Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
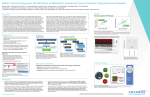
#3946 Stratification of Metastatic Colorectal Cancer Patients Using DNA and RNA Sequencing Fang Yin Lo1, Sharon Austin1, Kellie Howard1, Mollie McWhorter1, Heather Collins1, Amanda Leonti1, Lindsey Maassel1, Christopher Subia1, Tuuli Saloranta1, Nicole Christopherson1, Kathryn Shiji1, Shradha Patil1, Saman Tahir1, Sally Dow1, Evan Anderson1, Jon Oblad1, Kerry Deutsch1, Timothy Yeatman2, Steven Anderson3 and Anup Madan1 1Covance, Seattle, WA; 2Gibbs Cancer Center, Spartanburg, SC; 3Covance, Durham, NC Table 1. Frequency of Gene Fusion Events* B AstraZenica RAS signature gene expression from Affymetrix® microarray (log2) Select: - samples that have both FF and FFPE - about equal number from each Ras score group 0.08 6 RAS signature score Low High mutation call Figure 5. RAS signature scores versus mutation call. (A) Samples with KRAS mutation have significantly higher RAS signature scores compared with samples with wild type KRAS. (B) Combine information from gene expression, RAS signature score and mutation status. 55 samples for the pilot study Whole Transcriptome Analysis Exome Analysis RNA-seq Targeted Mutational Analysis Affymetrix® Microarray TruSight mutational panel Targeted Transcriptome Analysis Figure 2. Multi-platform comparison. Samples derived from the same 55 FFPE blocks were assayed across multiple platforms. The method design to combine RNA analysis (gene expression signature scores) with DNA analysis (i.e. mutation status) allows for comparison of RAS signature scores and overall gene expression from different platforms. CCDC125:MAGED2 CEACAM5:CEACAM7 CMTM8:CMTM7 DLG5:DLG3 LPHN2:LPHN3 PDE4DIP:RP11-353N4.1 RNF123:SERINC4 RP11-141M1.3:STARD13 RP11-680G10.1:GSE1 SAMD5:RP11-307P5.1 SF3B2:PHF17 SRPK2:KMT2E TFG:GPR128 VTI1A:RP11-57H14.3 Frequency 3 3 3 3 3 3 3 3 3 3 3 3 3 3 Table 2. Fusion Genes That Are Kinases Figure 6. The number of mutation versus KRAS status. KRAS mutant samples have significantly higher number of non synonymous mutations than KRAS wild type samples. 1000 p(aov)= 2.5e�02 500 mutation call Nanostring® Targeted RNA-seq A Distribution of number of gene fusion events B 0.16 6 Targeted RNASeq,FFPE Nanostring, FFPE Gene Expr Signature Score Quality Control and Data Normalization Affy, FF RNASeq-Acc, FFPE Affy, FFPE RNASeqrRNAdep, FFPE Targeted RNASeq,FFPE Nanostring, FFPE Ras Signature Score Calculation DNA and mutational information Correlation Analysis Regression Analysis Data Integration for Tumor Stratification Gene Mutation, e.g. KRAS/BRAF/NRAS Mutation Burden 0.12 4 0.08 p(aov)= 5.79e�05 0.04 2 0 0 10 20 30 Number of gene fusion events 40 low_fusion_num RNASeqrRNAdep, FFPE high_fusion_num RNASeq-Acc, FFPE Affy, FFPE Median = 17 RAS scores Affy, FF Figure 3. Flowchart for the analysis. 55 samples were gone through 5 different platforms for gene expression measurements – Affymetrix®, whole transcriptome RNA-Seq by two different library preparation methods, targeted RNA-Seq, and Nanostring®. Data went through quality control and normalization. For RAS score calculation, 18 genes were used based on previous study.5 count Data Source 1FF and 5 FFPE Datasets QC Presented at AACR 2016 Fusion 1500 KRAS_wt RNA Analysis KRAS_mut DNA Analysis RAS scores vs. Number of fusion events Figure 7. RAS signature scores and the number of gene fusion events. (A) Distribution of gene fusion events of all samples. Only high and medium confidence gene fusion events based on results from JAFFA7 were considered. (B) Samples with higher number of gene fusion events have significantly higher RAS signature scores (p<0.001). Gene Fusion Events Number of fusion events vs. RAS scores RNASeq.RNAAccess Affymetrix® 0.5 0.6 0.8 Nanostring® RNASeq.rRNAdepletion Affymetrix® 0.7 RNASeq.RNAAccess targeted RNAseq R=0.88 0.3 0.25 0.2 0.1 0.05 2. EGFR gene copy number as a prognostic marker in colorectal cancer patients treated with cetuximab or panitumumab: a systematic review and meta-analysis p(aov)= 9.97e�06 3. KRAS mutation status is predictive of response to cetuximab therapy in colorectal cancer. Lièvre A, Bachet JB, Le Corre D, Boige V, Landi B, Emile JF, Côté JF, Tomasic G, Penna C, Ducreux M, Rougier P, Penault-Llorca F, Laurent-Puig P. Cancer Res. 2006 Apr 15; 66(8):3992-5. 4. Loboda A et al. A gene expression signature of RAS pathway dependence predicts response to PI3K and RAS pathway inhibitors and expands the population of RAS pathway activated tumors. 5. BMC Medical Genomics 2010, 3:26Dry JR et al. Transcriptional Pathway Signatures Predict MEK Addiction and Response to Selumetinib (AZD6244). Cancer Res. 2010 Mar 15;70(6):2264-73. 0 0 0.05 0.1 0.15 0.2 RAS scores from RNASeq-RNAAccess 0.9 1. Gallagher DJ, Kemeny N. Metastatic colorectal cancer: from improved survival to potential cure. Oncology. 2010;78:237–248. 10 0 0.15 References 20 hi_rasscore RNASeq.rRNAdepletion 0.35 1 Pearson correlation coefficients Figure 4. Correlation of RAS signature scores between different platforms. (A) RAS scores calculated from multiple platforms are significantly correlated. All pairwise comparison has rho>=0.5 and p < 0.05. (B) Correlation of RAS scores calculated from RNA-seq and Affymetrix®. Scores between different platforms are highly correlated. Associated Gene Name Description ABR active BCR-related AKT3 v-akt murine thymoma viral oncogene homolog 3 BAZ1A bromodomain adjacent to zinc finger domain 1A BAZ1B bromodomain adjacent to zinc finger domain 1B BLK BLK proto-oncogene, Src family tyrosine kinase BLVRA biliverdin reductase A BMPR2 bone morphogenetic protein receptor type II CASK calcium/calmodulin-dependent serine protein kinase (MAGUK family) CDK6 cyclin-dependent kinase 6 CDK9 cyclin-dependent kinase 9 CLK3 CDC like kinase 3 DCLK2 doublecortin like kinase 2 FGFR1 fibroblast growth factor receptor 1 FGFR4 fibroblast growth factor receptor 4 INSR insulin receptor JAK2 Janus kinase 2 LATS1 large tumor suppressor kinase 1 LRRK1 leucine-rich repeat kinase 1 LRRK2 leucine-rich repeat kinase 2 LYN LYN proto-oncogene, Src family tyrosine kinase MAP3K7 mitogen-activated protein kinase kinase kinase 7 MAPKAPK2 mitogen-activated protein kinase-activated protein kinase 2 MAPKAPK5 mitogen-activated protein kinase-activated protein kinase 5 MARK3 MAP/microtubule affinity-regulating kinase 3 NEK9 NIMA-related kinase 9 PAK1 p21 protein (Cdc42/Rac)-activated kinase 1 PAN3 PAN3 poly(A) specific ribonuclease subunit PKN2 protein kinase N2 PLK2 polo-like kinase 2 RIOK2 RIO kinase 2 SCYL2 SCY1-like, kinase-like 2 SRPK2 SRSF protein kinase 2 TNIK TRAF2 and NCK interacting kinase 30 mid_rasscore Nanostring® 0.4 low_rasscore B RAS scores from Affymetrix® A Number of fusion events 40 targeted RNAseq 55 FFPE samples were selected from a cohort of 468 samples with matching FF samples. These 55 samples have about 1:1:1 ratio of high, medium and low RAS scores. Here we showed our capability to obtain RAS signature scores with concordant results using different platforms including whole transcriptome RNA-seq, Affymetrix® microarray (Affymetrix Inc.), targeted RNA-seq and Nanostring® (Nanostring Technologies, Inc.). We discovered that samples that have RAS activating mutations such as KRAS and BRAF have significantly higher RAS scores (p<0.001). On the contrary, expression of PD-L1 was significantly lower in tumor samples harboring mutations of genes such as MET, PTEN, NRAS, FBXW7 and GNAS. Kruskal-Wallis test showed that the expression of PD-L1 was significantly lower in samples with higher RAS signature scores (p<0.05). Furthermore, using the RNA-sequencing data, we were able to detect gene fusion events in these tumor samples. After filtering out low confidence results, a total of 730 gene fusion events were detected among the 55 tumor samples. While most of the gene fusion events were only detected once within the sample cohost, some were detected in multiple samples. For example, the fusion between KANSL1 and ARL17A was detected in 18 of the 55 samples. This is a relatively new discovery that had just started being mentioned in other cancer research institute reports.6 Other fusions that appeared multiple times include SAMD5 and SASH1. Interestingly, we discovered that significantly fewer fusion events were detected in samples with lower RAS signature scores than samples with higher RAS scores (p < 10-5). 1045 genes are involved in these fusion events. GO enrichment analysis shows that many of the cell cycle and phosphorylation associated pathways are significantly over-represented within these 1045 genes. Further analysis is being carried out for the implication of association between gene fusion events and RAS gene signature scores. Our analysis will lead to the development a combinatorial method for stratifying metastatic CRC patients. 18 16 9 7 6 5 5 5 5 5 4 4 4 3 3 KRAS mutation status vs. mutation number 2. Expression profile of immune checkpoint inhibitor target genes, such as PD1 and PD-L1. Methods and Results KANSL1:ARL17A SAMD5:SASH1 LMO7:EXT2 DPP4:FAP C10orf68:CCDC7 NOXA1:SLCO4A1 NR3C2:NR3C1 OSBPL2:OSBPL1A PRPF19:ABR USP7:SPARC PHF20L1:KIAA0753 RP11-123O10.4:GRIP1 WFDC10B:FA2H AKR1C1:AKR1E2 BIN2:MAN2A1 *Gene fusion events that occurred more than 3 times in the sample cohort. 55 FFPE colorectal cancer samples 1. RAS signature score based on the expression profile of 18 genes. This RAS signature score enables measurements of mitogen-activated protein/extracellular signal–regulated kinase (MEK) pathway functional output independent of tumor genotype. 3. DNA mutational profiles of genes such as KRAS, APC, BRAF and NRAS. Further, we explored potential gene fusion events in colorectal cancer tumor samples and discovered potential association between RAS gene signature score and the level of chromosomal rearrangements. Frequency 4 2 TP53 PIK3CA KRAS mutation status APC WT BRAF Mutant NRAS p(aov)= 3.04e�03 0.04 Fusion DS−56293 DS−52681 DS−60296 DS−51803 DS−53114 DS−60252 DS−54129 DS−52838 DS−51982 DS−51941 DS−54503 DS−40199 DS−54363 DS−54564 DS−33635 DS−48764 DS−52790 DS−51997 DS−53453 DS−49639 DS−70294 DS−54041 DS−48893 DS−53191 DS−52210 DS−47369 DS−54783 DS−49315 DS−48055 DS−58258 DS−52151 DS−48607 DS−58341 DS−54589 DS−67980 DS−56858 DS−44878 DS−50687 DS−56963 DS−54051 DS−51977 DS−51652 DS−48857 DS−56376 DS−52853 DS−51043 DS−52320 DS−56326 DS−53211 DS−49796 DS−50925 DS−51797 DS−49826 DS−60353 DS−67955 Samples with low Ras signature scores KRAS_wt Samples with medium Ras signature scores 0.12 KRAS_mut Samples with high Ras signature scores Figure 1. Colorectal cancer samples cohort selection strategy. The cohort was selected by filtering out colorectal cancer samples available as formalin-fixed, paraffinembedded (FFPE) and flash frozen (FF). Samples were then filtered for known RAS score obtained from Affymetrix® array. Known RAS scores are divided into 3 groups evenly: low (<33% percentile), medium (33%-66% percentile), high (>66% percentile). RASscores Ras signature scores calculated using FF samples 0 DUSP6 PHLDA1 PROS1 SERPINB1 MAP2K3 S100A6 TRIB2 ZFP106 SLCO4A1 DUSP4 ELF1 SPRY2 ETV5 KANK1 LZTS1 ETV4 FXYD5 LGALS3 Mean expression of all 18 genes log2 intensity KRAS mutation status vs. RAS scores 0.16 mutNum Colorectal cancer (CRC) is the third most common type of cancer in the United States. Although chemotherapy, radiation and targeted therapies can improve survival rates, recent studies have shown the potential benefit of immunotherapies to improve outcomes for patients with advanced CRC. Targeted therapies that use monoclonal antibodies (mAbs) to EGFR have been shown to benefit some CRC patients.1 Until recently, KRAS has been the only predictive biomarker for anti-EGFR therapy for metastatic CRC. However, 40% to 60% of patients with wild-type KRAS do not respond to anti-EGFR therapy. Therefore, to accurately predict patients’ responses to treatments and improve clinical outcomes, additional prediction and treatment methods are imperative. One of the many efforts to improve prediction for CRC patients’ responses to the anti-EGFR therapy is the development of gene expression based RAS signature scores for identification of RAS activated tumors independent of mutations in the KRAS gene.2,3 In addition to passive immunotherapy using mAb, there have been major advances in targeted active immunotherapy in other tumors, including checkpoint inhibitors and cancer peptide vaccines.4,5 In melanoma, there have been preliminary clinical findings indicating that combined targeted therapies and simultaneous active immunotherapies such as blockade of multiple immune checkpoints could promote therapeutic synergy and improve clinical outcomes for patients. In addition, chromosomal rearrangements have the potential to alter gene function in many different ways. Recently there have been major advances in detecting these chromosomal rearrangements. Fusion genes such as BCR-ABL and EML4-ALK have become targets for therapy in cancer. There is considerable effort being placed on combinatorial ways of tumor stratification to improve responses for these cancers. Similarly, since no single treatment can apply to all CRC patients, we aim to stratify patients using a combination of the following methods: A CRC sample cohort −6 −4 −2 Introduction Figure 8. Number of gene fusion events and RAS signature scores. Samples with lower RAS scores have significantly fewer gene fusion events detected than samples with higher RAS scores. Figure 9. Scatter plot of enriched GO cluster representatives. Multidimensional scaling is applied to the list of significantly enriched GO terms in fusion genes found in the CRC samples.6 6. http://newswise.com/articles/rutgers-cancer-researchers-examine-gene-fusion-and-treatment-implications-for-breast-cancer 7. Genome Medicine 20157:43. Covance is the drug development business of Laboratory Corporation of America Holdings (LabCorp). Content of this material was developed by scientists who at the time were affiliated with LabCorp Clinical Trials or Tandem Labs, now part of Covance.