Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
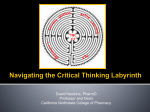
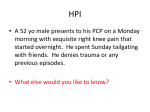
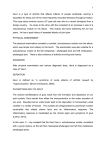
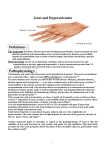
Review of Clinical Signs Series Editor: Bernard M. Karnath, MD Clinical Signs of Gout Prashanth Sunkureddi, MD Tracy U. Nguyen-Oghalai, MD Bernard M. Karnath, MD istorically, gout has been considered a disease of affluent middle-aged men who eat and drink to excess; however, gout does affect other segments of the population. Gout is a systemic disease characterized by manifestations of chronic underlying hyperuricemia, resulting in the deposition of monosodium urate crystals in various tissues. Initially, inflammatory arthropathy is episodic, but it can become persistent if left untreated. Other clinical signs of gout include tophi formation, renal calculi, and urate nephropathy. This article reviews the risk factors, clinical features, and diagnostic evaluation of gout and discusses the management of gout and hyperuricemia. H RISK FACTORS Gout has a strong male predominance, with an estimated 2% prevalence in men over age 30 years1 and a peak incidence in the fifth decade of life among men.2 Gout is rarely seen in premenopausal women but can be found in postmenopausal women. The prevalence of gout is higher in African Americans than in whites,3 and gout prevalence overall appears to have increased in recent decades.4 Other risk factors for gout include older age, obesity, taking certain medications (eg, diuretics), and consuming purine-rich food and alcohol. Alcoholic beverages not only increase urate production but also decrease urate elimination via the kidney. Beer has the highest purine content of the alcoholic beverages and confers the highest risk for developing gout. However, wine does not increase the risk of developing gout. Interestingly, a recent study by Choi et al5 showed that consuming purine-rich vegetables had no correlation with gout development and increasing dairy intake decreased gout incidence. PATHOPHYSIOLOGY Hyperuricemia is defined as a serum uric acid level www.turner-white.com FEATURES OF GOUT Gout has a strong male predominance. Asymptomatic hyperuricemia may be present for decades. Risk factors for gout include: older age, obesity, medications (eg, diuretics, niacin), and consumption of purine-rich foods and alcohol. The metatarsophalangeal joint of the great toes is involved in 50% of initial attacks. Nonsteroidal anti-inflammatory drugs (NSAIDs) are typically used as first-line therapy. Corticosteroids are an effective alternative to NSAIDs. greater than 6.8 mg/dL. Baseline uric acid level is higher among men (5.1 ± 1.0 mg/dL) than among women (4.0 ± 1.0 mg/dL).6 Common causes of overproduction or underexcretion of uric acid that can lead to hyperuricemia are shown in Table 1. When the limit of solubility of monosodium urate in plasma is exceeded, urate crystals precipitate. Urate crystals are phagocytosed by neutrophils, which subsequently release potent inflammatory mediators, such as tumor necrosis factor-α, interleukin-1, and interleukin-6. These inflammatory mediators are responsible for systemic effects (eg, fever, leukocytosis) observed during an acute attack of gout. Dr. Sunkureddi is a rheumatology fellow, and Dr. Nguyen-Oghalai is an assistant professor of medicine, Division of Rheumatology. Dr. Karnath is an associate professor of medicine, Division of General Medicine. All are at the University of Texas Medical Branch, Galveston, TX. Hospital Physician January 2006 39 Sunkureddi et al : Clinical Signs of Gout : pp. 39 – 42, 47 Table 1. Common Causes of Hyperuricemia Overproduction Foods with high purine content (eg, mussels, oysters, red meat, liver, anchovies) Alcohol Enzyme deficiencies (eg, hypoxanthine-guanine phosphoribosyltransferase, phosphoribosyl pyrophosphate) Obesity Increased cell turnover Malignancy Psoriasis Figure 1. Acute arthritis of the right first metatarsophalangeal joint in a patient with gout (known as podagra). Underexcretion Renal disease Lead intoxication (“saturnine gout”) Medications (eg, diuretics, cyclosporine, low-dose aspirin, pyrazinamide, niacin, ethambutol) Metabolic acidosis (eg, ketoacidosis, lactic acidosis) Alcohol CLINICAL FEATURES Gout can be described in 4 stages: asymptomatic hyperuricemia, intermittent acute gout, intercritical gout, and advanced or chronic tophaceous gout. The first stage, asymptomatic hyperuricemia, may be present for decades and is characterized by silent urate deposition in tissue. The degree of hyperuricemia correlates with the development of a gout attack in the second stage.7 Acute gout attacks occur abruptly with severe joint pain and inflammation and are typically monoarticular. In 50% of the initial attacks, the metatarsophalangeal joint of the great toes is involved, commonly known as podagra (Figure 1). Over time, attacks may become polyarticular and involve the ankles, knees, wrist, and joints in the hands. Impressive erythema of the surrounding area may also occur. Although the attack is often dramatic and painful, it is usually selflimited and lasts only several days. After each attack, long asymptomatic intervals may occur, which are referred to as the intercritical period.8 This stage may last many years and, in some cases, patients have persistent hyperuricemia and low-grade inflammation in the joints.9 Gout attacks can be precipitated by rapid changes in the serum urate level caused by trauma, alcohol consumption, medications, and increased consumption of purine-rich foods (eg, hospitalized patients such as those admitted for a myocardial infarction or surgery who are not on their usual diet). As the disease progresses, the intercritical periods of gout become shorter and attacks occur more often, 40 Hospital Physician January 2006 Figure 2. Arthritis of the hands. Note the distribution of the arthritis. The metacarpophalangeal and proximal interphalangeal joints are predominantly affected, as in rheumatoid arthritis. eventually leading to the last stage, advanced or chronic tophaceous gout. Patients often complain of constant pain and swelling in the joints. The clinical features of chronic gouty arthritis can be similar to rheumatoid arthritis (Figure 2), but in gouty arthritis, plain radiographs of the joints show distinctive submarginal erosions with “overhanging edges,” atrophic and hypertrophic features, and minimal periarticular osteopenia (Figure 3). Also, deposition of clusters of urate crystals in soft tissues, known as tophi, can occur (Figure 4). While tophi can form anywhere in the body, commonly involved sites are the olecranon bursa, fingers, wrists, and sometimes the helix of the ear. In chronic gout, urate deposition in the kidneys can also cause renal problems, such as urate renal stones (10%–25% of all patients with gout) and urate nephropathy, which can lead to progressive renal failure.6 DIAGNOSTIC EVALUATION The definitive diagnosis of gout is made by verifying the presence of monosodium urate crystals in neutrophils from synovial fluid obtained from the affected joint (via aspiration). Uric acid crystals are needleshaped and, under a compensated polarizing microscope, are yellow and negatively birefringent when www.turner-white.com Sunkureddi et al : Clinical Signs of Gout : pp. 39 – 42, 47 Figure 4. A large tophus at the olecranon in a patient with chronic gouty arthritis. Figure 3. Radiograph of the left hand in a patient with chronic gouty arthritis showing erosions in the second metacarpophalangeal joint, third proximal interphalangeal joint, and the distal radius. Note the joint space narrowing, the cystic lesions, the lack of periarticular osteopenia, and the submarginal location of the erosions. (Reprinted with permission from American College of Rheumatology. ACR slide collection on the rheumatic diseases. 3rd ed. Atlanta: The College; 2004. Copyright © 1972 – 2004 American College of Rheumatology Clinical Slide Collection.) parallel to the plane of the polarizing lens (Figure 5). Cell count of the synovial fluid typically shows an inflammatory exudate, with leukocyte counts ranging from 5000 to 80,000 cells/µL and with neutrophilic predominance. The synovial fluid should also be evaluated for infection with Gram stain and culture because septic arthritis can rarely occur with acute gouty arthritis. Serum uric acid levels should be checked, but an elevated serum uric acid level is not required to establish the diagnosis of acute gout. Although most patients will demonstrate hyperuricemia, a small number of patients may have a normal uric acid level at the time of an attack.10 A 24-hour urine collection for uric acid is not routinely performed in the initial evaluation but can be done when uricosuric therapy is being considered. Radiography of the affected joint in acute gout may reveal soft tissue swelling but no characteristic bone or joint abnormalities. www.turner-white.com Figure 5. Under a compensated polarizing microscope, urate crystals are needle-shaped, and they appear blue when perpendicular to the plane of the polarizing lens compensator (A), disappear when in the plane (B), and are yellow when parallel to the plane (C). (Reprinted with permission from American College of Rheumatology. ACR slide collection on the rheumatic diseases. 3rd ed. Atlanta: The College; 2004. Copyright © 1972 – 2004 American College of Rheumatology Clinical Slide Collection.) The American College of Rheumatology criteria for the classification of acute gouty arthritis state that the diagnosis of gout can be made based on clinical, laboratory, and/or radiographic findings without demonstration of crystals (Table 2).11 However, if a synovial fluid analysis is not performed, other conditions that can mimic acute gout, such as rheumatoid arthritis, pseudogout, septic arthritis, trauma, and avascular necrosis, cannot be definitively ruled out. MANAGEMENT OF ACUTE GOUT Nonsteroidal anti-inflammatory drugs (NSAIDs) can effectively treat acute gout attacks and are typically used as first-line therapy. Oral indomethacin has traditionally been the NSAID of first choice, initially administered at a dose of 50 to 75 mg and then 50 mg every 6 hours thereafter (maximum of 200 mg in 24 h). However, other NSAIDs, including the cyclooxygenase-2 selective agents, are effective as well.12 In general, NSAIDs should be started as soon as possible after a Hospital Physician January 2006 41 Sunkureddi et al : Clinical Signs of Gout : pp. 39 – 42, 47 Table 2. Criteria for the Classification of Acute Gouty Arthritis A. The presence of characteristic urate crystals in the joint fluid, or B. A tophus proved to contain urate crystals by chemical means or polarized light microscopy, or C. The presence of 6 of the following clinical, laboratory, and/or radiographic features: More than 1 attack of acute arthritis Maximal inflammation developed within 1 day Attack of monoarticular arthritis Joint redness First metatarsophalangeal joint painful or swollen Unilateral attack involving first metatarsophalangeal joint Unilateral attack involving tarsal joint Suspected tophus Hyperuricemia Asymmetric swelling within a joint (shown on radiography) Subcortical cysts without erosions (shown on radiography) D. Negative culture of joint synovial fluid for microorganisms during attack of joint inflammation Adapted with permission from Wallace SL, Robinson H, Masi AT, et al. Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum 1977;20:895–900. gout attack occurs and continued for 24 to 48 hours after the inflammation subsides. Because of the increased risk for gastrointestinal (GI) toxicity and renal damage with NSAIDs, caution must be exercised in high-risk patients, such as the elderly and those with underlying GI or renal disease. For patients unable to tolerate NSAIDs, corticosteroids are an effective alternative and can be given orally, intra-articularly, or intramuscularly. Intra-articular injection of trimacinolone (10–40 mg) with lidocaine can provide prompt relief in monoarticular gout. Systemic corticosteroids (triamcinolone 80 mg given intramuscularly or 3–5 days of prednisone 20–40 mg) can be used in patients with polyarticular gout. Adrenocorticotropic hormone has also been used to treat acute gout.13 Although effective for treating acute gout, the use of colchicine is limited by serious side effects and a frequent administration schedule. Colchicine 0.6 mg orally must be given every hour until symptoms have resolved, side effects have developed, or a maximum dose of 6 g has been given. Most patients develop GI side effects, such as nausea, vomiting, abdominal pain, and diarrhea, prior to resolution of the arthritis. Use of intravenous colchicine can avoid some GI toxicity, but the risk for toxicity is still high; it is contraindicated in patients with hepatic disease, renal failure, prior use of colchicine, or bone marrow suppression. For prophylaxis against recurrent attacks, colchicine 0.6 mg daily is effective and is usually continued until the serum uric level is below 6.0 mg/dL or after 6 months. MANAGEMENT OF HYPERURICEMIA The management of hyperuricemia is an essential component of the overall treatment of gout. Uratelowering agents not only control hyperuricemia but also can reverse urate deposition. Many experts recommend treatment of hyperuricemia with urate-lowering agents if a patient has tophi, 2 or more arthritis attacks per year, erosive arthritis seen on radiography, or renal calculi.14 Allopurinol lowers serum urate levels by inhibiting urate production and is a competitive inhibitor of xanthine oxidase, the last enzyme in the purine metabolism pathway that generates urate. The typical starting dose of allopurinol is 300 mg/d, and the dose can be titrated up to 800 mg/d to achieve the desired serum urate level of 6 mg/dL. Patients with renal insufficiency should be started at a lower dose (50–100 mg/dL) with slow titration as tolerated. There is a risk of precipitating an acute gout attack when initiating allopurinol. It is recommended that patients start or continue prophylactic therapy with either NSAIDs or colchicine when starting urate-lowering therapy.15 One option is to continue colchicine 0.6 mg daily for 6 months for prophylaxis in addition to allopurinol. Febuxostat, a new nonpurine xanthine oxidase inhibitor, has been reported to be efficacious and safe; US Food and Drug Administration approval is pending.16 A less commonly used treatment of hyperuricemia is probenecid, a uricosuric agent. The typical starting dose is 500 mg/d, titrated up to 3000 mg/d. Prior to starting therapy with a uricosuric agent, a 24-hour urine collection for uric acid should be performed. Typical indications for probenecid are urinary uric acid excretion of below 800 mg/24 h, age 60 years or younger, normal renal function, and no history of renal calculi.6 Xanthine oxidase inhibitors and uricosuric agents can be combined if serum urate levels are not reduced below 6 mg/dL on a single agent. Typically, patients continue on urate-lowering therapy indefinitely. Currently, urate-lowering therapy is not indicated for asymptomatic hyperuricemia. ADVERSE EFFECTS OF GOUT THERAPY Adverse reactions reported with allopurinol include GI intolerance, bone marrow suppression, and skin rashes. Another severe adverse effect is the allopurinol hypersensitivity syndrome, which is characterized by a (continued on page 47) 42 Hospital Physician January 2006 www.turner-white.com Sunkureddi et al : Clinical Signs of Gout : pp. 39 – 42, 47 (from page 42) skin rash, hepatitis, eosinophilia, fever, renal failure, and possibly death. Patients with underlying renal insufficiency and those taking diuretics are mostly likely to develop the allopurinol hypersensitivity syndrome. Also, patients taking azathioprine or 6-mercaptopurine should avoid allopurinol or substantially reduce their dose because of the risk of bone marrow suppression. Chronic colchicine therapy has been associated with rhabdomyolysis and a painful axonal neuromyopathy and should be avoided in patients with significant renal or hepatic disease.17 Probenecid is generally well tolerated, with GI distress being the most common adverse effect; however, it alters the metabolism of many drugs, including penicillin, heparin, and indomethacin. 10. CONCLUSION 11. Gout is a systemic disease characterized by manifestations of hyperuricemia, such as inflammatory arthritis, tophi formation, nephropathy, and nephrolithiasis. When possible, diagnosis should be made by identifying characteristic urate crystals in synovial fluid. Therapy for gout is effective and can dramatically change the course of the disease. New drugs that are currently under development may provide additional options to treat gout in HP patients not amenable to current therapies. REFERENCES 6. 7. 8. 9. 12. 13. 14. 15. 1. Choi HK, Curhan G. Gout: epidemiology and lifestyle choices. Curr Opin Rheumatol 2005;17:341–5. 2. Roubenoff R, Klag MJ, Mead LA, et al. Incidence and risk factors for gout in white men. JAMA 1991;266:3004–7. 3. Johnson RJ, Rideout BA. Uric acid and diet: insights into the epidemic of cardiovascular disease. N Engl J Med 2004;35:1071–3. 4. Arromdee E, Michet CJ, Crowson CS, et al. Epidemiology of gout: is the incidence rising? J Rheumatology 2002;29: 2403–6. 5. Choi HK, Atkinson K, Karlson EW, et al. Purine-rich 16. 17. foods, dairy and protein intake, and the risk of gout in men. N Eng J Med 2004;350:1093–103. Terkeltaub RA. Gout. Epidemiology, pathology, and pathogenesis. In: Klippel JH, Crofford L, Stone JH, et al, editors. Primer on the rheumatic diseases. 12th ed. Atlanta: Arthritis Foundation; 2001:307–12. Campion EW, Glynn RJ, DeLabry LO. Asymptomatic hyperuricemia. Risks and consequences in the Normative Aging Study. Am J Med 1987;82:421–6. Yu TF. Diversity of clinical features in gouty arthritis. Semin Arthritis Rheum 1984;13:360–8. Pascual E. Persistence of monosodium urate crystals and low-grade inflammation in the synovial fluid of treated gout. Arthritis Rheum 1991;34:141–5. Logan JA, Morrison E, McGill PE. Serum uric acid in acute gout. Ann Rheum Dis 1997;56:696–7. Wallace SL, Robinson H, Masi AT, et al. Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum 1977;20:895–900. Wortmann RL. Recent advances in the management of gout and hyperuricemia. Curr Opin Rheumatol 2005;17: 319–24. Axelrod D, Preston S. Comparison of parenteral adrenocorticotropic hormone with oral indomethacin in the treatment of acute gout. Arthritis Rheum 1988;31:803–5. Mikuls TR, MacLean CH, Olivieri J, et al. Quality of care indicators for gout management. Arthritis Rheum 2004; 50:937–43. Wortmann RL, Kelley WN. Gout and hyperuricemia. In: Harris ED Jr, Budd RC, Firestein GS, et al, editors. Kelley’s textbook of rheumatology. 7th ed. Philadelphia: Saunders/Elsevier; 2004:1402–29. Becker MA, Schumacher HR Jr, Wortmann RL, et al. Febuxostat, a novel nonpurine selective inhibitor of xanthine oxidase: a twenty-eight-day, multicenter, phase II, randomized, double-blind, placebo-controlled, doseresponse clinical trial examining safety and efficacy in patients with gout. Arthritis Rheum 2005;52:916–23. Emmerson BT. The management of gout. N Engl J Med 1996;334:445–51. Copyright 2006 by Turner White Communications Inc., Wayne, PA. All rights reserved. www.turner-white.com Hospital Physician January 2006 47