effects of therapeutic intervention depend on reliable and comparable measurement techniques. The measurement of LV dimensions in research and clinical practice is most commonly carried out using Mmode echocardiography, which is widely available, noninvasive and free of radiation. M-mode methods are used to record echocardiographic images of LV dimensions at the mitral–chordal junction. Three principal dimensions are measured : the LV internal diameter (LVID), the interventricular septum (IVS) and the posterior wall Key words : echocardiography, hypertrophy, left ventricle, M-mode, population. Abbreviations : ASE, American Society of Echocardiography ; IQR, interquartile range ; IVS, interventricular septum ; LV, left venticular ; LVID, LV internal diameter ; PW, posterior wall. Correspondence : Professor Stephen B. Harrap. # 1999 The Biochemical Society and the Medical Research Society 377 378 J. A. Deague and others (PW). Two measurement protocols are in common use. The American Society of Echocardiography (ASE) recommends that dimensions are measured from the leading edge to the leading edge of echocardiographic borders. This results in the inclusion of endocardial echoes from the IVS and PW, and the exclusion of endocardial echoes from the LVID. Subsequently, the Penn convention proposed measurements that exclude endocardial echoes from IVS and PW dimensions, but include endocardial echoes in measurement of the LVID. Therefore, for any given recording, the Penn convention gives larger cavity dimensions and smaller wall thicknesses than the ASE convention. Measurements of LVID, PW and IVS are used in formulae to estimate LV mass [11–17]. These formulae are based on the assumption that the left ventricle approximates a prolate ellipse. LV linear dimensions are cubed to provide volume terms. However, the way in which Cubic terms are derived and handled vary according to different formulae. Three basic formulae have been described, two of which use measurements made according to the ASE convention and one which uses measurements according to the Penn convention. An early Cubic formula based on geometric predictions and using measurements made according to the ASE convention was described by Rackley et al. [16] : 1.0996o[(2LVIDjIVSjPW) i0.5(IVSjLVIDjPW)#]k(LVID)$q. Subsequently, the arithmetic nature of the formula was simplified, and this version was recommended by the ASE : 1.04[(IVSjLVIDjPW)$k(LVID)$]. Later, using the Penn convention to measure dimensions, Devereux and co-workers [11,12] derived the Penn formula : 1.04[(IVSjLVIDjPW)$k(LVID)$]k13.6, by regression analysis using post-mortem LV weights. A further regression analysis against autopsy specimens [12] found that the original ASE formula overestimated autopsy LV weight, and a mathematical modification was suggested : 0.832[(IVSjLVIDjPW)$k(LVID)$]j0.6. This modified ASE formula and the Penn formula are both in common use to assess LV mass by M-mode echocardiography. Throughout this development, the agreement between different methods has been assessed simply by linear regression analysis and correlation coefficients. Close linear correlation has led to general acceptance that the Penn and ASE methods are more or less equivalent and can be used interchangeably [18–20]. However, such correlation analyses may obscure important differences # 1999 The Biochemical Society and the Medical Research Society between the estimates [21]. For this reason, Bland and Altman [21] recommended a method in which the differences between two measurements are compared with their average values. Such analyses provide information about agreement between methods that is not available from simple correlational analyses. The aim of the present study was to compare the estimates of LV mass derived according to the Penn, the ASE and the original Cubic formulae over a broad physiological range in a sample of the normal adult population. METHODS Subjects Subjects were drawn from the Victorian Family Heart Study, which is a population-based study of the familial patterns of cardiovascular risk factors. The total sample comprises 3000 volunteers from 828 families. Each family is composed of a minimum of a mother and father and one natural child. At the time of original recruitment, parents were aged between 40 and 70 years and offspring were between 18 and 30 years of age. We invited a random selection of families from the Victorian Family Heart Study to participate in this study of echocardiography and LV mass. Altogether, 180 volunteers agreed to participate in the study, and informed consent was obtained from all participants. These experiments were approved by the Ethics Committee of the Royal Melbourne Hospital. Echocardiography The M-mode echocardiographic study of the left ventricle was performed under cross-sectional control with a Hewlett-Packard 2500 or 1000 Echocardiography machine. Both Penn and ASE measurements of the LV dimensions were taken from M-mode strip chart recordings. The mean value of at least three measurements was determined for each LV dimension. LV mass was determined using three formulae : (a) the Penn formula o1.04[(IVSjLVIDjPW)$k(LVID)$]k 13.6q, using Penn convention measurements, (b) the ASE formula o0.832[(IVSjLVIDjPW)$k(LVID)$]j0.6q, using ASE convention measurements, and (c) the original Cubic formula (1.0996o[(2LVIDjIVSjPW)i 0.5(IVSjLVIDjPW)#]k(LVID)$q), using ASE convention measurements. A combined estimate of LV mass was calculated as the mean of the three individual estimates of LV mass. M-mode recordings and linear-dimension measurements were made by two of us (J. A. D. and C. M. W.). Measurements of the intra- and inter-observer errors (average difference divided by the average of the measurements), based on ten subjects, were 0.15 % and 1.3 % respectively for ASE measurements and 0.5 % and 2.5 % Echo measurements of left ventricular mass respectively for Penn measurements. Eleven of the 180 subjects were excluded because of technical difficulties with M-mode echocardiographic measurements. Data from the remaining 169 individuals were included and are presented in these analyses. Table 2 Univariate correlation matrix between estimates of LV mass by the three different methods These analyses were based on regression analyses using logarithmically transformed values ; * P 0.0001. Correlation coefficient Statistical analyses Summary data are expressed as the median and interquartile range (IQR), unless specified otherwise. For entry in parametric analyses, logarithmic transformation of LV mass values was used to normalize data distributions. Comparisons between groups were made using non-parametric and parametric analysis of variance. The linear association between variables was assessed using non-parametric and parametric regression analyses. The method of Bland and Altman [21] was used to assess agreement between different methods of LV mass estimation. Statistical significance was accepted when P 0.05. RESULTS The basic characteristics of the 169 participants are shown in Table 1. The combined estimates of LV masses showed a unimodal distribution, with a skew to the upper values (Figure 1), as reported previously in normal adult populations [2,7]. The Penn, ASE and Cubic LV mass Table 1 Basic characteristics of subjects Descriptive statistics are given as median (IQR). n Females Age (years) Weight (kg) Height (cm) Body surface area (kg/m2) Parents Offspring 96 52 57 (53–60) 75.5 (66–87) 167.5 (161–174.5) 1.87 (1.72–1.98) 73 41 29 (23–32) 69.5 (59.5–80) 169 (163–177.5) 1.77 (1.63–1.99) Figure 1 Frequency histogram of combined LV mass (g) for the subjects in this study See the text for a definition of combined LV mass. Penn ASE Cubic Table 3 Penn ASE Cubic 1.000 – – 0.980* 1.000 – 0.988* 0.999* 1.000 Pairwise differences between estimates of LV mass The values represent the medians of the differences between estimates of LV mass (column minus row). The values in parentheses represent the IQRs for these differences. Correlation coefficient Penn ASE Cubic Penn ASE Cubic 0 – – 1.9 (12.3) 0 – 6.4 (10.9) 4.2 (2.2) 0 estimations were normalized by logarithmic transformation (results not shown). Calculation of LV mass by each of the three formulae resulted in median values that were reasonably close : Penn, 126 g (IQR 96–170 g) ; ASE, 129 g (IQR 105–164 g) ; Cubic, 134 g (IQR 108–169 g). The nonparametric Friedman analysis of variance for related samples suggested that these differences were significant (χ# l 141.1, P 0.0001). The Wilcoxon rank test showed a significant difference between Cubic values and both ASE and Penn values. However, the difference between ASE and Penn values was not significant statistically (P l 0.08). Nevertheless, a strong linear correlation was demonstrated between the three calculated estimates of LV mass, as shown by the matrix with univariate correlation coefficients in Table 2. Despite the high degree of correlation, the differences between individual estimates using the different formulae varied widely (Table 3). These comparisons showed that the median of differences between LV mass estimated by the Penn and ASE methods was small (1.9 g). However, individual estimates of LV mass by the Penn method ranged from 54.2 g greater than to 29.0 g less than the corresponding ASE estimates. The magnitude and direction of these differences between LV mass estimates calculated using the different formulae appear to depend on the size of the heart. This was demonstrable on the Bland–Altman plots. For each subject, we plotted the individual combined LV mass against differences in LV mass derived using the two LV # 1999 The Biochemical Society and the Medical Research Society 379 380 J. A. Deague and others Figure 2 Bland–Altman plots of the differences in LV mass estimates as a function of combined LV mass Differences in LV mass are shown as measured by the Penn and ASE methods (top panel), the ASE and Cubic methods (middle panel) and the Penn and Cubic methods (bottom panel). mass formulae. Figure 2 (top panel) shows the differences between the Penn and ASE estimates of LV mass. This plot reveals a significant positive correlation (P 0.0001). Therefore, for smaller LV mass, Penn estimates were lower than ASE estimates, whereas for larger LV mass, Penn estimates were greater than ASE estimates (Figure 2, upper panel). When we examined subjects in the upper 5 % of the distribution for combined LV mass, we found that the median LV mass estimate by the ASE method was 241.5 g, compared with 268.1 g calculated by the Penn method. This difference was statistically sig# 1999 The Biochemical Society and the Medical Research Society nificant (Wilcoxon rank test ; 2P l 0.017). The same conclusions were true when the data were expressed as LV mass index, the values of which were 116.5 g\m# for ASE estimates and 132.4 g\m# for Penn measurements (2P l 0.017). When compared with LV mass derived by the Cubic formula, the Penn and ASE estimates showed distinctly different relationships. Figure 2 (middle panel) shows that the differences between Cubic and ASE estimates were small, and were distributed evenly across the range of combined LV size. In contrast, Figure 2 (bottom panel) shows that the differences between Cubic and Penn estimates varied substantially, and depended on LV size. Penn estimates were less than Cubic estimates for small hearts, and greater than Cubic estimates for large hearts. Two factors vary between these formulae : the arithmetic construction and the techniques for measuring dimensions. The similarity between the Cubic and ASE estimates, despite different mathematical constructions, may reflect an overriding importance of using the same dimensional measurements. To understand further the differences between LV mass estimates derived by the ASE and Penn methods, we examined the effect of standardizing dimensional measurements by entering into the Penn formula values for LVID, PW and IVS measured according to the ASE convention. This gave estimates of LV mass we refer to as PennASE. By comparing Penn and PennASE values, we studied the effects of different dimensional measurements in the same arithmetic formula. In this instance the median difference was large (20.1 g), with a wide IQR (63.4 g to k9.5 g). The Bland–Altman plot (Figure 3, upper panel) showed that the differences were significantly, but not closely, related to LV size, such that the difference between Penn and PennASE became larger as heart size increased. The comparison of PennASE with ASE estimates examined the effect of entering the same dimensional measurements in two different arithmetic formulae. By inspection of the mathematical construction of the Penn and ASE formulae, it is clear that when LVID, IVS and PW are the same (as they are in ASE and PennASE), the formulae reduce to linear equations that differ only by slope (1.04 for Penn ; 0.832 for ASE) and intercept (k13.6 for Penn ; 0.6 for ASE). Therefore the magnitude and variation of differences between PennASE and ASE estimates are dependent on simple mathematical considerations. As expected, the differences between these estimates were highly correlated over the range of LV mass (Figure 3, lower panel). The discrepancy between the Penn and ASE estimates is likely to be explained by the differences in both arithmetic structure and dimensional measurements. The greater slope of the Penn formula produces values of LV mass greater than those obtained with the ASE formula, Echo measurements of left ventricular mass lines of different slopes with a common point at approximately the mid-population value. DISCUSSION Figure 3 Bland–Altman plots of the differences in LV mass estimates measured by the Penn and PennASE methods (upper panel) and the ASE and PennASE methods (lower panel), as a function of combined LV mass Figure 4 Scatter diagram of individual values of LV mass estimated by the Penn ($) and ASE () methods plotted against combined LV mass and these differences increase with heart size (see Figure 3, lower panel). In addition, the use of Penn convention measurements results in smaller LV mass estimates than when using ASE convention measurements (see Figure 3, upper panel). The combined result of these effects is depicted in Figure 4, which shows the plots of Penn and ASE estimates of LV mass against combined LV mass, i.e. Echocardiographic measurement of LV mass is an important clinical and research technique. M-mode echocardiography is widely available, non-invasive and free of radiation. In comparison with magnetic resonance imaging (MRI), two-dimensional echocardiography and three-dimensional echocardiography, both the Penn and corrected ASE formulae have been anatomically validated using autopsy weight as a ‘ gold standard ’ [11,12]. In addition, both methods have demonstrated acceptable intra-observer and inter-observer variability [22]. Internationally, the ASE and Penn methods are both in common use, and there is no consensus on their relative merits or advantages. The choice in a particular laboratory is often arbitrary. It has been assumed that, because the average values of LV mass obtained by the Penn and ASE methods are similar and because individual values are highly intercorrelated, there is little difference between the estimates of LV mass obtained using the two methods. Some studies have incorporated both Penn and ASE data [18,19] and have used them interchangably [18]. Indeed, we were able to confirm high degrees of linear correlation between Penn and ASE estimates of LV mass. However, we found that this obscured substantial differences between estimates at the lower and upper ends of the population distribution of LV mass. For small hearts, Penn estimates were less than ASE estimates, while for large hearts Penn estimates were greater than ASE estimates. Our findings are relevant, therefore, to LV hypertrophy. Although definitions vary, LV hypertrophy is often categorized as the upper 5 % of the distribution of LV mass. When we examined this group, we found a significant difference of 27 g (approx. 10 %) in the estimates of LV mass by the Penn and ASE methods, and a significant difference of 16 g\m# (approx. 13 %) in values of LV mass index obtained using the two methods. Vasan et al. [7], in an analysis of the Framingham data, showed that even within the upper 5 % of LV mass there is a correlation between cardiovascular risk and increasing LV mass. Therefore, as cardiovascular risk increases, so does the discrepancy between Penn and ASE estimates of LV mass. These differences have important implications for the comparison of studies of LV hypertrophy that are based on different LV mass measurement criteria. Definition of a threshold value for LV hypertrophy is arbitrary, since LV mass is a continuous variable. There is no clear consensus concerning LV hypertrophy cut-offs, and various proposals have been based on the meanj2S.D. of # 1999 The Biochemical Society and the Medical Research Society 381 382 J. A. Deague and others the population distribution for LV mass index [2,7,18]. Data from the Framingham Study using the Penn criteria defined LV hypertrophy as an LV mass index of greater than 131 g\m# for men and 100 g\m# for women [23]. In the ASE technique used by De Simone and coworkers [19,20], LV hypertrophy was defined as an LV mass index of greater than 117 g\m# for men and 104 g\m# for women. The discrepancies in LV mass thresholds have been accepted largely without critical evaluation. Our findings suggest that part of this difference, particularly in males, is due to the divergence of estimates of LV mass at the upper end of the spectrum, rather than fundamental differences in the populations that were used to define these diagnostic thresholds. Unless diagnostic criteria are clearly defined in relation to a particular method of estimating LV mass, there is considerable potential for mis-labelling in relation to LV hypertrophy. Individual or group data derived by one method of estimating LV mass cannot be applied directly to studies in which other methods are used. This is relevant to LV hypertrophy diagnosis and therapy in relation to hypertension, valvular heart disease, ischaemic heart disease and obesity. However, our findings have equal importance at the other end of the population spectrum, and epidemiological comparisons should also take into account the methods used to estimate LV mass. Our findings raise further questions : how are these differences explained, and is one method more accurate than the other ? Our data provide no information on the accuracy of the various methods. However, our study offers some insight into an explanation for the discrepancy between estimates of LV mass by echocardiography. It has been suggested [15] that the simplification of the original Cubic formula was incorrect. However, we found that the values of LV mass derived by the Cubic and ASE formulae were very close across the range, despite differences in the mathematical structure of the two formulae. As both the Cubic and ASE formulae use the same measurements of cavity and wall dimensions, this observation suggests that physical dimensions, rather than arithmetic, are important. This view is supported by our observation that when different dimensional measurements were incorporated into the same arithmetic formula, larger discrepancies arose, as we observed in the Penn–PennASE comparison. The justification for particular M-mode echocardiographic methods has been based on linear correlations with LV weight measured at autopsy. To our knowledge, no Bland–Altman test of agreement between Penn or ASE estimates and the anatomical LV mass has been published. It seems that the differences between the Penn and ASE conventions have arisen as a result of empirical attempts to derive equations based on arbitrary measurement techniques that provide good correlation coefficients when compared with anatomical assessment of LV mass. The problem is that simple correlation is an # 1999 The Biochemical Society and the Medical Research Society imperfect assessment of agreement. The discrepancy between Penn and ASE estimates at low and high values of LV mass has obvious implications for clinical and research cardiology. It also seems necessary to use the Bland–Altman method to test agreement between all indirect methods of assessing LV mass and anatomical measurements. Until such data become available, it would seem sensible for individual echocardiography laboratories to use either the Penn or the ASE method and to determine the distribution of LV mass in a representative sample of their own population in order to determine relevant definitions of clinically important diagnoses, such as LV hypertrophy. In addition, multicentre studies need to standardize their use of formula, so as to avoid bias and confounding of analyses of LV mass. ACKNOWLEDGMENTS This work was supported by the Victorian Health Promotion Foundation and the National Health and Medical Research Council of Australia. We thank Ms. Margaret Stebbing, Dr. John Hopper (Australian NHRMC Twin Registry), Dr. Graham Giles (Collaborative Cohort Study, Health 2000), and the general practitioners and research nurses for their contributions to subject recruitment. REFERENCES 1 Levy, D., Garrison, R. J., Savage, D. D., Kannel, W. B. and Castelli, W. P. (1989) Left ventricular mass and the incidence of coronary heart disease in an elderly cohort. Ann. Intern. Med. 110, 101–108 2 Levy, D., Garrison, R. J., Savage, D. D., Kannel, W. B. and Castelli, W. P. (1990) Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N. Engl. J. Med. 322, 1561–1566 3 Casale, P. N., Devereux, R. B., Milner, M. et al. (1986) Value of echocardiographic measurement of left ventricular mass in predicting cardiovascular morbid events in hypertensive men. Ann. Intern. Med. 105, 173–178 4 Koren, M. J., Devereux, R. B., Casale, P. N., Savage, D. D. and Laragh, J. H. (1991) Relation of left ventricular mass and geometry to morbidity and mortality in uncomplicated essential hypertension. Ann. Intern. Med. 114, 345–352 5 Liao, Y., Cooper, R., Mensah, G. and McGee, D. (1995) Left ventricular hypertrophy has a greater impact on survival in woman than in men. Circulation 92, 805–810 6 Liao, Y., Cooper, R., McGee, D., Mensah, G. and Ghali, J. (1995) The relative effects of left ventricular hypertrophy, coronary artery disease, and ventricular dysfunction on survival among black adults. JAMA J. Am. Med. Assoc. 273, 1592–1597 7 Vasan, R., Larson, M., Levy, D., Evans, J. and Benjamin, E. (1997) Distribution and categorization of echocardiographic measurements in relation to reference limits. Circulation 96, 1863–1873 8 Verdecchia, P., Schillaci, G., Borgioni, C. et al. (1998) Prognostic significance of serial changes in left ventricular mass in essential hypertension. Circulation 97, 48–54 9 Koren, M. J., Ulin, R. J., Laragh, J. H. and Devereux, R. B. (1991) Reduction of left ventricular mass during treatment Echo measurements of left ventricular mass 10 11 12 13 14 15 16 of essential hypertension is associated with improved prognosis. Am. J. Hypertens. 4, IA (abstract) Muisesan, M. L., Salvetti, M., Rizzoni, D., Castellano, M., Donato, F. and Agabiti-Rosei, E. (1995) Association of change in left ventricular mass with prognosis during longterm antihypertensive treatment. J. Hypertens. 13, 1091–1095 Devereux, R. B. and Reichek, N. (1977) Echocardiographic determination of left ventricular mass in man : anatomic validation of the method. Circulation 55, 613–618 Devereux, R. B., Alonso, D., Lutas, E. et al. (1986) Echocardiographic assessment of left ventricular hypertrophy : comparison to necropsy findings. Am. J. Cardiol. 57, 450–458 Woythaler, N., Singer, S. L., Kwan, O. L., Meltzer, R. S., Reubner, B. and Bommer, W. (1983) Accuracy of echocardiography versus electrocardiography in detecting left ventricular hypertrophy : comparisons with postmortem mass measurements. J. Am. Coll. Cardiol. 2, 305–311 Devereux, R. B., Pini, R., Aurigemma, G. and Roman, M. J. (1997) Measurement of left ventricular mass : methodology and expertise. J. Hypertens. 15, 801–809 Wikstrand, J. (1997) Calculation of left ventricular mass in man – a comment. J. Hypertens. 15, 811–813 Rackley, C. E., Dodge, H. R., Coble, Y. D. and Hay, R. E. (1964) A method for determining left ventricular mass in man. Circulation 29, 666–671 17 Troy, B. L., Pombo, J. and Rackley, C. E. (1972) Measurement of left ventricular wall thickness and mass by echocardiography. Circulation 45, 602–611 18 Abergel, E., Tase, M., Bohlender, J., Menard, J. and Chatellier, G. (1995) Which definition for echocardiographic left ventricular hypertrophy ? Am. J. Cardiol. 75, 498–502 19 De Simone, G., Devereux, R., Daniels, S. R., Koren, M., Meyer, R. and Laragh, J. (1995) Effect of growth on variability of left ventricular mass : assessment of allometric signals in adults and children and their capacity to predict cardiovascular risk. J. Am. Coll. Cardiol. 25, 1056–1062 20 De Simone, G., Daniels, S. R., Devereux, R. B. et al. (1992) Left ventricular mass and body size in normotensive children and adults : assessment of allometric relations and impact of overweight. J. Am. Coll. Cardiol. 20, 1251–1260 21 Bland, J. and Altman, D. (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet i, 307–310 22 Devereux, R., Liebson, P. and Horan, M. (1987) Recommendations concerning use of echocardiography in hypertension and general population research. Hypertension 9 (Suppl. 2), II-97–II-104 23 Levy, D., Savage, D. D., Garrison, R. J., Anderson, K. M., Kannel, W. B. and Castelli, W. P. (1987) Echocardiographic criteria for left ventricular hypertrophy : the Framingham Heart Study. Am. J. Cardiol. 59, 956–960 Received 19 February 1999/4 May 1999; accepted 27 May 1999 # 1999 The Biochemical Society and the Medical Research Society 383