Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
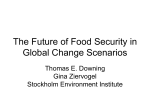
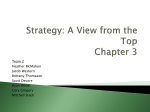
SCENARIO 1 Aspiration/#ankle Domain Criteria for High Rating Medical Expertise Discusses nature of original injury. Examiner’s form Explains need for urgent reduction. Outlines what has occurred. Explains consequences of aspiration and appropriate care. Communication Clear and concise language. Jargon free. Clearly acknowledges that a complication has occurred. Reassures mother that Paul will be recover. Appropriate use of body language. Allows for questions Health Advocacy Takes responsibility for arranging on going care Professionalism Shows respect and empathy. Professional appearance and conduct. Use of appropriate language tailored to Sarah’s understanding. SCENARIO 1 Candidate’s information You have just reduced a fracture/dislocation of the ankle of a 15 year old boy under sedation. An Xray is available for you ti view. Paul injured his ankle at school in a fall off some rocks. You were unable to contact his parents when he arrived and due to the nature of the injury, you decided to proceed with the reduction after discussing it with Paul. Unfortunately, Paul vomited and aspirated during the procedure. Whilst there is some evidence of aspiration on a chest Xray, Paul is comfortable and requiring 2L/min of nasal prong oxygen. The school managed to contact Paul’s mother, Sarah, and she has just arrived. Paul has given you permission to talk to his mum. Paul would like you to explain what has happened to his mother. You have 7 minutes to complete this task Domains assessed; Medical expertise Communication Professionalism Health Advocacy SCENARIO 1 Actor’s notes You are the mother of a 15 year old boy who sustained a fractured ankle in a fall at school. You are concerned, but reasonable and keen to find out how your son is. The doctor tried to contact you, but was unable to get hold of you. The school teacher managed to speak to you and told you which hospital your son is at. You have just arrived and the doctor looking after Paul is here to talk to you. Paul had a badly fractured and dislocated ankle. The fracture was putting the blood supply to the foot at risk and was very painful. The required treatment to restore normal blood flow and help reduce the pain is to realign the fracture/fix the dislocation under sedation. Paul suffered a complication, namely he vomited whilst sedated and aspirated (some of the vomit went into his lungs). He will need admission to hospital. Things to ask the doctor - Have them acknowledge that bit was a complication - ask directly “is that a complication?” if not volunteered by the doctor - Ask what treatment is needed for the aspiration if not volunteered by the doctor - Ask about the treatment for the ankle if not volunteered Please allow the candidate time to tell you what they want you to know, but please ask any questions that you feel are necessary. This should be as realistic as possible. Set up/Equipment 1 x actor Xray of fracture/dislocation of ankle SCENARIO 2 ICH family discussion Examiner’s form Domain Criteria for High Rating Medical Expertise Interpret CT to high standard and explain scan to daughter Recognises and explains very poor prognosis. Discussion about patient’s end of life wishes/advanced care plan - must focus on the patient’s, not the daughter’s wishes. Offer’s social work or other support (religious) Outlines comfort measures and why they are appropriate. Communication Introduces themselves to the daughter and confirms her name and that she is Mrs Smith’s daughter. Appropriate use of body language. Clear, concise and direct language used when discussing death/dying. Avoids use of euphemisms. Offers the daughter the opportunity to ask questions Health Advocacy Daughter will ask about neurosurgery and Intensive care - candidate to explain that either are unlikely to change the outcome, but should be happy to arrange consultation if daughter requests it. Advocate for the patient’s dignity and comfort. Professionalism Shows respect and empathy. Professional appearance and conduct. Use of appropriate, tactful language tailored to daughter’s understanding. SCENARIO 2 Candidate’s information An 84 year old female, Mrs Smith, presented to your ED from home after a collapse. Her GCS is 6. She is currently maintaining her own airway, so you elect to take her to CT without intubation. A CT brain shows a massive intracerebral haemorrhage. One of the nurses spoke to her daughter prior to the CT and she is waiting to discuss the CT result and her mother’s condition with you. Please discuss the CT result and what this means for Mrs Smith with her daughter. You have 7 minutes for this scenario. Domains assessed; Medical expertise Communication Professionalism Health Advocacy Scenario 2 Actor’s information You are the daughter of an 84 year old lady, Mavis Smith, who collapsed at home and was bought to hospital unconscious by ambulance. She has had a CT scan of her brain and you are meeting with the doctor to discuss how your mum is and the CT result. You are quite upset and you suspect the worst. The CT shows extensive bleeding inside the brain (a type of stroke) and it is unlikely your mother will survive. When the prognosis is explained to you, please ask about whether brain surgery or intensive care could help. If you are satisfied with the doctor’s explanation of why they would not, you can leave it there. If you are not happy, ask can you get the opinion of the neurosurgeon or intensive care specialist - you want to be sure that there really isn’t anything that can be done to change the outcome. You have never had a formal discussion about end of life care with your mother, but you believe that she would want to be kept comfortable if there was little chance of recovering and continuing to live a reasonably active life. Please ask any questions you feel are appropriate. This should be as realistic as possible. Some suggestions - How will you keep Mum comfortable? How do you know if she is in pain? Do you think she will die soon? What will happen now? CT scan of ICH SCENARIO 3 Oesophageal intubation Examiner’s form Domain Criteria for High Rating Medical Expertise Obtains relevant handover about the patient - including age, indication for intubation, drugs used, vital signs Recognizes oesophageal intubation. Asks about ETCO2/uses to confirm misplaced ETT. Removes ET tube and oxygenates patient (ventilation can be assessed by mannequin sensors and must be adequate to pass) Prepares for repeat attempt at intubation - positioning, in line stabilisation, equipment, drugs, fall back plan. Successful intubation. Confirms ET placement with ETCO2 and auscultation Addresses hypotension post intubation. Outlines plan for ongoing care - CT, Sedation, ventilator, control of ETCO2 and other strategies to prevent secondary brain injury. Communication Verbal clarity, conciseness, specificity. Confident, calm approach. Graded assertiveness to deal with registrar’s reluctance to step aside Controls flow communication and verbalizes plan to the team. Leadership & Clear leadership ability. Uses leadership skills to deal with registrar Management Maintains situational awareness Prioritizes tasks appropriately Teamwork & Collaboration Utilizes team members effectively Summarizes and updates team with plan appropriately Scenario 3 Candidate’s information This station involves a simulated patient. Please manage the patient exactly as you would in a real clinical setting. A registrar in your department is in the process of intubating a patient who has experienced a polypharmacy overdose. You are unaware of the patient, as there was no prehospital notification and you are busy with a sick child in the paediatric area. One of the senior nurses asks for you to come to the resuscitation bay as the registrar appears to be struggling. You have 15 minutes for this station. There will be 2 nurses and the registrar in the room, as well as a simulated patient. Any information about the patient’s condition that you cannot directly observe from the patient will be provided by the senior nurse on request. All treatment is to be carried out as if this is a real patient. You should assume leadership of the team and coordinate the management of the patient. Domains assessed; Medical expertise Communication Leadership and Management Teamwork and Collaboration Scenario 3 Actor/Confederate information The registrar has just intubated a 27 year old man who was found unconscious in a park. No trauma. It is suspected to be a polypharmacy overdose. The registrar has used thiopentone 400 mg and rocuronium 100mg. This will result in post intubation hypotension. Pre intubation vitals are P 105 GCS 7 BP 125/70 02 Sats 100% on NRBM One of the nursing staff is very concerned about the registrar’s intubation technique and has called out for your assistance. The oxygen saturations will begin to fall soon after the candidate enters the room. The registrar and airway nurse are just starting to tie the ETT in position as the candidate arrives. The ETT tube is in the oesophagus. Act as you normally would, but avoid giving the candidate direct prompts about management unless advised by the scenario leader by radio. Pointing out vital signs and clinical deterioration is expected and acceptable. The registrar is certain that the intubation is successful. They are reluctant to step aside despite falling saturations. “I saw the tube pass through the cords”. No ETCO2 was used to confirm the initial tube placement. Set up/equipment Use Oesophageal intubation scenario Difficult airway trolley Choice of induction and paralysis agents IV access already established 3 actors - 1 airway nurse, one circulation nurse, 1 registrar SCENARIO 4 Domain Difficult Airway Examiner’s form Criteria for High Rating Medical Expertise Recognises need for intubation. Recognises potential for difficult intubation and discusses options. Appropriate preoxygenation and positioning. Verbalises clear and appropriate plan for failed intubation and performs a pre intubation check. Does not persist at attempted intubation for a prolonged period. Follows plan once intubation fails (mannequin will be set to ensure direct laryngoscopy is impossible). Secures airway via iLMA or surgical airway if fails with iLMA Appropriate post intubation checks and care (ETCO2, sedation, vitals, auscultation etc) Communication Clear, concise communication. Closed loop. Confident, calm approach. Controls flow communication and keeps unnecessary communication to a minimum. Leadership & Clear leadership ability. Management Maintains situational awareness Prioritizes tasks appropriately Teamwork & Collaboration Utilizes team members effectively Communicates plan and summarizes management as appropriate SCENARIO 4 Candidate information This station involves a simulated patient. Please manage the patient exactly as you would in a real clinical setting. You are working at a small regional hospital Emergency Department. A 48 year old man with influenza pneumonitis has worsening type 1 respiratory failure. He is morbidly obese and is known to have a grade IV laryngeal view from a previous anaesthetic. HR 110 RR 32 BP 150/80 mmHg O2 Saturation 85 % 15L oxygen via NRBM. GCS 14 with equal and reactive pupils On examination he is obviously tiring and becoming more drowsy. Please mange the patient as you see appropriate. You will have the assistance of an airway nurse and a junior doctor. Another nurse who can provide you with clinical information not available from the patient will also be present and they will identify themselves as the confederate when you enter the room. You will have 15 minutes for this station Domains assessed; Medical expertise Communication Leadership and Management Teamwork and Collaboration Scenario 4 Actor/Confederate information Act as you normally would, but avoid giving the candidate direct prompts about management unless advised by the scenario leader by radio. Pointing out vital sign, clinical deterioration etc. is expected and acceptable. Set up/equipment Use anticipated difficulty airway scenario Difficult airway trolley Choice of induction and paralysis agents IV access already established NIV may be requested. Airway nurse, second doctor and Confederate nurse as a minimum. SCENARIO 5 Chest Pain Examiner’s form Domain Criteria for High Rating Medical Expertise Thorough history of the pain - Nature of the pain, Aggravating/relieving factors (including exertion, position, movement), radiation etc. Screening questions for pulmonary cause (pleuritic pain/cough/fever/SOB) Risk factors for PE and IHD. Screen for GORD symptoms Past medical history and medications. Recognises pericarditis as most likely diagnosis. Discusses appropriate further investigations on the basis that the clinical exam is normal. Communication Verbal clarity, conciseness, specificity. Avoids medical jargon. Obtain focused history in timely manner without pressuring/rushing the patient. Health Advocacy Clear explanation that informs patient of likely cause of chest pain and prognosis and what this means for the patient. Professionalism Shows respect. Professional appearance, demeanor and conduct. SCENARIO 5 Candidate’s information A 45 year old previously healthy man presents to the emergency department complaining of 2 weeks of chest pain Please take an appropriate history and review the provided ECG. After 7 minutes you will be asked to discuss the likely diagnosis and any alternate diagnoses with the patient. You will not be required to examine the patient. Vital sign are normal and a clinical examination was unremarkable. Domains assessed; Medical expertise Communication Health Advocacy Professionalism SCENARIO 5 Actor’s information You are 45 and called James/Jenny. You started to notice chest pain two weeks ago, and since then you have been having continuous chest pain with occasional exacerbations. This is very unusual for you. The pain is a dull constant ache over the left side of your chest. It does not get worse on exertion or movement. It is not worse on deep breathing but you think it might be worse when you lie down (do not offer this information unless asked). You are normally fit and well; non-smoker; no blood pressure or cholesterol problems. No family history of cardiac disease; no previous cardiac problems. No nausea or vomiting and no shortness of breath. No fever. No reflux symptoms. You have taken panadol, but this has only helped slightly. After the candidate has finished asking you questions and has looked at your ECG - ask them “what is causing the pain?” “Am I having a heart attack?” NEED ECG of pericarditis 1 actor SCENARIO 6 LP Examiner’s form Domain Criteria for High Rating Medical Expertise Checks clear indication for procedure (Post sudden onset of severe headache. CT at 8 hours post onset is normal) Establishes that informed consent has occurred. Ensures landmarks clearly identified, anatomy explained. Appropriately guides junior doctor through the technique. Scholarship & Teaching Permits the registrar to ask questions Teaching method that is structured and tailored to registrar’s understanding Communication Verbal clarity, conciseness, specificity Professionalism Shows respect Professional appearance, demeanor and conduct SCENARIO 6 Candidate’s instructions You are asked by a JMO to help them perform an LP on a 42 year old woman who presented with a severe headache. The JMO has never performed an LP before, but has assisted at several lumbar punctures previously. Informed consent has been obtained and the patient is set up ready for the procedure. Please guide the JMO through the entire process of performing the LP. The JMO will be doing the procedure and you will supervise and assist as needed. You have 7 minutes for this station Domains assessed; Medical expertise Scholarship and teaching Communication Professionalism SCENARIO 6 Actor’s instructions You are a junior doctor, who has never performed an LP before. You have assisted before and are very keen to do this LP yourself. The patient is a 42 year old female who is otherwise well. She presented after sudden onset of severe headache whilst at the gym. She is alert (GCS15). She had a CT performed 8 hours after the onset of the headache, which was normal. It is now 12 hours post onset of the headache. Informed consent has already been obtained. The patient is ready for the procedure to begin. You will perform the procedure as directed by the candidate. Once it is finished, you will ask the candidate what you should do if the xanthachromia is positive. If not told what tests to order, please ask the candidate “what tests should I order”. Set up/equipment LP mannequin LP needles/kit Syringe Local anaesthetic Sterile gloves/drapes/gowns/masks Actor x 1 SCENARIO 7 Examiner’s form Domain Criteria for High Rating Medical Expertise Checks clear indication for procedure and establish that informed consent has occurred. Discusses risks of the procedure with the JMO. Inspects CXR and identifies the haemothorax and the correct side of the patient. Ensures landmarks clearly identified, anatomy explained to JMO. Discusses analgesia/sedation/local anaesthesia Gives clear post procedure instructions – repeat CXR, analgesia, record ICC output, suction. Ensures that sterile technique is maintained. Scholarship & Teaching Permits registrar to ask questions Teaching method that is structured and tailored to registrar’s understanding Communication Verbal clarity, conciseness, specificity Professionalism Shows respect Professional appearance, demeanor and conduct SCENARIO 7 Candidate’s information A patient who has sustained a haemothorax in a fall from a ladder requires insertion of an ICC. You are to supervise and assist a junior ED trainee with the entire procedure. They will perform the procedure under your direct supervision. An Xray of the patient will be available in the room. The registrar has the patient prepared and ready to start. Informed consent has been obtained. The patient, a 54 year old man, is otherwise well and this is an isolated injury. Pulse 105 BP 115/70 Sat 99% on Hudson mask 8L/min GCS 15 Last eaten 4 hours ago You have 7 minutes for this station. Domains assessed; Medical expertise Scholarship and teaching Communication Professionalism SCENARIO 7 Chest tube insertion - Actor’s information You are a junior registrar working in the ED. You have asked one of the consultants to assist you in placing an ICC in a patient who has a haemothorax after a fall from a ladder. You will perform the procedure under their guidance. Consent has been obtained and the patient is positioned ready to go. All required equipment is set up. Act as you normally would in this situation. An Xray of the patient is available to view. Questions to ask: “Does the patient require IV antibiotics?” “Does the patient require sedation?” “Should I connect the chest tube to suction?” Equipment Thoracostomy mannequin LA/needles/syringe ICC Sterile drapes Gloves 1 actor SCENARIO 8 Candidate’s information A junior registrar in your department asks for assistance with a 47 year old man with a history of chronic liver disease secondary to excess alcohol consumption. He was brought to your emergency department by ambulance with acute confusion. The patient’s vital signs are GCS 12 Pulse 100 BP 120/65 RR 38 TEMP 35.7°C The registrar has performed a venous blood gas. Please assist them in interpreting the results. You will be assessed on your ability to interpret the VBG appropriately, given the clinical context and assist the registrar in reaching the appropriate interpretation. You will also be assessed on your ability as an educator, your professionalism and communication. You have 7 minutes to complete the task. Domains assessed; Medical expertise Scholarship and teaching Communication Professionalism Scenario 8 VBG result A 47 year old man with a history of chronic liver disease was brought to your emergency department by ambulance with acute confusion. The patient’s vital signs are GCS 12 Pulse 100 BP 120/65 RR 38 TEMP 35.7°C VBG pH 7.21 7.32-7.42 pCO2 14 35-45 mmHg HCO3 9 22-28 mmol/L BE -12.3 -2 to +2 Lactate 11 < 2 mmol/L Glucose 1.7 5-8 mmol/L Na 107 134-146 mmol/L K 4.7 3.4-5 mmol/L Cl 73 98-106 mmol/L SCENARIO 8 - Actor information You are a junior registrar in the department. You have just started seeing a 47 year old man with a history of chronic liver disease due to ETOH. He was brought to your emergency department by ambulance with acute confusion. The patient’s vital signs are GCS 12 Pulse 100 BP 120/65 RR 38 TEMP 35.7°C You have asked the consultant for assistance interpreting a VBG you have just performed. Introduce yourself. You will hand the VBG result to the candidate and ask them to help you interpret it. Some questions to ask (if not addresses by the candidate) “What is the anion gap?” “What is the cause of the high lactate?” “How do I work out the respiratory compensation?” “What treatment should I start?” NEED A CALCULATOR Laminated VBG result 1 actor SCENARIO 8 Examiner’s Form Domain Criteria for High Rating Medical Expertise Interpret the ABG: Acidaemia. HAGMA. Anion gap of 25. Adequate respiratory compensation (pCO2 should be 18 - mild resp alkalosis). Severe hyponatreamia - liver failure, renal failure, SIADH. Very high lactate - Hypoxia, hepatic failure, sepsis, seizure, poisoning, toxic alcohols. Hypoglyceamia - Hepatic failure, seizure. No Delta gap, suggesting a pure HAGMA. Needs fluid resuscitation (Albumin?), Glucose, Hypertonic saline. Watch fluid status carefully. Seek and treat possible infection. Consider seizure as possible cause and monitor carefully. Measure INR and albumin and renal function - hepatorenal syndrome. Recognises seriousness of illness. Scholarship & Teaching Permits registrar to ask questions Teaching method that is structured and tailored to Registrar’s understanding Communication Verbal clarity, conciseness, specificity Professionalism Shows respect Professional appearance, demeanor and conduct SCENARIO 9 - Missed Lis Franc injury Candidate’s Instructions A patient has represented to your ED today with a painful foot. She was seen in the ED 7 days ago after injuring her foot in a fall from a horse and discharge with a diagnosis of a sprained foot and ankle. She has represented as her foot is not improving. You have a copy of her original Xrays to view. The films are yet to be reported. Please interpret the Xrays and discuss the findings with the patient and address her concerns and outline further management. You are not required to examine the foot, which is still very swollen and bruised in the midfoot area and the patient cannot weight bear. You will be assessed on your communication, professionalism and management of the patient’s concerns and injury. You have 7 minutes for this scenario. Domains assessed; Medical expertise Health Advocacy Communication Professionalism SCENARIO 9 - Missed Lis Franc injury - Actor’s instructions You injured your foot in a fall from a horse 10 days ago. The horse was barely moving and your left foot became caught in the stirrup when you fell. You were seen in the ED at the time and told that your Xray was normal and sent home with crutches and a bandage. You still cannot walk on your foot and are waiting to see your GP about it. You received a phone call today from a doctor in the ED, who advised you that the Xray of your foot was not normal and you need to return to hospital. You are quite annoyed, as you have been unable to work at your small business (hairdresser) since the injury and are now concerned you will need even longer off work. You run the business yourself and hence you have had to close your business for now. You can be annoyed/upset, but not rude. You really want to know why this was not picked up initially and why it has taken 10 days to be called back. Please ask these questions. You should act just as if this was happening to you. Also ask: “What happens now?” “Do I need an operation?” “How long will I be off work?” “Are you going to deal with the Dr who missed this?” 1 actor with bandaged foot Crutches for effect. Xray of Lisfranc injury SCENARIO 9 - Missed Lis Franc injury Examiner’s form Domain Criteria for High Rating Medical Expertise Further investigation and management of LisFranc injury Correctly interprets the Xray Communication Allows time for patient to vent frustration. Acknowledges their concerns. Clear and concise language Seeks information about social and occupational circumstances Allows patient to ask questions Health Advocacy Seeks an understanding of the patient’s situation and concerns about previous presentation. Explores impact on occupation and financial implications. Enable patient to make choices, through information, advice and understanding of his circumstances Professionalism Shows respect and empathy Professional appearance and conduct SCENARIO 10 Consent for LP Examiner’s form Domain Criteria for High Rating Medical Expertise Demonstrates knowledge of role of LP in ruling out subarachnoid haemorrahge, including the probability of SAH in this patient with a normal CT. Demonstrates knowledge of risks/complications of LP Demonstrates knowledge of consequences of missed SAH May explore other imaging modalities, but must understand and explain to the patient that none will demonstrate if a bleed has occurred if the original CT is normal. Clear about patient’s decision to have/not have an LP Communication Clear, concise, jargon free language Allows patient the opportunity to ask questions Clearly communicate risk, benefits and what is involved in the procedure Health Advocacy Enable’s patient to make choices, through information, advice and understanding of risks and benefits of LP - shared decision making Professionalism Shows respect Professional appearance and conduct SCENARIO 10 Candidate’s information Your task is to discuss the need for a lumbar puncture with the patient, who presents after onset of a sudden severe headache whilst exercising at the gym. The headache was occipital, severe and has improved now with analgesia, but is still present. There is no neurological deficit. No vomiting or fever. A CT scan of the brain 8 hours after the onset of the headache has been reported as normal. The patient is otherwise well. You have 7 minutes for this task, at which point the patient should have reached a decision regarding the LP. Domains assessed; Medical expertise Health Advocacy Communication Professionalism SCENARIO 10 Consent for LP Actor’s information You experienced the worst headache of your life this morning whilst exercising at the gym. The headache was at the back of your head, came on suddenly and was very severe. It has improved now with some analgesia. You have had a CT scan, which is normal, looking for “bleeding around the brain”. The candidate will discuss with you the need for a lumbar puncture to exclude a bleed from a weak blood vessel around your brain - a serious condition that could result in a life threatening stroke if it was to bleed again. You are reluctant to have a needle stuck in your back and you should decide whether to have the LP or not based on your discussion with the candidate. 1 Actor SCENARIO 11 Paediatric Seizure/Meningitis Domain Criteria for High Rating Medical Expertise Recognises seriously ill child. Examiner’s form Establishes IO access. Gives drugs to terminate the seizure. Begins resuscitation and administers appropriate antibiotics. Addresses enquiry about FEAST trial and fluid resuscitation appropriately Takes appropriate investigations, including blood culture. Focused assessment for source of sepsis, strongly considers meningitis Measures and corrects low BSL Appropriate plan for ongoing management. Communication Clear, concise, closed loop communication. Controls flow of communication and verbalizes plan to the team. Appropriate handover to PICU consultant Leadership & Clear leadership ability. Delegates roles to team members. Management Maintains situational awareness. Prioritizes tasks appropriately. Confident, calm approach. Teamwork & Collaboration Utilizes team members effectively Summarizes and updates team with the management plan appropriately SCENARIO 11 Paediatric sepsis Actor/Confederates notes The patient is a 14 month old girl called Mia, who has presented with a fever, reduced oral intake and drowsiness. She has a seizure as the resident starts to assess them and they call the consultant for assistance. There is no IV access and it cannot be easily obtained. She has septic shock, no clear source of infection clinically, but meningitis is likely. Her legs are mottled and she looks unwell. Her vital signs are P 195 Sats 95% RA BP 60/40 RR Temp 39.4°C 50 She requires IV access, resuscitation, IV antibiotics and a PICU admission. Act as you normally would, but avoid giving the candidate direct prompts about management. Pointing out vital signs and clinical deterioration is expected and acceptable. A venous blood gas is available to review. Glucose is 2.4. Only reveal this is the candidate asks for it to be measured. The resident will ask a number of questions. When fluid resuscitation begins, please ask the candidate “what do you think about the FEAST Trial (showed an increased mortality in paediatric sepsis with higher volumes of resuscitation) and should this alter our fluid resuscitation?” “When should we think about inotropes?” “What do you think about this VBG?” (if one is taken) 2 x Actors. Use modified meningitis scenario and VBG. SCENARIO 11 Candidate’s Information This station involves a simulated patient. Please manage the patient exactly as you would in a real clinical setting You will be asked to assist with the management of a 14 month old girl called Mia, who has presented with a fever, reduced oral intake and drowsiness. She has a seizure as the resident starts to assess them and they call you for assistance. You have 15 minutes for this station. There will be 2 nurses and the registrar in the room, as well as a simulated patient. Any information about the patient’s condition that you cannot directly observe from the patient will be provided by the senior nurse on request. All treatment is to be carried out as if this is a real patient. Domains assessed; Medical expertise Communication Leadership and Management Teamwork and Collaboration SCENARIO 12 REGISTRAR COMPLAINT Examiner’s form Domain Criteria for High Rating Communication Clear and concise. Does not shy away from the issue. Genuinely curious about what happened and why. Leadership & Collaborative, non-belligerent approach Management Discusses specific issues of the complaint Listen’s to the trainee’s side of the story Explores any extenuating circumstances for behaviour Reaches agreement with trainee on expected level of behaviour Seeks consent from trainee to feedback to staff member concerned Professionalism Consultant level approach. Takes matter very seriously. Professional and respectful, but firm in recommendations and advice to the trainee SCENARIO 12 REGISTRAR COMPLAINT Actor’s form You are an ED trainee. One of the pharmacists has made a complaint that you were very rude to her over the phone. You had written a prescription for antibiotics for a patient with a UTI, but the pharmacist had a question about the dose and the indication for using ciprofloxacin for a UTI in a young woman with no allergies. You became quite angry with the pharmacist and told them in no uncertain terms that it was none of their business why you were prescribing ciprofloxacin and the dose was fine (500mg tds). The pharmacist politely tried to suggest 500mg BD, but you shouted and swore at her to “just give the patient the cipro like I asked and stop #@&%%* bothering me”. The pharmacist hung up. You have not been enjoying work recently, after your were involved in disagreement with an inpatient consultant who did not want to admit a patient who you thought needed admission with chest pain. The patient went home on their advice but represented a week later with an AMI. You are bit sorry about what you said to the pharmacist, but are reluctant to admit it, as feel that you are the only person working hard here and that if everyone else in the hospital would just pull their weight life would be much better. The candidate will be acting as your consultant and has been asked to discuss the issue with you and make a recommendation to the director. Please act as if you don’t really care about this incident and you expect the consultant to just brush off the complaint. However, if they ask you about any issues you are dealing with, please bring up the recent issue with the inpatient consultant and your feelings about lack of enthusiasm for work, compounded by your (unfounded) views on the poor work ethic of those around you. SCENARIO 12 REGISTRAR COMPLAINT Candidate’s Information At this station you will be asked to discuss with a trainee a recent complaint made against them by one of the hospital pharmacists. The complaint reads “The doctor was exceptionally rude to me on the phone. I called to check the prescribed dose of ciprofloxacin and why it was being prescribed to a young woman with a UTI, as I am required to do by the hospital’s protocol on antibiotic prescribing. The dose was prescribed was 500mg tds rather than the usual BD. When I asked about this with the doctor, they swore at me, told me it was none of my business why they were prescribing ciprofloxacin and said ‘just give the patient the cipro like I asked and stop #@&%%* bothering me’. I think that this behaviour is clearly against the hospital’s code of conduct policy and I would like a formal apology and the doctor concerned dealt with.” Please discuss the compliant with the trainee and make recommendations to them based on your discussion. You have 7 minutes for this station. SCENARIO 14 Toxicology/phone advice Examiner’s Form Domain Criteria for High Rating Medical Expertise Recognizes’ s seriousness of patient’s overdose Appropriate assessment of clinical picture (risk assessment) Appropriate recommendation for treatment - Calcium - Adrenaline - Fluids - High dose insulin and dextrose - Decontamination Advice regarding patient transfer - intubation Communication Clear, concise instructions and recommendations Clear and concise language Checks that instructions are understood Health Advocacy Ensures that plans are being put in place to have the patient retrieved Professionalism Shows respect and is collegial with rural doctor Professional conduct and supportive of rural doctor SCENARIO 14 Toxicology/phone advice Actor’s Information In this station, the examiner will be the rural doctor making the call for advice. You are an experienced rural GP who is covering the small local emergency department, when a 5 year old girl presents after a large calcium blocker overdose. She was being cared for by her grandmother, who found her with an empty packet of Verapamil 360mg SR tablets about 2 hours ago. The child is a currently alert. Vitals signs P 50 BP 70/45 Sat 98% RA Temp 36.4°C RR 36 You call the nearest Emergency Department to ask for advice on management of the girl from the Emergency Physician. You have IV access and have given 10mls/kg of N/saline as a bolus. The girl weighs 20 kg. Your hospital is 2 hours flying time by helicopter from the ED you are calling. Things to ask the candidate; “Should I give charcoal?” Clarify the dose of any medication given. If they mention high dose insulin/dextrose - ask about why and can you give it through a peripheral cannula? Phone x 2, Blood gas results for GP (if asked) SCENARIO 14 Candidate’s Information You will receive a phone call from a GP who works at a small rural hospital which is about a 4 hour drive away. The GP is managing a 5 year old girl who has accidentally taken a large number of her Grandmother’s calcium channel blocker medication. Please provide advice to the GP over the phone. The phone will ring once you enter the room. The GP role is being played by the examiner. You have 7 minutes for the station. Domains assessed; Medical expertise Communication Professionalism Health Advocacy SCENARIO 15 Suicidal Ideation Examiner’s form Domain Criteria for High Rating Medical Expertise Assess suicide risk in a thorough and formalized way. Assess options for safe discharge and follow up. Communication Clear and concise communication Direct questions about relevant suicide risk factors Health Genuinely concerned about patient’s wellbeing and risk of self-harm. Advocacy Professionalism Shows respect and empathy Professional conduct and non-judgmental approach The actor’s suicide risk is actually low (score 4 below), but a thorough formal assessment should be made elucidating the following or similar factors; S: Male sex → 1 A: Age 15-25 or 59+ years → 1 D: Depression or hopelessness → 2 P: Previous suicidal attempts or psychiatric care → 1 E: Excessive ethanol or drug use → 1 R: Rational thinking loss (psychotic or organic illness) → 2 S: Single, widowed or divorced → 1 O: Organized or serious attempt → 2 N: No social support → 1 S: Stated future intent (determined to repeat or ambivalent) → 2 This score is then mapped onto a risk assessment scale as follows: 0–5: May be safe to discharge (depending upon circumstances) 6-8: Probably requires psychiatric consultation >8: Probably requires hospital admission - May be suitable for discharge and follow up with GP/community mental health team, but lack of a responsible person to take the patient home, psychiatric consultation likely to be required.] SCENARIO 15 Suicidal Ideation Actor’s instructions In this scenario, you will be playing the role of a young woman who has presented to hospital after taking 10 paracetamol tablets following a fight with her boyfriend. The candidate will be asked to assess your risk of suicide. If you DO NOT think that you can play this role for any reason or it becomes difficult for you at any stage, please advise the examiner. Your actual risk of suicide is now low. You had your first major fight with your boyfriend of 4 months. You were angry and upset at the time, and in that distressed state, you took 10 paracetamol tablets telling him that you wanted to kill yourself. He called the ambulance. Soon after taking the tablets you regretted it and you don’t really want to die now, but at the time you thought that you did. You have no plan/date for any future suicide attempts and do not feel suicidal now. You are otherwise well. When you were 24 years of age you took an overdose of nurofen tablets, with no ill effects, but were admitted overnight to hospital. You were treated for depression with medication (Effexor) for 2 years after that episode, but have been feeling well since and have been free of medication and counselling for nearly 5 years. No other psychiatric history or medical history. No family history of mental illness. You live in a share house with 2 friends. You are studying Architecture at University and will finish at the end of the year. You do not feel helpless or hopeless, but have been struggling with money and your university studies as you try to balance studying and working. You do not use any illicit drugs, but drink 4-5 glasses of wine each night. Your family live in Melbourne and you do not have much contact with them. No local family. If you were discharged you would head home to your share house. You have a GP that you could see in the next few days. You want to go home. SCENARIO 15 Candidate’s Instructions You will be asked to assess a young woman for ongoing risk for suicide. She present’s after taking 10 x 500mg paracetamol tablets after a disagreement with her partner. Please focus your assessment on her suicide risk. You have 7 minutes for this station. At the end of this scenario, please discuss with the patient what you think their risk of suicide is and what will happen next. Domains assessed; Medical expertise Communication Professionalism Health Advocacy SCENARIO 16 CXR/REQUEST FOR ADMISSION Domain Criteria for High Rating Medical Expertise Recognizes’ s need for admission Examiner’s form Interpret CXR findings correctly in light of clinical picture Communication Clear and concise language Clearly and effectively communicated need for admission Graded assertiveness to deal with Respiratory consultant’s reluctance Health Advocacy Advocate on behalf of patient for appropriate care from inpatient team Professionalism Shows respect and is collegial with Respiratory Physician Professional conduct You will play the role of the respiratory consultant on the phone. You are to be obstructive and not keen at all to admit the patient. The resident who spoke to you earlier could not clearly explain the Xray findings. Please be sure to clarify what the Xray shows. Eventually the candidate should be able to convince you that the patient does require admission. Please keep an eye on the time. The phone call should go for no more than 7 minutes. SCENARIO 16 CXR/REQUEST FOR ADMISSION Candidate’s Information A resident in your department has attempted to refer a patient to the respiratory team for admission, but the respiratory consultant Dr Blogs does not think the patient requires admission. The resident is very concerned about discharging the patient as they feel that they are unwell and their social situation will impact on their treatment. The patient, John Smith, is a 32 year old man who presents with a productive cough, lethargy and fever for 5 days. He admits to being an IV drug user and is currently of no fixed abode and has no money. He has previously had bacterial endocarditis. He has no other significant past medical history. On exam, He looks unwell. He is mildly dehydrated. P 110 Sat 100% 2LNPO2 TEMP 38.7°C BP 95/65 His left lung has some very coarse creps in the mid zone. WCC 19. Lactate of 1.9. Other bloods are normal. Her Xray is available for you to review. Please review his Xray and call the Respiratory team to facilitate his admission. You have 7 minutes to perform this task. Domains assessed; Medical expertise Communication Professionalism Health Advocacy