Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
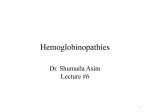
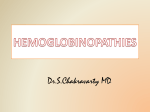
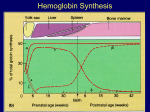
Hemolytic Anemia Part I FJ Albert, DO, DTM&H Hospital Medicine Lexington Medical Center West Columbia, SC Associate Professor Clinical Internal Medicine Edward Via College of Osteopathic Medicine Carolinas Campus Topic Summary • • • • • Anemia Hemolytic Anemia Hereditary Spherocytosis (HS) Elliptocytosis Paroxysmal Nocturnal Hemoglobinuria (PNH) • Pyruvate Kinase Deficiency Topic Summary • Glucose-6-Phosphate Dehydrogenase Deficiency (G6PD) • Thalassemias • Sickle Cell Disease • Disseminated Intravascular Coagulation (DIC) • Malaria • Henoch-Schonlein Purpura (HSP) Anemia • Defined by hemoglobin value • Hemoglobin <13.5 g/dL in women • Hemoglobin <12 g/dL in men Anemia • Mean Corpuscular Volume (MCV) – Size of a red blood cell – Normal 80-100 fL – Microcytic vs Macrocytic • Mean Corpuscular Hemoglobin Concentration (MCHC) – Concentration of hemoglobin within a red blood cell – Normal 32-36 g/dL – Hypochromic vs Hyperchromic Anemia Workup • • • • Serum iron Serum Total Iron Binding Capacity (TIBC) Serum ferritin Reticulocyte percentage/CBC smear – Normal reticulocyte percentage 0.5-1.5% Anemia Workup • Iron deficiency anemia – Low serum iron and high TIBC – Low serum ferritin • Anemia of chronic disease – Low serum iron and low TIBC – Normal or high serum ferritin Hemolytic Anemia • Elevated reticulocyte percentage • Elevated serum LDH • Elevated serum bilirubin (indirect predominance) • Low plasma haptoglobin Haptoglobin • RBC destruction releases hemoglobin in plasma • Free hemoglobin binds to haptoglobin • Hemoglobin-haptoglobin complex removed by liver • Plasma haptoglobin, therefore, markedly reduced with hemolytic anemia Red Blood Cells • Average survival is 110 to 120 days • Two modes of destruction – Increasing RBC age – Hemolysis due to processes independent of RBC age Hereditary Spherocytosis • Characterized by anemia, jaundice, and splenomegaly • Family history of hemolytic anemia Hereditary Spherocytosis • Alterations in genes that encode proteins responsible for unifying RBC inner membrane to the outer lipid bilayer • Spectrin deficiency most common protein deficiency seen in HS • Passage of RBCs through spleen progressive loss of RBC lipid layer acquired spheroid shapeultimate RBC hemolysis Spherocytosis • Complete Blood Count (CBC) – Anemia – Reticulocytosis – Low Mean Corpuscular Volume (MCV) – Increased Mean Corpuscular Hemoglobin Concentration (MCHC) – Increased Red Cell Distribution Width (RDW) – Spherocytes seen on CBC smear Spherocytosis • Direct and Indirect Antiglobulin (Coombs) serology is NEGATIVE with spherocytosis • POSITIVE Direct and Indirect Antiglobulin (Coombs) tests are associated with autoimmune hemolytic anemias Normal RBCs Spherocytes Spherocytes • Presence of spherocytes seen in – Hereditary Spherocytosis (HS) – Glucose-6-phosphate deficiency (G6PD) – Snake bites – Sepsis secondary to Clostridium – Microangiopathic hemolytic anemia Confirming Diagnosis of Hereditary Spherocytosis • Serologic testing – Eosin-5-maleimide binding test – Acidified glycerol lysis time or the cryohemolysis test (either one in combination with the Eosin-5-maleimide binding test) Hereditary Spherocytosis Treatment • RBC transfusions for symptomatic anemia • Folic acid (1 mg/day orally), to support erythropoiesis • Consideration of splenectomy – Eliminate hemolysis and anemia • Early splenectomy reduces risk of bilirubin gallstone formationreduces need for cholecystectomy later in life Splenectomy • ALL patients who undergo splenectomy (regardless of reason), are at increased risk for infections/sepsis from encapsulated bacteria • Proper immunization and/or antibiotic considerations for splenectomized patients – Hemophilus Influenzae B – Streptococcus Pneumoniae – Neisseria Meningitidis Elliptocytosis • Also known as hereditary ovalocytosis • Autosomal dominant transmission • Inherited disorder of one or more red blood cell membrane proteins Elliptocytosis • Spectrum of disease from asymptomatic (most cases) to life-threatening • Normal individuals have up to 5% elliptical RBC forms • Hereditary Elliptocytosis associated with 15-100% elliptical RBC forms Elliptocytosis • Diagnosed by peripheral smear abnormalities and other specialized laboratory tests and DNA testing • Treatment – Folic acid (1mg/day) orally – Red blood cell transfusions – Splenectomy for severe disease Paroxysmal Nocturnal Hemoglobinuria (PNH) • Defect in the glycosylphosatidyl-inositol (GPI) anchor of hemoglobin, due, in turn, to a genetic abnormality (PIG-A gene) • Clinical manifestations relate to hematopoietic function abnormalities Paroxysmal Nocturnal Hemoglobinuria (PNH) • Hemolytic anemia – Especially after viral or bacterial infections • Hypercoagulable state – Venous thrombosis, especially hepatic or other intraabdominal venous system • Bone marrow hypoplasia/aplasia • Progression to myelodysplastic syndrome (MDS) or acute leukemia Pyruvate Kinase Deficiency • Most common congenital NON- SPHEROCYTIC hemolytic anemia • Autosomal recessive transmission • Deficiency of erythrocyte Pyruvate Kinase enzymehemolysis • Mechanism of hemolysis not clear Pyruvate Kinase Deficiency • Severity of disease is highly variable • Some have life-threatening, transfusion requiring, hemolytic anemia from onset at birth • Some have fully compensated disease with minimal hemolysis Pyruvate Kinase Deficiency • Intrauterine PRBC transfusions in affected fetuses with severe anemia • Phototherapy, in addition to possible PRBC transfusions, for severe hyperbilirubinemia during neonatal period Pyruvate Kinase Deficiency • Oral folic acid (1 mg/day) is common • Splenectomy for severe disease – Reduces symptoms – Reduces frequency of PRBC transfusions • Hematopoietic cell transplantation if no benefit from splenectomy Glucose-6-phosphate dehydrogenase deficiency (G6PD) • Most common enzyme disorder of red blood cells in humans • X-linked transmission • Mostly asymptomatic, except following exposure to agents that cause hemolysis G6PD Deficiency • Glucose-6-phosphate dehydrogenase catalyzes first step of the hexose monophospate (HMP) shunt • HMP shunt protects RBCs from oxidative injury via NADPH production • Enzyme deficiency results in RBC oxidative injury G6PD Deficiency • List of more commonly used medications to avoid with known G6PD deficiency – Dapsone – Nalidixic Acid – Nitrofurantoin – Primaquine – Sulfamethoxazole (TMP-SMX; Bactrim/Septra) G6PD Deficiency • Foods notorious for hemolysis in G6PD deficiency – Fava beans • Others that MAY cause hemolysis with G6PD deficiency (individualized based on mutations) – Red wine, legumes, blueberries, tonic water – Henna (tattoo ink) Fear the Fava! Thalassemia • The major hemoglobin in NORMAL adults is hemoglobin A, consisting of one pair of alpha globin chains and one pair of beta globin chains Thalassemia • Thalassemia refers to a spectrum of diseases characterized by reduced or absent production of these pairs of alpha or beta globin chains • Definitive diagnosis of ALL thalassemias is by hemoglobin electrophoresis • Microcytic, hypochromic anemia – Low MCV and low MCHC, respectively Beta Thalassemia • Beta thalassemia is due to impaired production of beta globin chains • Associated with relative excess of alpha globin chains Beta Thalassemia • Beta thalassemia minor – Majority are asymptomatic – Ninety percent of hemoglobin is Hgb A • Beta thalassemia intermedia • Beta thalassemia major – Absent or markedly reduced beta chains – Hemoglobin A absent or markedly reduced – Only hemoglobin F and A2 present – Severe hemolytic anemia Alpha Thalassemia • Alpha thalassemia is due impaired production of alpha globin chains • Associated with relative excess of beta globin chains Alpha Thalassemia • A normal individual possesses four functional alpha globin genes • Alpha thalassemia reflects a loss of one, two, three, or four of these genes Alpha Thalassemia • Alpha thalassemia minima – Three normal alpha globin chain genes – Asymptomatic, with normal blood counts • Alpha thalassemia trait – Two normal alpha globin chain genes – Mild anemia (microcytic, hypochromic) Alpha Thalassemia • Hemoglobin H disease – One normal/functional alpha globin chain gene – Symptomatic at birth – Neonatal jaundice and life long hemolytic anemia • Hydrops fetalis and hemoglobin Barts – No inherited normal alpha globin chain genes – Not compatible with extrauterine life Sickle Cell Disease • Homozygous for hemoglobin S (HbSS) – Most severe form of disease – Results from substitution of valine, for glutamic acid, as the sixth amino acid of the beta globin gene Sickle Cell Disease • Heterozygous for both hemoglobin S and hemoglobin C (HbSC) • Heterozygous for hemoglobin S (HbS) – Sickle cell trait – Asymptomatic Sickle Cell Disease • Clinical hallmarks of disease – Vaso-occlusive processes (sickle cell pain crisis) – Red blood cell destruction via hemolysis Sickle Cell Disease • Exacerbations of disease usually occur secondary to some type of physiologic stressor – Infection – Volume depletion – Emotional stress/sleep deprivation Sickle Cell Disease • Clinical manifestations of disease – Anemia (hemolytic) – Reticulocytosis (3-15 reticulocyte %) – Unconjugated hyperbilirubinemia – Elevated serum LDH – Low serum haptoglobin – Sickled RBCs on peripheral smear – Howell-Jolly bodies on peripheral smear • Reflects hyposplenia from splenic infarctions Sickle Cell Anemia Sickled RBCs and Howell Jolly Bodies Sickle Cell Disease Treatment • Acute pain crisis treatment – Determine possible source of infection – Supplemental oxygenation – IVF with hypotonic fluid (e.g. ½ NS) is preferred – Pain control (narcotics are first line) Sickle Cell Disease • Chronic disease management – Folic acid (1mg/day) orally – Hydroxyurea – Multivitamin (MVI) – Calcium with vitamin D supplementation Sickle Cell Disease • Chronic disease management – Vaccination against encapsulated bacteria (Streptococcus pneumoniae, Hemophilus influenzae (HIB), and Neisseria meningitidis) – Vaccination against Hepatitis B, seasonal influenza, and H1NI influenza