Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
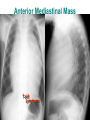
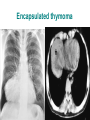
Mediastinal Syndromes 1 • Division Mediastinum - Superior, - Inferior - Anterior, - Middle, - Posterior compartments. • The mediastinum contains all of the vital structures of the chest except the pulmonary parenchyma. Mediastinal Regions Mediastinum • The superior mediastinum lies between the manubrium and thoracic vertebrae one to four. • The anterior mediastinum is bounded by the sternum anteriorly and pericardium posteriorly. • The middle mediastinum consists of the heart and vascular structures; anything in the middle of the chest that is radio dense on lateral radiograph is within the middle mediastinum. • The posterior mediastinum lies between the heart and the vertebral bodies. Subdivision of mediastinum • anterior mediastinum • middle mediastinum • posterior mediastinum Mediastinal Lesions • Any lesion that occurs in the mediastinum – can be focal or diffuse. • CT scan or MRI with contrast is usually indicated for further evaluation. Mediastinal Lesions Focal vs Diffuse Anthrax Thymoma 1. Superior Mediastinum • • • • • • • • Aortic Arch & its branches Brachiocephalic and subclavian vessels Superior vena cava upper half & tributaries Trachea Thyroid Oesophagus Thoracic duct Phrenic ,Vagus ,Cardiac, Lt.Recurrent L nerves 2. Anterior Mediastinum Anterior mediastinum Anterior Mediastinal Masses •Thymus •Thyroid •Ectopic Thyroid Tissue •Parathyroid Gland •Internal mammary vessels •Lymph nodes •Aortic Arch •SVC Superior Vena Cava •Thymic lesions (and parathyroid masses) •Teratomas (and other germ cell tumors) •‘Terrible' lymphoma •Tortuous vessels •Dissecting aorta, right arch •Trauma •Aortic aneurysm, •Pericardial cyst, •Epicardial fat pad •Lymphadenopathy. Anterior mediastinal mass Anterior Mediastinal Mass T-cell Lymphoma Mediastinal Lesions • Anterior lesions – thymoma, thyroid lesions, teratoma, tcell lymphomas, and lymphadenopathy. • Usually seen in retrosternal space. anterior lesion. Lymphoma Mediastinal Lesions • Lateral view shows a solid tissue density in the region anterior and superior to the heart. • Lymphoma is the most common anterior mediastinal mass. Lymphoma 3. Middle Mediastinum Middle mediastinum Heart and pericardium Ascending aorta Superior vena cava Azygous vein Phrenic and vagus nerves Trachea Trachea Bifurcation and main bronchi Pulmonary arteries and veins Hilar Lymph Node Middle Mediastinal Mass lymphadenopathy due to metastases or primary tumor. Other causes include hiatial hernia, aortic aneurysm, Thyroid mass, duplication cyst, and bronchogenic cyst. Mediastinal Lesions • Middle lesions – thoracic aortic aneurysms, hematomas, neoplasms, lymphadenopathy, esophageal lesions, and diaphragmatic hernias. • Enlarged lymph nodes are the most frequent cause of a middle mediastinal mass. lymphadenopathy Mediastinal Lymphadenopathy • InfectionPneumonia, TB, Anthrax • Inflammation Sarcoidosis • MalignancyLymphoma, Metastatic 4. Posterior Mediastinum Posterior Posterior mediastinal mass •Esophagus •Thoracic duct •Thoracic descending •Aorta Descending •Azygos •Hemiazygos vein •Vagus nerves •Sympathetic Chain •Paravertebral Lymphnode •Neurogenic lesions, •Neoplasm , •Lymphadenopathy , •Aortic aneurysm, •Adjacent pleural or lung mass, •Neurenteric cyst or lateral meningocele, and •Extramedullary hematopoiesis Mediastinal Lesions • Posterior lesions – Neurogenic lesions, hiatal hernias, descending aortic aneurysm, neoplasms, and hematomas. • 90% of posterior lesions are neurogenic lesions. Aneurysm of Descending Aorta Posterior mediastinal masses will give double density over left side of heart. Origins of Mediastinal Mass • • • • • Developmental Neoplastic Infectious Traumatic Cardiovascular disorders Mediastinologists • • • • • • Thoracic Surgeon Pulmonologist ENT Cardiologist Endoscopist Radiologist Differentials • • • • • • • • Diaphragmatic lesions; eventration ,hernia Esophageal tumours ,achalasia Mediastinal metastasis Mediastinal lymph nodes: lymphomas, granulomas Thyroid retrosternal extension Aneurysm of aorta Ventricular aneurysm Tracheal , heart tumours Incidence • • • • • • • • 1 in 100000 Thrice more common than bronchial adenoma 1/3000 admission at large medical centre Neural commonest 20-27% Thymic second 19-26% Cyst third 18-21% Teratomas \ lymphoma fourth 12% Neural , Thymic, developmental ,Lymphoma :88% of all mediastinal tumours Children Adult •Neural tumours 40% •Lymphoma 20% •Teratomas & Cysts 10-15% •Thymic rare •Posterior Mediastinum •Most often benign •2/3 of tumors symptomatic •Neural tumours 20-27% •Thymic 19-26% •Cyst third 18-21% •Teratoma \ lympho 11-12% •Anterior Mediastinum •Often Malignant •1/3 of tumors are symptomatic •Ages 30 – 50 Malignant Tumors Invasion Structure • • • • • Tracheobronchial tree and lungs Esophagus Superior Vena Cava Pleura and Chest Wall Intrathoracic nerves Primary Mediastinal Tumors • Neural – Nerve sheath – Autonomic nervous system – Malignant peripheral nerve sheath – Granular cell tumour • • Thymic Thyroid • Germ cell tumours – Benign – Malignant • Seminomatous • Non seminomatous • Lymphomas • Developmental cysts • Pleuropericardial cysts Symptoms • Cough often recurrent • Shortness of Breath may be with wheeze • Chest pain • Fever • Chills • Weight loss • Night Sweats • Hemoptysis • Airway compression with – Stridor – Hoarseness • Esophageal compression – dysphagia • SVC compression …. – Neck vein engorgement, – facial swelling • Rt.ventricular outflow obstn – Pericarditis – Cardiac temponade – Heart failure Mediastinal Neural tumours Nerve sheath t0 • Benign (neurolemmoma) – Schwannoma – Neurofibroma • Malignant peripheral nerve sheath t0 – – – – – Neurosarcoma Neurofibrosarcoma Neurogenic sarcoma Malignant schwannoma Malignant neurinoma • Granular cell tumour Granular cell myoblastoma – Autonomic nervous system (neurocyte) • • • • Ganglioneuroma Ganglioneuroblastoma Neuroblastoma Paraganglioma – Aorticopulmonary – Aorticosympathetic Large Neuroma Ganglioneuroma Ganglioneuroblast Neuroblastoma oma •Most common •< 20 yrs age •Posterior mediastinum •Rare tumour in adults •50% in first 3 yr of age •Majority occur in adrenal medulla •Sex : equal •Equal among both sex •Often pear shaped or lobulated •Majority are encapsulated •Must be regarded as malignant •Encapsulated •Slow growing •Benign, May be malignant •Adults rarely •Within 2 yrs , •Posterior mediastinum •Adrenal medulla, 20% in thorax •Retroperitoneal •Equal in both sexes •Radio-logically less well defined •Highly malignant •Locally invasive •Spontaneous regression may occur Intrathoracic Meningocele Thymus of a Neonate Thymus – Thymic hyperplasia – Thymoma – Thymic cyst – Thymic carcinoma – Thymic carcinoid tumours – Thymolipoma – Germ cell tumours – Ectopic parathyroid adenomas – Lymphoma – Secondary neoplastic Thymic hyperplasia • • • • Nearly always infantile or childhood Usually asymptomatic Pronounced in HIV, SLE,Thyrotoxicosis Indistinct from other thymic t0 on Radio or CT • Steroids may reduce • Subtotal surgery Thymoma • Epithelial neoplasms • most common primary neoplasms of the anterior superior mediastinum • Any age , rare <20, nearly all middle-aged adults. • Male predominance • ½ of the patients are asymptomatic • 25-30% of patients have symptoms related to compression of adjacent mediastinal structures including cough, chest pain, and shortness of breath Thymoma • • • • • may have myasthenia gravis (30-40%), pure red cell aplasia, hypogammoglobulinemia, endocrine disorders can be completely encapsulated (benign) or locally invasive without a fibrous capsule • classified by predominant cell types: – epithelial, – lymphoid, or – Biphasic , mixed or lymphoepithelial type • one- third of thymomas are invasive and may grow into the surrounding mediastinal structures, Thymoma • This is determined at surgery and is not a histologic diagnosis, • local invasion of the pleura occurs frequently, • distant metastases are infrequent • Surgical removal enmass with capsule intact – Median sterotomy – Thoracotomy – Transcervical approach • Radiotherapy usually reserved for incomplete excission • Chemo-sensitive (May be) : cis, doxo, vin, c-phos Encapsulated thymoma Invasive Thymoma Germ cell tumours • As a result of the proliferation of the primary extragonadal germ cell • Mostly found near the midline – Adults :anterior mediastinum – Child : sacrococcygeal area Germ cell tumours • Benign – Mature cystic teratoma • Malignant – Seminomatous* : – Non Seminomatous* Anterior mediastinal mass Teratoma Malignant Germ cell tumours • Seminomatous* : Seminoma – Exclusively young male 20-40 yrs – 1/3 asymptomatic , – Chest pain, dysponea, SVC obstruction – Radio ; lobulated , non cacified ,anterior mediastinal – Normal serum AFP – USG testicle discrete hypoecoic masses,with microcalcifictions – Treatment ; chemotherapy* , Radio or combi • Et +cis *4 cycle or Et +cis +bleo * 3 cycles • Highly radiosensitive radio reserved for bulky Mediastinal Lymphoma • Mediastinum is involved in 50% Hodgkin’s diseases • Most cases are of nodular sclerosing type • Treatable and many are curable too • Intensive chemotherapy or radiotherapy or both • Radio alone relapse 50-74% • Chemo alone relapse 33-50% • “MOPP” or “DBVD” followed by radio preferred Anterior mediastinal nodes Lymphoma Anterior mediastinal nodes Lymphoma Mediastinal Mesenchymal tumours Benign Lipoma Hemangioma Lymphangioma Cystic hygroma Malignant Liposarcoma Leiomyosarcoma Rhabdomyosarcoma Hemangiosarcoma Angiolipoma Developmental Mediastinal cysts • Congenital ; 16% of all mediastinal cyst • Foregut duplication largest group • Pleuropericardial next to it Pleuropericardial cysts • Synonyms – – – – Pericardial cyst Coelomic cyst Spring water cyst Hydrocele of mediastinum • 1 / 100000 per year • 70% occur in right cardiophrenic angle – Usually anterior • Male : Female 1 :1 • All ages • 5 – 25 cms • Soft , unilocular • Crystal clear spring water , transudate with acellular & little proteins – Asymptomatic – Chest pain • Radiograph – – – – Sharply demarcaed Rounded Smooth edged Anterior mass Middle Mediastinal Cysts Bronchogenic Cyst Pericardial Cyst Aortic aneurysm Diagnostic of mediastinal masses • Chest X-Rays • CT ( Computed Tomography)/MRI • Radionuclide Scanning – Goiter • Barium studies – Most valuable for diagnosis – For: hernia,diverticuli,achalasia – Done in most of cases • Percutaneous fine needle biops • CT guided needle biopsy • Mediastinoscopy / ant. mediastinotomy – Definite diagnosis • Mediastinoscopy/ant. medistinotomy with biopsy – Definite with establishing the disease diagnosis • endoscopic ultra sound guided biopsy • Video assisted thoracoscopic removal of mass Mediastinoscopy Mediastinoscopy: Overused, Invasive, Limited Applications • Mediastinoscopy: Invasive, requires general anesthesia. Subcarinal and subaortic (a-p window) nodes inaccessible. Thoracoscopy: Limited to inferior mediastinum • Thoracoscopic biopsy (video-assisted thoracoscopy) Limited to inferior mediastinum. Endoscopic Ultrasound: No incision, no anesthesia Endoscopic ultrasound guided biopsy of mediastinal lesions has a major impact on patient management. • It is a safe and sensitive minimally invasive method for evaluating patients with a solid lesion of the mediastinum suspected by CT scanning. • It has a significant impact on patient management and should be considered for diagnosing the spread of cancer to the mediastinum in patients with lung cancer considered for surgery, as well as for the primary diagnosis of solid lesions located in the mediastinum adjacent to the oesophagus. Thorax 2002 Feb;57(2):98-103 • “Endoscopic ultrasonography also provides information helpful for clinical staging of lung cancer and is the procedure of choice for performing fineneedle aspiration biopsy of posterior mediastinal and subcarinal lymph nodes.” AJCC manual 2007 CT scan or MRI • CT scan or MRI with contrast is always indicated for further evaluation. • MRI is preferred for neurogenic lesions but obtaining a CT scan is never wrong with a mediastinal mass. • CT-guided transthoracic fine needle aspiration (FNA): Limited by surrounding vascular structures, size of the targeted lesion. – Pneumothorax risk. Prognosis • Varies depending on type of tumors and resection. • Benign tumors – excellent prognosis • Malignant tumors – depends on the type