Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
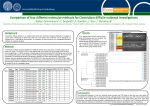
Journal club 2011.09.21 Type-Specific Risk Factors and Outcome in an Outbreak With 2 Different Clostridium difficile Types Simultaneously in 1 Hospital A. Goorhuis, S. B. Debast, J. C. Dutilh, C. M. van Kinschot, C. Harmanus, S. C. Cannegieter, E. C. Hagen, and E. J. Kuijper Clinical infectious disease. (2011) November 1 R2. Yoo, Jung-sun Introduction Clostridium difficile infection (CDI) due to polymerase chain reaction (PCR) ribotype 027 (type 027) : described worldwide This strain harbors the toxin genes tcdA and tcdB as well as binary toxin genes, and has a deletion at position 117 in the toxin regulatory gene tcdC C. difficile strains lacking toxin A (A-/B1) : increasingly found to cause outbreaks, especially in some Eastern European countries, South America, and Asia The most commonly found A-/B1 strain belongs to PCR ribotype 017 (type 017) Introduction They encountered a unique CDI outbreak due to type 027 and type 017 occurring simultaneously in a 980-bed teaching hospital in the Netherlands. In response, they performed a case-control study to investigate type specific risk factors and outcome of CDI patients, compared with control patients without diarrhea. They studied clonal dissemination using multilocus variable number tandem repeat analysis (MLVA). Methods Included all consecutively diagnosed CDI patients with a positive feces toxin test and culture of C. difficile from May 2005 through January 2007. For every CDI patient, they randomly selected a control patient without diarrhea, matched for ward, age, sex, admission period, and duration of hospitalization. They also included a group of control patients with non CDI diarrhea, as determined by a negative C difficile toxin assay. Methods Microbiological analysis : They used the number of differing loci and the summed tandem-repeat difference (STRD) between MLVA types as coefficients for the genetic distance Genetically related complexes were defined by a STRD ≤ 10 and clonal complexes by a STRD ≤ 2. CDI was defined as diarrhea in combination with a positive laboratory assay for C. difficile toxin A or B in stools Sever diarrhea : Occurred in combination with 1 or more of the following (bloody stools, hypovolemia, hypoalbuminemia (<20g/L), fever (T >38.0 C), leukocytosis and pseudomembranous colitis. Results 33 type-027 isolates (in blue circles) and 42 type-017 isolates (in green circles). The numbers between the circles represent STRD between MLVA types. Within the spanning tree, genetically related complexes (STRD ≤ 10) are marked in grey. Clonal complexes (with a STRD ≤ 2) are marked in yellow. Figure 1. Minimum spanning tree analysis of Clostridium difficile isolates typed by multilocus variable-number tandem-repeat analysis (MLVA) Results Table 1. Risk Factors Among Clostridium difficile Infection Cases and Non–Clostridium difficile Infection Diarrheal Patients Compared With Nondiarrheal Control Patients Results In the adjusted model, the association with high exposure to second-generation cephalosporins and clindamycin remained statistically significant (Case Vs control) Table 2. Antibiotic Use Among Cases and Non–Clostridium difficile Infection Diarrheal Patients Compared With Nondiarrheal Controls Results Significant risk factors, in both crude and adjusted models, were older age and hematological malignancy (Type 027 Vs other types) Significant risk factors, in adjusted models, were use of immunosuppressive agents and hematological malignancy (Type 017 Vs other types) Table 3. Risk Factors Among Patients With Type 027, Type 017, and Other (Non017/Non-027) Types Results High exposure to ciprofloxacin was specifically associated with type-027 CDI (Type 027 Vs other types) High exposure to clindamycin was specifically associated with type017 CDI (Type 017 Vs other types) Table 4. Antibiotic Use Among Patients With Type 027 or Type 017 Versus Patients With Other (Non-27/Non-017) Clostridium difficile Infection Types Results Patients with CDI had a higher 30-day mortality, overall in hospital mortality than both non-CDI diarrheal patients and nondiarrheal control patients. Table 5. Clinical Outcome Among Cases (All Types Combined), Non–Clostridium difficile Infection Diarrheal Patients, and Nondiarrheal Controls Results Patients with type 027 or 017 had similar overall mortality rates after 30 days, which were significantly higher than the mortality rate observed among patients with CDI due to other types. Table 6. Clinical Outcome Among Patients With Clostridium difficile Infection Due to Different Polymerase Chain Reaction Ribotypes Conclusion Type-specific risk factors were older age for both types 017 and 027, use of clindamycin and immunosuppressive agents for type 017, and use of fluoroquinolones for type 027 Patients with CDI had a higher 30-day mortality than both non-CDI diarrheal patients and nondiarrheal control patients. Patients with type 027 or 017 had similar overall mortality rates after 30 days, which were significantly higher than the mortality rate observed among patients with CDI due to other types. Patients with CDI have type-specific risk factors and mortality rates, with prolonged clonal spread of type 027 or 017.