Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
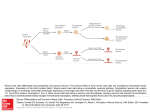
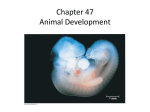
D22 – neural tube begins to close D24-cranial neural pore closes D26-28 caudal neuropore closes 4 types of spina bifida – oculta –small dimple, tuft of hair; no symptoms Cystica – extension of meninges outside of body, but no neural tissue; can have minor defects to complete loss of function from that level downward. Myeloschisis – cleaving or dividing, never hooked together, neural tissue is exposed; myelomeningocele Making a neural tube – have to have had gastrulation (trilaminar embryo); process by which we form ectoderm, mesoderm and endoderm. Notochord is formed by inducing factors. Invertebrates have a functional notochord. Notchord secretes factors like NOGGIN, etc. (don’t have to know all the induction factors) inducing overlying ectoderm to become neural epithelium. The neural epi, differentiates by rising off the surface and expanding off the cranial end into the neural plate. Along the edges, cellular prolif occurs, which makes the tissue rise up from surface of embryo. In the midline, envagination occurs digging the ectoderm into the mesoderm layer (V-shaped). As the envagination continues, rolling occurs until it forms a tube, dragging surface ectoderm with it, covering the neural epithelial in normal ectoderm and covers the neural tube inside the embryo. As lateral lips are coming together, specialized migratory cells spill out, neural crest cells migrate and go out into the body. Neural crest forms odontoblasts, ciliary mm of eye, schwann cells, truncocoronal septum, DRG sensory cells, peripheral ganglia, melanocytes, cartilages of the pharyngeal arches, precursors to the ossicles. Baby cannot hear until 3 wks before birth, ossicles are embedded in solid tissue and the Eustachian tubes are filled with fluid. Ciliary mm of the eye accommodate the lens, w/o it you have fixed focus, poor vision. Truncoconal septum error gives a common outflow to the heart and needs inutero surgery. DRG sensory cells don’t migrate there, you have no gross sensory system. Would die of an infxn from an injury you can’t feel. Adrenal medulla, need sympathetic ganglia here, to give fight or flight. Cardiac regulation (both symp/parasymp ganglia); point and shoot, parasympathetic and sympathetic (erection/ejaculation). Melanocytes, albinism, severe skin burns, bad vision. Pharyngeal arches from lots of structures in the face and neck. When we close the anterior neural plate, it is enlarged, big hollow tube, starts to fold in three places. As the embryo folds, the neural tube bends with it, isolating it into three areas, pro, mes, and rhombencephalon. 3 primary vesicles divide into 2ndary vesicles. Pro becomes tel (cerebral cortex), di (thalamus), mes (midbrain), met (pons and cerebellum) and myel (medulla). Don’t close the neural tube, calvarium does not form (comes from direct ossification from tissues surrounding the brain). Neural tube persists. Tel develops into lateral ventricles. Di dev into 3rd ventricle, Mes into the aqueduct. Met/myel 4th ventricle, SC gets the central canal. B/t mes and myel the neural tube is not complete, we have a layer of mixed neuroderm and mesenchyme called the telea choroidae (gives rise to choroid plexus, filters arterial blood and makes CSF). This tissue will end up lining the entire neural tube. CSF prod. in most ventricles. Failure to prod telencephalon, no cerebral cortex and connecting white matter = microcephaly. Can live and maintain normal body function, but this is like being born w/ a lobotomy. Failure for cephalad opening to close = meroencephaly (anencephaly). Mesencephalon issue, overproduce some cells, push inward, blocking off remnance of neural tube = non-communicating hydroencephalus, ventricles huge, di and tel very thin. Early closure of sutures, need them open for birthing and let the brain grow. Grows through myelination (oligos myelinate axons in the brain) and pruning (born with more neurons than we need). Sutures close early, we get herniations and malformations. Ant, post fontalnelle, foramen magnum, and nasal pathway, brain can herniate here. Grades of herniation: just meninges (CSF external to skull). Patterning – gradient setup b/t the basal (floor) and alar (roof) plate. SHH found in greater conc. in the floor (motor) and bonemorphogenic proteins found in greater conc. in the alar (sensory). This patterning of ventral being motor and dorsal being sensory continues into the midbrain, as seen in SC tracts. Know which cells develop from what lines. How do we get oligodendrocytes? Neuroepithelium dev into apolar neuroblasts (neurons), glioblasts (spongioblast, supt cells), and ependyma (surround brain tissue, CSF). Mesenchymal cells dev into microglia. Apolar neuroblasts dev into bipolar neuroblast which dev into unipolar neuroblast. Glioblasts dev into astroblasts and oligodendroblasts. Astroblsats dev into protoplasmic (grey matter) and fibrous (white matter) astrocytes. Oligodendroblasts dev into oligodendrocytes. Dr. Sarko Thalamus lesions, know groups, motor, those communicating w/ limbic, medial geniculate (auditory), Thalamic syndrome dejerine-roussy….end up w/ allodynia, pain/temp nucleus issue. Wernicke’s and broca’s have specific vascular supply, MCA sup/inf branches, don’t have to know specifics for other occlusions that could happen. Hypothalamus – know the balance, what nucleus regulates what, know diff subdivisions of pituitary gland and how the hypothalamus influences it, neural or vascular connection. Know oxytocin and vasopressin what they do. Circadian rhythm, sexual dimorphism nuclei. Know syndromes, korsikoff’s amnesias, main connectivities for limbic system. Basal ganglia – do a motor activity over and over again. If they are hyperkinetic, they might do an overexaggeration, hypokinetic they wouldn’t have enough motion. Motor cortex – look over FEF.