Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
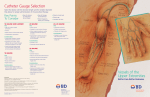
Nursing Orientation IV Therapy Insertion & Care of Peripheral & Central IV Devices Peripheral Intravenous Therapy – Insertion, Care and Removal - ID #: 500 It is the policy of the AtlantiCare Regional Medical Center that peripheral intravenous access and/or infusion therapy shall be initiated upon the order of an authorized Practitioner. The patient or legal representative shall be informed of potential complications associated with the treatment and have the right to accept or refuse treatment. The patient or legal representative shall also receive education relative to the prescribed treatment and plan of care. Peripheral intravenous access may be initiated by a registered nurse, licensed practical nurse, licensed radiologic technologist, or nuclear medical technologist with appropriate education and training. Peripheral intravenous access and care may be performed by a registered nurse. PROCEDURE INSERTION EQUIPMENT: Catheter (recommended size: 18g, 20g, 22g, or 24g) IV Start/ Dressing Change Kit Clean Gloves End cap extension set 2.5 ml 0.9% Sodium Chloride (NSS) (pre-filled syringe) Intermittent Infusion Extension set with cap Adult Patients – 2.5 ml 0.9% Sodium Chloride pre-filled syringe with end cap extension set Pediatric Patients – 2.5 ml 0.9% Sodium Chloride pre-filled syringe with end cap extension set Neonatal Patients – 0.5 – 1 ml 0.9% Sodium Chloride with end cap extension set Continuous Infusion Extension set IV solution with attached primed IV set IV pole Short Term Access (ie: For Contrast Media for IVP, MRI, CT Scan, etc) Extension set with cap Adult Patients – 2.5 ml 0.9% Sodium Chloride pre-filled syringe with end cap extension set Pediatric Patients – 2.5 ml 0.9% Sodium Chloride pre-filled syringe with end cap extension set stylus into the catheter. 1. Explain procedure to patient. 2. Wash hands thoroughly with antimicrobial hand washing agent to minimize possibility of infection. 3. For male adapter, fill extension set with normal saline prior to venipuncture attempt. For continuous infusion, have IV fluid on pole with tubing primed and within easy reach. If filter is necessary, attach. Check system for leaks, tears, cracks or particulate matter. 4. Place tourniquet 4-8" above intended puncture site; radial pulses should still be present. Palpate vein. Select IV catheter. 5. Prepare skin. If excessive hair is present, clip hair. Cleanse with Chloraprep applicator, rubbing vigorously and allow drying. Palpation of the insertion site should not be performed after the application of antiseptic, unless aseptic technique is maintained. 6. Put on clean gloves, rather than sterile gloves, for the insertion of peripheral intravascular catheters, if the access site is not touched after the application of skin antiseptic. Nursing Orientation IV Therapy 7. Hold skin taut, and insert IV catheter, bevel up, at a slight angle to the vein. Push needle through skin and vein wall at the same time. 8. Check flash back chamber for blood return to assure placement in vein. Advance needle 1/3 its length into the vein. 9. Remove tourniquet. Advance catheter full length of catheter into vein. 10. Place needles in proper disposal box. NOTE: Once the stylus has been removed, never re-advance or reinsert the stylus into the catheter. 1. 2. 3. 4. For male adapter, remove stylus, attach extension set and flush with 0.9% Sodium Chloride. For continuous infusion, remove stylus and attach IV tubing. Open clamp, allow fluid to flow to clear catheter of blood, then adjust rate. Remove gloves. Dress site as indicated or as appropriate for short term intravenous access. Place needles in proper disposal box. NOTE: A new cannula must be used in any subsequent attempt. SITE ROTATION Adult Patients - Peripheral sites must be rotated every 96 hours unless there is documented lack of venous access. Document reason if site not rotated every 96 hours. Pediatric Patients - Peripheral sites are not routinely rotated unless there is evidence of complications. Neonatal Patients - Peripheral sites are not routinely rotated unless there is evidence of complications. NOTE: Peripheral intravenous access, initiated in an emergency situation, must be re-started at the earliest opportunity. TUBING SET UP EQUIPMENT: Adult Patients: For Gravity Set-up: Primary Tubing 60gtt/ml or Primary Tubing 15gtt/ml End cap Extension Set For Secondary (Piggyback) Set-up: Secondary Piggyback Tubing End cap Piggyback Connector For Infusion Pump Set-up: Primary Tubing End cap Extension Set Secondary Piggyback Tubing For Patient Controlled Analgesia Infusion Pump Set-up: Obtain Cartridge and Tubing from the Pharmacy For Blood/Product Infusion Set-up: Y Type Blood Set Nursing Orientation IV Therapy Specialty Filter if Ordered Pediatric Patients: For Infusion Pump Set-up: 150 Burrette Pump Set (Soluset) – OL End cap T – Connector For Secondary (Piggyback) Set-up: 150 Burrette Pump Set (Soluset) – OL Secondary Piggyback Set End cap Piggyback Connector For Blood/Product Infusion Set-up: Hemoset Burrette Pump Set – OL Specialty Filter if Ordered FILTERS Refer to the Pharmacy web site for list of medications/ infusions/ patient populations that require filtering. NOTE: The Nurse is responsible for filtering the medication with the appropriate size filter before administering to the patient. When applicable, use filters provided by the Pharmacy. FLUSHING ►0.9 % NaCl is the standard flush for adult, pediatric and neonatal patients unless otherwise ordered by the Practitioner. ►0.9% NaCl flushes do not require a Practitioner’s order, will not be profiled by the Pharmacy, and will not generate tasks on the MAR ►Keep vein open (KVO) intravenous rates are to be converted to male adapters For Adult Patients 2.5 ml 0.9% NaCl every 12 hours and after each use For Pediatric Patients 2.5 ml 0.9% NaCl every 12 hours and after each use For Neonatal Patients For Neonates < (less than) 28 days of age, catheters may be flushed with either 1 ml 0.9% NaCl or 1 ml Heparinized Sodium Chloride 1 unit/ ml every 6 hours and after each use or as ordered by a Practitioner. Heparinized Sodium Chloride will be prepared by the Pharmacy and all ingredients are preservative free. For Neonates ≥ (greater than or equal to) 28 days of age, catheters may be flushed with 1 ml 0.9% NaCl every 6 hours and after each use or as ordered by a Practitioner. SITE CARE Site should be palpated daily for tenderness. If patients have tenderness at the insertion site or other signs of a possible infection, remove the dressing and visually inspect the site. Remove peripheral venous catheters if the patient develops signs of infection or signs of phlebitis (warmth, tenderness, erythema or palpable venous cord), or a malfunctioning catheter. Peripheral venous catheter dressings should be changed at a minimum of every 96 hours or if the dressing becomes loose, wet or soiled. 1. Explain procedure to patient. 2. Wash hands thoroughly with an antimicrobial hand washing agent to minimize possibility of infection. 3. Obtain IV Start/ Dressing Change Kit. Nursing Orientation IV Therapy 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. Put on clean gloves. Gently remove tape and dressing presently in place. Observe site for signs of infection: redness, streak formation inflammation, induration purulent drainage, foul odor skin ulceration If above symptoms exist, remove peripheral catheter and notify the physician. Palpate vein for hardness, tenderness, increased warmth, edema and/or pain. Cleanse insertion site with Chloraprep applicator in a back and forth motion and allow to dry. Remove gloves. Dress the site with transparent dressing. Document date, time, catheter gauge and initials directly on site dressing. Make a small loop of tubing away from patient's body and secure with 1/2" tape. TUBING CHANGE Tubings with continuous infusion should be changed every 96 hours. Tubings with intermittent infusion should be changed every 24 hours. Tubings utilized for TPN/ PPN should be changed every 24 hours. Tubings utilized for fat emulsions (i.e. Lipids) should be changed every 24 hours. Tubings utilized for propofol infusions should be changed every 12 hours and when the vial/bottle is changed. Patients who are on Protective Environment Precautions must have their tubing changed every 24 hours If a bolus of medication is withdrawn from the bottle/bag or needless ports on the tubing aseptic technique must be maintained. If aseptic technique is not strictly followed all tubing and the solution bag/bottle must be changed. NOTE: This procedure should be done in conjunction with site care/ site rotation when applicable. 1. Explain procedure to patient. 2. Wash hands thoroughly with an antimicrobial hand washing agent to minimize possibility of infection. 3. Prepare new IV bag with new tubing attached. Prime tubing. Clamp. Attach label indicating date tubing due to be changed. 4. Check container and tubing for leaks, cracks or particulate matter. 5. Put on clean gloves. 6. Remove tape. Clamp off present infusion. 7. While holding new tubing in hand with protective cap loosened, hold catheter hub between two fingers with alcohol swab and with a gentle twisting motion remove old tubing. 8. Swab end cap connector with alcohol for 15 seconds and allow to dry. 9. Insert new tubing into catheter hub. 10. Open clamp and allow IV fluid to infuse rapidly for a few seconds and then adjust to appropriate rate. 11. Proceed with site care as per established procedural guideline. Loop IV tubing and apply tape to secure. Utilize luer-locking devices on tubings as indicated. 12. Dispose of old container, tubing and dressing in waste container. Place any needles/ syringes in disposal box. REMOVAL 1. 2. 3. 4. 5. 6. 7. 8. Explain procedure to patient. Wash hands thoroughly with antimicrobial hand washing agent. Clamp off IV fluid. Put on clean gloves. Remove all tape from catheter site. Remove transparent dressing. Place gauze over site. Hold catheter hub, keeping hub in line with skin, gently and steadily pull catheter out. Examine catheter for breakage. Notify Practitioner for catheter breakage. Nursing Orientation IV Therapy 9. Using gauze pad, apply pressure for 1-2 minutes to stop bleeding from insertion site. Apply Band-aid. 10. Observe site for: Inflammation Red streaks Purulent drainage Foul odor Excessive bleeding If above symptoms exist, notify the physician. DOCUMENTATION OF PERIPHERAL ACCESS CARE Document indicated information on the Intravenous Therapy Flowsheet and/ or Specialty Flowsheet in the paper medical record, or document on the powerform IV Activity, Number of Attempts, Site, Laterality, Catheter Size (Gauge and Length), Catheter Type, Site Condition, Drainage Description (if applicable), Infiltration Score (0 – 4) (if applicable), Phlebitis Score (0 – 4) (if applicable), Site/ Line Care, Dressing/ Activity, Flow/ Patency, Equipment/ Supplies and Patient Response in the electronic medical record. Central Intravenous Therapy – Site Selection, Insertion, Care & Removal - ID #: 463 It is the policy of the AtlantiCare Regional Medical Center that central intravenous access shall be initiated by a physician and infusion therapy shall be initiated and maintained in accordance with the order of a physician or authorized prescriber. The patient or legal representative shall be informed of potential complications associated with the treatment and have the right to accept or refuse treatment. The patient or legal representative shall also receive education relative to the prescribed treatment and plan of care. SITE SELECTION PHYSICIAN DOCUMENTATION: Progress note: pre and post procedure note. If femoral site is chosen, documentation of reason behind choice will be included (subclavian vein stenosis, abnormal coagulation studies, catheter-operator’s skill, mechanical complications, etc.). Consideration of comfort, security, and maintenance of asepsis as well as patient-specific factors (e.g., preexisting catheters, anatomic deformity, and bleeding diathesis), relative risk of mechanical complications (e.g., bleeding and pneumothorax), and the risk for infection should guide site selection. In adult patients, a subclavian site is the preferred insertion site for a central venous catheter (CVC) for two reasons: (1) femoral catheters have been associated with a higher risk of deep venous thrombosis (DVT) and (2) there is an assumed presumption that femoral catheters are more likely to become infected because of proximity to the groin area and body waste products. The following guidelines for site insertion should be followed: 1. The subclavian vein will be the preferred site for insertion of the CVC. 2. Internal jugular will be the secondary preferred site for CVC insertion. 3. If femoral site is used, the catheter will not remain in place for longer than 48 hours. INSERTION: EQUIPMENT: Central venous catheter Chloraprep applicator CVP dressing kit Masks (for everyone in room except the patient) Sterile gown Sterile gloves Sterile drape 2.5 ml 0.9% Sodium Chloride (NSS) (pre-filled syringes) Syringes Local anesthetic (as ordered by practitioner) End cap port male adapter plug(s) Alcohol swabs Nursing Orientation IV Therapy 1. An assistant (either supervising or assisting with the procedure) is required to be at the bedside during insertion of central lines (with the exception of PICCs). 2. Verify signed and witnessed authorization is on the chart. In an emergency situation, informed consent may be waived. 3. Explain procedure to patient. 4. Place patient in supine position. Trim excess hair around the site with scissors. 5. Prime IV tubing and attach filter if applicable. 6. Wash hands thoroughly with hospital-approved soap and water or waterless alcohol-based cleanser. 7. Place towel roll along thoracic spine to elevate clavicle facilitating location of central vein and separating it from apex of lung. 8. Close door and keep traffic in and out of room to a minimum during line insertion. 9. The assistant (or supervisor) will help monitor for the safe insertion and adherence to maximal sterile barrier precautions of the central line and will complete the Central Line Insertion Practices checklist. The assistant will immediately notify the practitioner of any deviation of the critical steps as outlined in the checklist, stop the procedure if necessary, and assure compliance before the procedure can proceed. 10. Hand hygiene will be performed before and after palpating catheter insertion sites as well as before and after inserting an intravascular catheter. Palpation of the insertion site should not be performed after the application of antiseptic, unless aseptic technique is maintained. Hand hygiene must be performed with hospital-approved soap and water or waterless alcohol-based hand rub. 11. Open packages and assemble central line and maximal sterile barrier supplies. 12. Maintain aseptic technique for the insertion and care of intravascular catheters. 13. Sterile gloves will be worn; and these gloves will be changed if a catheter is being exchanged over a guidewire (thereby contaminating the gloves) and a new sterile catheter is then handled. 14. A mask, cap, sterile gown, and sterile gloves are to be worn by all healthcare personnel involved in the catheter insertion procedure. A cap and mask must also be worn by any personnel entering the room during the procedure. 15. Place a large sterile drape to cover the patient from head to foot. 16. Prepare clean site with a 2% chlorhexidine-based skin preparation. Alternative skin preps (1% tincture of iodine or povidone iodine) may be used if patient is intolerant to chlorhexidine. Apply skin antiseptic and allow to fully dry, which can be up to 2 minutes for povidine iodine. 17. Practitioner will prepare each lumen of catheter. Assist as necessary. 18. Assist with preparation of local anesthetic. 19. Advise patient to expect injection. 20. After anesthetic has taken effect, advise patient procedure will commence. Valsalva must be maintained until system is closed to prevent air embolus. 21. Instruct patient to perform maneuver (holding inspiration) after venous blood is aspirated into syringe and attempt to maintain until guide wire is removed from distal lumen and the system is closed. 22. Assist the patient on a ventilator by bagging to prolong inspiratory phase, if patient unable to perform valsalva. 23. Immediately after guide wire is removed from the distal lumen attach a primed End cap port male adapter plug and flush lumen. 24. Advise patient suturing is to anchor catheter in place. 25. Observe position of catheter by ring markings. 26. Apply dressing to site utilizing CVP dressing kit. Loop catheter under dressing before covering site. Date, time and initial dressing. 27. Assess patient's status and response to procedure. 28. Obtain chest x-ray to confirm catheter placement prior to use. Catheter may be used only after practitioner who interprets x-ray calls clearance to immediate care taker of the patient. Document verification of central intravenous catheter placement. 29. Radiologist performs formal interpretation of post placement x-ray, and calls any abnormality to patient’s immediate care taker. Note: Admitted patients with a cordis may only be in ICU, PCU or PCCU. INSERTION PHYSICIAN DOCUMENTATION: Progress Note: Pre and Post procedure note, and if line is aberrant, add description of assessment and interventions Nursing Orientation IV Therapy CARE TUBING SET-UP EQUIPMENT: Adult Patients: For Secondary (Piggyback) Set-up: Secondary Piggyback Tubing Clave Piggyback Connector For IV Pump Set-up: Primary Tubing Clave Extension Set Secondary Piggyback Tubing For Blood/Product Infusion Set-up: Y Type Blood Set Specialty Filter if Ordered Pediatric Patients: 150 Burrette Pump Set (Soluset) – OL Clave T – Connector For Secondary (Piggyback) Set-up: 150 Burrette Pump Set (Soluset) – OL Secondary Piggyback Set Clave Piggyback Connector For Blood/Product Infusion Set-up: Hemoset Burrette Pump Set – OL Specialty Filter if Ordered FILTERS Refer to the Pharmacy web site for list of medications/ infusions/ patient populations that require filtering. NOTE: The Nurse is responsible for filtering the medication with the appropriate size filter before administering to the patient. When applicable, use filters provided by the Pharmacy. FLUSHING: ►0.9 % sodium chloride (NSS) is the standard flush for adult, pediatric and neonatal patients unless otherwise ordered by the Practitioner. ►NSS flushes do not require a Practitioner’s order, will not be profiled by the Pharmacy, and will not generate tasks on the MAR. ►Heparinized flushes require a Practitioner’s order, will be profiled and dispensed by the Pharmacy, and will generate tasks on the MAR. For Adult Patients 2.5 ml 0.9% NaCl every 12 hours and after each use For Pediatric Patients 2.5 ml 0.9% NaCl every 12 hours and after each use For Neonatal Patients For Neonates < (less than) 28 days of age, catheters may be flushed with 1 ml 0.9% NaCl every 6 hours and after each use or as ordered by a Practitioner. Nursing Orientation IV Therapy For Neonates ≥ (greater than or equal to) 28 days of age, catheters may be flushed with 1 ml 0.9% NaCl every 6 hours and after each use or as ordered by a Practitioner . 1. Swab port with alcohol swab for 15 seconds and allow to dry. 2. Attach syringe by pushing and twisting until tight. Flush lumen with appropriate flush solution. As the last 0.5 ml is injected, clamp catheter and remove syringe. Never completely empty the syringe. SITE CARE: Central venous catheter dressings should be changed a minimum of every 7 days. If the dressing is soiled, loose, or damp, change it immediately. Any type of gauze dressing, including gauze under transparent dressing, must be changed at a minimum of every 2 days. Site should be palpated daily for tenderness. If patients have tenderness at the insertion site, fever without obvious source, or other signs and symptoms suggestive of a local or bloodstream infection, the dressing should be removed and the site thoroughly examined. 1. 2. 3. 4. 5. 6. 7. Explain procedure to the patient. Position patient to expose area of dressing to facilitate access to site. Wash hands thoroughly with hospital-approved soap and water or waterless alcohol-based cleanser. Don a surgical mask. Open kit maintaining a sterile field. Put on clean gloves and remove old dressing. Observe site for evidence of complications: purulent drainage foul odor catheter migration redness inflammation 8. Wash hands and put on sterile gloves. 9. Clean site and catheter with Chloraprep applicator provided using a back and forth motion to remove debris. Allow to dry. 10. Apply appropriate (transparent or gauze/ tape) dressing to site. Date, time and initial dressing. NOTE: For implanted ports, indicate date port was accessed and place a folded sterile 2x2 gauze pad under the needle, if necessary. Loop extension tubing and apply dressing. 11. Reposition the patient to level of comfort and remove procedure supplies. 12. Continue to observe for signs of complications and advise patient to report same. 13. Document the completed site care appropriately TUBING CHANGE: Tubings with continuous infusion should be changed every 96 hours. Tubings with intermittent infusion should be changed every 24 hours. Tubings utilized for TPN/ PPN should be changed every 24 hours. Tubings utilized for fat emulsions (i.e. Lipids) should be changed every 24 hours. Tubings utilized for propofol infusions should be changed every 12 hours and when the vial/bottle is changed. Patients who are on Protective Environment Precautions must have their tubing changed every 24 hours If a bolus of medication is withdrawn from the bottle/bag or needless ports on the tubing aseptic technique must be maintained. If aseptic technique is not strictly followed all tubing and the solution bag/bottle must be changed. NOTE: This procedure should be done in conjunction with site care when applicable. 1. 2. 3. Explain procedure to patient. Proper preparation of patient leads to better acceptance of treatment. Wash hands thoroughly with hospital-approved soap and water or waterless alcohol-based cleanser. Prepare new IV bag with new tubing attached. Prime tubing. Clamp. Attach label indicating date tubing due to be changed. Nursing Orientation IV Therapy 4. 5. 6. 7. Check container and tubing for leaks, cracks or particulate matter. Put on clean gloves. Remove tape which secures tubing connection to catheter hub. Clamp off present infusion. While holding new tubing in hand with protective cap loosened, hold catheter hub between two fingers with alcohol swab and with a gentle twisting motion remove old tubing. 8. Swab end cap connector with alcohol for 15 seconds and allow to dry. 9. Insert new tubing into catheter hub. 10. Open clamp and allow IV fluid to infuse rapidly for a few seconds and then adjust to appropriate rate. 11. Proceed with site care as per established procedural guideline. Loop IV tubing and apply tape to cover catheter hub and tubing connection. Utilize luer-locking devices on tubing as indicated. 12. Dispose of tubing and dressing in waste container. Place any needles/ syringes in disposal box. END CAP CHANGE: End Cap changes should be performed in conjunction with tubing change and as needed. 1. Wash hands thoroughly with hospital-approved soap and water or waterless alcohol-based cleanser. 2. Peel open end cap connector package at designated end, remove protector cap and prime with flush solution 3. Clamp catheter. If catheter does not have attached clamp, pinch tubing or use padded clamp. 4. Put on clean gloves. Clean junction between catheter and end cap with alcohol swab for 15 seconds. Allow to dry. 5. Remove old end cap connector. If any blood or debris remains on the catheter, clean with a new alcohol wipe. Blood on the catheter will cause the new end cap connector to be very difficult to remove. 6. Attach end cap connector to catheter by pushing and twisting until tight. Do not over tighten. 7. Unclamp the catheter. 8. Swab tip of end cap connector with alcohol swab for 15 seconds, allow to dry, attach flush-filled syringe by pushing and twisting until tight, and flush catheter. If flush is performed after blood drawing, use push/stop technique. BLOOD DRAW: Blood cultures should only be drawn from a central line when the provider is ruling out central line associated infection or if venipuncture is not possible or indicated for the patient. There are two methods for drawing blood: Vacutainer and Syringe method. Guidelines for both follow. This procedure refers to blood drawing from all central lines except dialysis catheters. NOTE: If patient is receiving a continuous infusion, an additional 10 ml 0.9% Sodium Chloride is required to clear line before withdrawing. EQUIPMENT: VACUTAINER METHOD/ SYRINGE METHOD: Vacutainer sleeve/Multiple sample Luer adapter 10 cc syringe Collection tube/Discard tube collection syringe (large enough to hold volume for needed blood sampling) Collection and discard tube Vacutainer sleeve/Multiple sample Luer adapter Double End cap connector 2.5 ml 0.9% Sodium Chloride (NSS) (pre-filled syringe) 1. 2. 3. 4. 5. Explain procedure to patient. Position patient supine and expose pigtails. Free pigtail from top of dressings. Wash hands thoroughly with hospital-approved soap and water or waterless alcohol-based cleanser. Assemble supplies on clean table. Put on clean gloves. TURN OFF ANY SOLUTIONS INFUSING INTO PORTS FOR ONE FULL MINUTE. Clamp off any infusion infusing into the proximal port. Blood withdrawal will be from the distal port if multi-lumen catheter is in place. If any solution has been infusing via blood drawing lumen, flush the lumen with 10 ml 0.9% Sodium Chloride before waste. Nursing Orientation IV Therapy VACUTAINER METHOD: Swab end cap connector with alcohol for 15 seconds and allow to dry. Insert Luer adapter into end cap connector. Collect discard specimen. Fill desired collection tubes. Flush lumen with 0.9% Sodium Chloride using push-stop technique. Resume any infusions or flush with heparin or saline as appropriate. NOTE: Discard specimen should be equal to the internal volume of the device in use. If unsure, 5 ml is an adequate amount. SYRINGE METHOD: Swab end cap connector with alcohol for 15 seconds and allow to dry. Insert empty syringe into End cap connector by pushing and twisting until tight and draw off discard. If fluid was running via lumen and a 0.9% Sodium Chloride flush was performed, this same syringe may be used for the discard specimen. Insert syringe for blood collection and draw off the necessary amount of blood for a waste. Discard this waste syringe Insert a different syringe and draw off the necessary amount of blood for testing. Flush lumen with 20 ml 0.9% Sodium Chloride using a push-stop technique. Transfer blood into appropriate collection tubes using multiple sample luer adapter and double connector. Attach blood filled syringe to one end of the double connector and the multiple sample luer adapter. Attach vacutainer to the other end of the double connector. Slide vacuum tube into the vacutainer holder and fill tubes. Resume any infusions or flush with heparin or saline as appropriate. IF UNABLE TO OBTAIN BLOOD: Have patient change position. Have patient cough with hands over head. Change vacutainer tube. Flush lumen with 3-6 ml 0.9% Sodium Chloride (NSS). If using vacutainer method, try syringe method. Send labeled specimens to laboratory. NOTE: With the Groshong catheter, the syringe method is the method of choice. When initiating blood flow, pull back 1 ml and hesitate to initiate flow. When flow begins, maintain steady pull on syringe to maintain flow. REPLACEMENT OF CENTRAL VENOUS LINES 1. Do not routinely replace central venous catheters to prevent catheter-related infections. 2. Do not remove central venous catheters on the basis of fever alone. Use clinical judgment to determine if the catheter should be removed. 3. Do not routinely replace catheters via guidewire exchange to prevent infection. 4. Do not use guidewire exchanges to replace a catheter suspected of infection. Use guidewire exchange to replace a malfunctioning catheter if no evidence of infection is present. Don new sterile gloves before handling the new catheter when performing a guidewire exchange. DOCUMENTATION OF CENTRAL ACCESS CARE: Document indicated information on the powerform: Activity Type, Access Type, Central Line Site, Laterality, External Catheter Length, IV Mid Arm Circumference, Site Condition, Drainage Description (if applicable), Infiltration Score (0 – 4) (if applicable), Phlebitis Score (0 – 4) (if applicable), Site/ Line Care, Dressing/ Activity, Flow/ Patency, Equipment/ Supplies and Patient Response in the electronic medical record. Nursing Orientation IV Therapy REMOVAL: Identification of nurses permitted to remove various Central lines by Location TYPE OF LINE LOCATION OF LINE CVU ICU TRAUMA PCU PCCU CATH LAB TELE/ MEDSURG Jugular Subclavian Femoral YES YES YES NO NO NO YES YES YES NO NO NO NO NO NO N/A N/A N/A NO NO NO Jugular Subclavian Femoral YES YES YES YES YES YES YES YES YES NO NO NO NO NO NO N/A N/A N/A NO NO NO Radial Femoral YES NO YES NO YES YES YES NO YES YES YES YES NO NO Femoral Only if arterial sheath not present Only if arterial sheath not present Only if arterial sheath not present NO YES YES NO Jugular Subclavian Femoral YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES N/A N/A N/A NO NO NO Arms YES YES YES YES YES N/A YES PA LINE Cordis A-Line Venous Sheath TLC PICC Line Type of Line and Procedure for Removal: CENTRAL VENOUS CATHETER (TLC) EQUIPMENT Goggles or face shield mask, and non-sterile and sterile gloves Occlusive dressing kit and Antiseptic solution Suture removal kit or sterile scissors 4 x 4 gauze pads 2 x 2 gauze pads 2 inch tape Sterile container for culture if ordered PROCEDURE Wash hands thoroughly with hospital-approved soap and water or waterless alcohol-based cleanser. Open the suture removal kit or sterile scissors and sterile gauze. Turn off and disconnect IV infusions. Don personal protective equipment i.e. goggles, mask, and non sterile gloves Place patient supine in slight Trendelenburg position. Place the patient flat if Trendelenburg position is contraindicated or not tolerated or if a femoral central venous catheter will be removed. If the catheter is in the femoral vein, extend the patients leg and ensure the groin area is adequately exposed. Have the patient turn their head away from the catheter which decreases the risk for air entry and reduces the transmission of microorganisms. Remove the catheter dressing and discard. Remove the non-sterile gloves, wash hands, and don a pair of sterile gloves. Carefully cut the sutures and pull the suture material through the skin. Instruct patient to take a deep breath in and hold it (if removing an internal jugular or subclavian catheter). This minimizes air from being accidentally drawn into systemic venous system. If patient is mechanically ventilated, Nursing Orientation IV Therapy withdraw the catheter during the inspiratory phase of the respiratory cycle or while delivering a breath via a bagvalve-device. Remove catheter as follows: a. Grasp the catheter with the dominant hand and withdraw the catheter in one continuous motion. This type of motion will decreases trauma to the vein. The distal end of the multilumen catheter should be removed quickly because the exposed proximal and medial opening could permit the entry of air. b. With the nondominant hand, quickly apply pressure over the puncture site with a sterile 4x4 gauze pad to prevent bleeding. c. If resistance is met, do not continue to remove the catheter. Notify the provider immediately. d. Maintain pressure for 5 minutes until hemostasis has been achieved. e. Pressure may be needed for a longer period of time if your patient has been receiving anticoagulant therapy or has abnormal coagulation studies. f. Once hemostasis has been achieved, apply a sterile occlusive dressing over site. g. Inspect the catheter after it has been removed to ensure that the entire catheter has been removed. Monitoring and Care: a. Monitor the patient’s vital signs, pulse oximetry, and level of consciousness before and after central line is removed. If an embolus is suspected, position the patient on the left side and in Trendelenburg and notify the physician immediately. b. Asses the dressing for the first 15 minutes after catheter removed then every 15 minutes for one hour for S/S of bleeding. c. Observe the catheter site for signs of infection. d. Remove the dressing and asses for site closure 24 hours after removal. Pulmonary Artery Catheter Removal (See policy 3011) Removal of Introducer/Cordis (See policy 3011) Removal of Arterial Line (See policy 3635) Removal or PICC Line (See policy 3416) Intraosseous Infusion - Policy #4631 Intraosseous (IO) needle insertion/IO infusion is indicated when standard intravenous (IV) insertion procedures fail or are insufficient to meet the clinical needs of the patient. While the insertion of an IO needle may occur anywhere in emergency situations, ongoing use is restricted to the emergency department, critical care unit and PCU. IO needles are to be removed as soon as secure venous access is accomplished, and may remain in place no longer than 24 hours. General Information Intraosseous (IO) infusion involves the insertion of a large bore (15 gauge) needle into the intramedullary space of a long bone and the administration of IV fluids, blood/blood products, and/or medications in situations when IV access cannot be accomplished in a timely manner. All fluids and medications that can be administered IV may be administered via the IO route. A variety of IO needles and devices are available, however, Policy #4631 addresses only the Vidacare EZ-IO driver and needles. An EZ-IO needle may be inserted by a physician, nurse practitioner or physician’s assistant who has received appropriate education and has demonstrated competency in its insertion. Nursing Orientation IV Therapy An EZ-IO may be used and removed by registered nurses, physicians, nurse practitioners, and physician’s assistants who have received appropriate education and demonstrated competency in use and removal. Patients with an EZ-IO in place will be cared for in the ED, Critical Care Units or PCU. A pink wrist band (provided by the EZ-IO maker) alerting caregivers that the device is present is applied when the device is inserted, and removed when the device is removed. Indications The EZ-IO is used: 1. Prior to peripheral intravenous (IV) attempts in the following situations: A. Cardiac arrest. B. Profound hypoperfusion with altered mental status. 2. When IV access cannot be established within 90 seconds (maximum of two (2) attempts) and one or more of the following is present: A. Altered mental status (Glasgow coma score 8 or less). B. Profound hypoperfusion/hemodynamic instability C. Need for medication-assisted intubation 3. When IV access is medically necessary and a peripheral IV cannot be established. Contraindications 1. Fracture of/in proximity to the proposed insertion site, e.g., tibia, femur, humerus 2. Infection at proposed insertion site. 3. IO attempt or placement within 48 hours in the same extremity. 4. Previous orthopedic procedure (e.g., joint replacement) involving proposed extremity. 5. Pre-existing medical condition involving the proposed extremity (e.g., tumor near site, severe peripheral vascular disease). 6. Inability to identify landmarks (e.g., morbid obesity, significant edema, excessive tissue). 7. Patient requires immediate MRI (metal in the device is incompatible with MRI). Possible Complications 1. Extravasation of fluid 2. Needle dislodgement 3. Compartment Syndrome 4. Fracture 5. Pain 6. Reduced Flow Rate 7. Infection NOTE: IO insertion may only be performed by a physician, nurse practitioner or physician’s assistant. An EZ-IO may be used and removed by registered nurses, physicians, nurse practitioners, and physician’s assistants who have received appropriate education and demonstrated competency in use and removal. Nursing Orientation IV Therapy After Insertion 1. Prime the IV tubing and attach it to either a pressure infuser device or IV pump. Note: All IV solutions must be infused under pressure. If a pressure infuser device is used, ensure the device is inflated to 300mmHg. If an IV pump is used, set the hourly infusion rate as ordered. Prime EZ-connect tubing or extension tubing with at least 10 ml normal saline. 2. If not obtaining a blood specimen, connect normal saline primed EZ-IO® connect tubing or extension tubing. If obtaining lab specimens, draw a full waste tube first (per policy 515), then obtain the specimen. Notify Lab that it is an IO specimen. 3. Unless contraindicated, patients who are responsive to pain should receive preservative-free and epinephrine-free 2% Lidocaine (cardiac lidocaine) injected slowly through the IO. A physician must place an order for the appropriate dose and frequency. The Lidocaine should be injected in 0.2 ml increments (before normal saline flush) in the following doses: A. Adult dose: 1mg/kg, up to 50mgs B. Pediatric dose: 0.5mg/kg C. DO NOT EXCEED 3mg/kg/24 hrs 4. The physician-prescribed dosage of 2% lidocaine without preservatives or epinephrine (cardiac lidocaine) must be infused slowly to prevent it from being sent directly into the central circulation. Medications intended to remain in the medullary space, such as a local anesthetic, must be administered very slowly until the desired anesthetic effect is achieved. 5. Using a syringe, flush the IO line rapidly with at least 10 ml of normal saline, and observe for swelling around the insertion site, indicating extravasation. Resistance to the flush is not uncommon and you will need to continue to flush in order to open up and move gelatinous intramedullary material. The inability to flush any solution indicates incorrect placement and another site should be pursued. 6. Confirming IO needle placement. A. IO needle is firm in the bone and fluids infuse without extravasation. B. Blood/marrow may be apparent in the needle, and may be aspirated; however, Inability to aspirate blood is NOT a reliable indicator of non-placement. C. If placement in doubt, leave needle in place with connecting tubing and syringe attached and attempt IO on alternate site or IV – do not attempt a 2nd insertion at the same site. 7. Attach EZ connect tubing to IV tubing. Begin infusion using either the pressure infuser device or IV pump. Infusions cannot be administered by gravity as it increases the incidence of the device becoming occluded. 8. Secure tubing to extremity with tape. Label site as IO, date & time inserted. 9. Apply pink EZ-IO alert band to the wrist. This serves to alert clinicians to the presence of the IO as well as a reminder to remove the IO within 24 hours of insertion. 10. Monitor EZ-IO® site and patient response, including need for additional IO Lidocaine. 11. Assess and document site/extremity assessment q 2h while the device is in use. 12. If the line is not being used, it should not be flushed routinely, but rather is flushed immediately prior to use as discussed above. Nursing Orientation IV Therapy Removal Procedure 1. To remove device, remove the extension tubing and stabilizer, attach a syringe to the IO needle, grasp the syringe and needle firmly, and simultaneously pull straight out and rotate the syringe and IO needle clockwise; this may require strength since the needle is in bone. 2. Apply an adhesive bandage or dressing to the site. 3. Remove colored EZ-IO alert band. 4. Observe site for evidence of infection or bleeding. Documentation 1. Document the IO site, flush and infusion as you would any other vascular access site, including position and security of the IO needle as well as condition of the site and extremity. 2. Removal: All IOs must be removed within 24 hours of insertion. Documentation should include site of IO prior to removal, condition of needle (ex. Intact, bent) when removed, and how the patient tolerated the procedure. Subject: Hospira Symbiq Infusion Pumps ID #: 4026 It is the policy of AtlantiCare Regional Medical Center that the Hospira Symbiq Infusion System/ Devices (pumps) will be utilized as described for intravenous fluid/ medication administration and in accordance with the manufacturer’s guidelines. Devices should be utilized for continuous infusions when warranted by: patient age, patient condition, prescribed therapy, care setting, type of access and including but not limited to: Patients 18 years of age Patients Patients 90 lbs in weight Patients that are medically unstable Patients receiving high volume infusions 150 ml/ hr Patients receiving “high risk” infusions Patients receiving TPN and/ or Lipids Patients receiving Potassium Patients receiving prescribed therapy via a central venous or arterial access device The integration of safety software and smart pump technology are intended to reduce the frequency of human error and enhance patient safety. Clinicians will administer prescribed therapy utilizing the smart pump technology and within the defined limits in the safety software whenever possible. In the event that a medication is not available in the Medication Library, or is a Non-Formulary medication, the “Other” option may be utilized. DEFINITIONS: Infusion System Device/ Pump: Infusion management device/ pump that allows controlled delivery of intravenous medications and that possesses safety software that checks programmed doses against preset dose limits specific to a medication and/ or clinical service profile. Nursing Orientation IV Therapy Clinicians are alerted to programmed doses that exceed these preset dose limits and may either require confirmation before beginning delivery (soft limit), or by not permitting delivery at all (hard limit). Medication Library: An established collection of medications that when utilized with the infusion system is intended to reduce the frequency of human error by restricting ways in which medications may be administered. Drugs available for selection within a Clinical Care Area (CCA) are based on the drug dosing recommendations for the service, unit/ department and/ or patient population. The content of the Medication Library is based on the Pharmacy and Therapeutics approved ARMC formulary and the established Standard Medication Drip Card concentrations. The design and product descriptions mirror the pharmacy information system’s formulary (Cerner Pharmnet) and selections display with the same safety features within the infusion devices (for example: look and sound alike medication names display in tall man lettering). The current and complete medication library is located on the Pharmacy web site. Refer to ARMC Policy ID # 4016 Hospira Symbiq Infusion System/ Pumps: Medication Library Clinical Care Area (CCA): A defined patient care service area or unit/ department that has been established and defined by the institution. A CCA may mirror a service line or unit/ department, or encompass a particular patient population or specific clinical situation. Available medications and medication limits are specific to the CCA. Drugs available for selection within a CCA are based on the drug dosing recommendations for the service, unit/ department and/ or patient population. For Example, but not limited to: the following are defined as CCAs: MET/ Code, Critical Care, 2 Meadows, OB, NICU, etc. Master Infuser Settings: System and/ or CCA specific infuser settings that have been determined and programmed at both the system and CCA levels based upon the clinical setting and patient population served. For Example, but not limited to: screen displays, pressures, alarms, etc. Soft Limit: Upper and/or Lower dose limits for the selected medication and selected CCA that may be overridden. Soft limits for a particular medication may vary between CCAs. Soft Limit Alert: An alert presented to the user when a selected medication dose is outside of the pre-defined Soft Limit value. The user may choose to over-ride or edit the dose in response to the alert. An Upper soft limit or Lower soft limit icon displays on the channel tab when the upper or lower soft limit is over-ridden. A yellow banner will display across the top of the screen to alert the user that they have over-ridden the soft limit. Hard Limit: Upper and/ or Lower dose limits for the selected medication and selected CCA that cannot be overridden. Hard limits for a particular medication may vary between CCAs. Hard Limit Alert: An alert presented to the user when a selected medication dose is outside the pre-defined Hard Limit value. Nursing Orientation IV Therapy Clinical Notes: A medication specific note that is defined in the medication library and that displays on the screen when the specific medication is selected. A Clinical Note may include, but is not limited to: interaction information, compatibility information, or high risk medication alert, or any type of information that enhances patient medication safety. PROCEDURE: Cleaning and Distribution: The Hospira Symbiq Infusion Devices/ Pumps will be cleaned and distributed via the established institutional processes. NOTE: It is important that these devices be cleaned with PDI Sani-Cloth AF for pumps in NON-ISOLATION patient rooms and PDI Sani-Cloth BLEACH for pumps in ISOLATION patient rooms. Medication Library Updates: Medication library updates are wirelessly transmitted to devices/ pumps via the wireless network. Devices must be plugged in to receive the wireless update. The device will display a message “New Drug Library” and the user may continue to use the device without interruption. When the device is turned off, it will display a message “Transfer Drug Library”. The user should select “yes” to install the new medication library at that time to avoid delays in start up the next time the device is needed. Medication Library/ System Change Requests: Suggestions/ Recommendations for additions, deletions, and/ or revisions to the medication library or system must be in writing utilizing the “Drug Library Change Request Form” which is located on the Pharmacy web site. Change requests will be reviewed by the institutional Pharmacy & Therapeutics Committee. Transfers: In an emergent situation, it is the responsibility of the higher level of care nurse to change the CCA to support the needs of that patient. Change in Level of Care Transfer: When a patient is transferred from one level of care to another, it is the responsibility of the higher level of care nurse to change the CCA to that of the receiving unit. Upon receipt of the patient, the receiving nurse must verify the order, medication/ infusion, and the CCA. Any discrepancies must be resolved immediately. Note: If a dual channel device/ pump is being utilized, the change and verification processes must be completed for both channels (A & B). When a patient goes to a procedural area (for example: Interventional Radiology, Cath/ EP Labs, etc.) it is not necessary to change the CCA. In the event that the set CCA does not support the needs for that patient or procedural area, the procedural area will change it to their designated CCA. Nursing Orientation IV Therapy Lateral Transfer: When a patient is transferred from one location to another, without a change in the level of care, it is the responsibility of the sending nurse to change the CCA to that of the receiving unit. Upon receipt of the patient, the receiving nurse must verify the order, medication/ infusion, and the CCA. Any discrepancies must be resolved immediately. Subject: Implanted Ports – Accessing and De-Accessing ID #: 482 POLICY: It is the policy of the AtlantiCare Regional Medical Center that a Registered Nurse will be responsible for accessing and de-accessing implanted ports. It is also the policy of the AtlantiCare Regional Medical Center that the following strategies to reduce tube/ catheter/ device misconnection errors will be utilized: 1. Discourage patients, families and non-clinical staff members from connecting/ disconnecting/ reconnecting any tubes/ catheters/ devices. 2. Trace tubes and catheters back to their origin before connecting/ reconnecting. 3. Label all high risk infusions and tubes/ catheters. These include: Neuromuscular Blocking Agent Infusions, Heparin Infusions, Insulin Infusions, Chemotherapy Infusions, Patient Controlled Analgesia Infusions, Epidural Infusions, Neonatal/ Pediatric Infusions. 4. Recheck connections and trace all tubes and catheters to their sources upon the patient’s arrival to a new setting or service as part of the hand-off process. 5. Route tubes and catheters having different purposes in different directions. This is especially important in the care of the Neonate. (Ie: Intravenous tubings routed toward the head; Enteral Feeding tubings routed toward the feet) ACCESSING THE IMPLANTED PORT EQUIPMENT: CVP Dressing kit Noncoring safety (Huber) needle (right angle bent tip - 20g or 22g with an attached extension set) ChloraPrep applicator Heparin flush, if ordered 10 cc NSS pre-filled syringe Clave extension set 1. 2. 3. 4. 5. Wash hands with antimicrobial soap. Identify the septum by palpating the outer perimeter of the port. Create sterile field using dressing kit. a. Open non-coring needle and extension tubing onto sterile field. Open Clave extension set onto sterile field. Attach NSS filled syringe to Clave extension set and prime. b. If continuous infusion is being initiated, attach syringe directly to extension set and prime set. Put on sterile gloves. Prep the skin over the port with Chloraprep applicator using a circular motion and extending from the center to the periphery and allow todry. NOTE: Allow Chloraprep to dry. 6. Stabilizing port between thumb and index finger of non-dominant hand, insert non-coring needle into the septum at a perpendicular angle maintaining sterile technique. Advance needle until reaching back of port. Nursing Orientation IV Therapy 7. Use 22g non-coring needle for infusions < 200 cc/hr. Use 19g or 20g non-coring needles for blood products or infusions > 200cc/hr. If implanted port to be used for blood drawing, a 19g or 20g non-coring needle is recommended. Check patency by aspirating blood into extension set and then flush with 10 cc NSS using a push-stop technique. If unable to obtain blood, have patient change position, cough or raise arms over head. If still unable to obtain blood return, flush the catheter with an additional 3-6 cc NSS and attempt to aspirate again. If resistance is met, withdraw needle and re-access port. If still unable to obtain blood return or flush, notify physician. NOTE: Blood return is an indication that both the catheter and needle are correctly placed. If troubleshooting procedures have been performed, and a blood return is still absent, infusion therapy should be withheld until the problem can be diagnosed and treated and a physician’s order is required prior to use. 8. Dress the site as indicated for a central venous access. CARE OF THE IMPLANTED PORT Non-coring needles and extension sets must be changed a minimum of every 7 days. Implanted ports dressings must be changed a minimum of every 96 hours and as needed. SPECIAL CONSIDERATIONS WITH CENTRAL VENOUS ACCESS DEVICES Sepsis – this is the most common life- threatening complication from CVAD’s. The following can increase a patient’s risk of catheter- related sepsis Poor insertion technique Multiple lumen catheters – the larger gauge introducer is needed to insert the catheter, trauma is created at the insertion site and due to the multiple lumens may be handled more frequently leading to increased microorganism introduction. Use of stopcocks Jugular or femoral insertion site Catheter material (body reacts to foreign body) Long term use Frequent dressing changes Poor Patient health Skin Preparation – using proper skin prep can decrease chances of sepsis. Air embolus -The risk is increased if while you’re manipulating the system, the patient’s intrathoracic pressure changes ie during coughing, sneezing, crying, or laughing. Also, if a break occurs in the CVAD above the level of the heart – 10 – 15ml of air can enter the bloodstream as a bolus. Signs and symptoms include – respiratory distress, increased heart rate, cyanosis, thready pulse, hypotension, and sudden change in LOC. What to do? Prevent any further air from entering by folding the catheterr back on itself and clamp the proximal portion or recap/rehook to IV line. PLACE patient on Left side and if possible place in a head down position. Administer O2, physician may aspirate with an Intracardiac needle. Venous Thrombus -When the inner layer of vein wall (the intima) is injured platelets and fibrin can accumulate and a clot can form. The patient can develop swelling on the affected side. The thrombus can also impede blood return from the head, causing the patient’s face to swell and become flushed. If you see these signs – Stop the infusion and notify the physician. Anticoagulation therapy is indicated and thrombolytic therapy may also be initiated. Nursing Orientation IV Therapy A component of General Nursing Orientation is to assess for competency in the areas of insertion and care of peripheral and central lines as well as IV Therapy administration calculations. The exam contains questions to support general knowledge regarding ARMC policy on care and insertion of IV’s. Additionally, during Unit based Orientation you will need to complete the Skills Form included in this packet. Follow the directions on the form. INFUSION RATES/CALCULATIONS: Included in the handout is a review of formulas with samples of dosage calculations. It will be a good review prior to the exam. The following information is for your review. It can be used as a resource as well as a review for the exam. Fluid Imbalances Hypovolemia – low volume of extracellular fluid. Dehydration occurs when the volume of fluid id reduced in both the extracellular and intracellular compartments. Hypervolemia – high volume of water in the intravascular fluid compartment. As this increases the fluid is redistributed into the interstitial space, leading to edema. Thirds spacing refers to the transmission of intravascular fluid into nonvascular fluid compartments where it becomes trapped. This causes a depletion of fluid in the intravascular space and may lead to hypotension, shock, circulatory failure. This condition is associated when serum albumin levels are low such as liver failure, burns, chronic kidney disease. How do you think we can reverse this condition??? FLUID REPLACEMENT SOLUTIONS Isotonic solutions – contains the same concentration of dissolved substances as is normally found in plasma. A solution with the same osmotic pressure as blood serum (body fluids) (275- 300). Isotonic fluids do not enter the cells because there is no osmotic force to shift them. Solutions include: 0.9% saline aka NSS, Physiologic Saline – contain amounts of sodium and chloride in physiologically equal amounts to that found in the plasma. 5% dextrose and water, aka D5W – This is isotonic when infused BUT, the glucose is metabolized quickly(starts out with osmotic pressure above 275 but then decreases to below 245 so that it can diffuse into cells), leaving a solution of dilute water (hypotonic salt solution) . Isotonic fluids are used clinically to treat hemorrhage, hypovolemia, extracellular fluid volume deficit, or as an initial treatment of dehydration. Lactated Ringers – Replaces electrolytes in amounts similarly found in plasma. The lactate helps maintain acid-base balance (not recommended in alkalosis and liver disease). CONTRAINDICATED in circulatory overload. Complications can include circulatory overload, which can include pulmonary edema. Hypotonic solutions – contains fewer dissolved substances than normally found in plasma. A solution with less osmotic pressure than blood serum (below 275). Solutions include 0.45% NS ( 155 con) aka 1/2NS, 2.5%Dextrose (130 con), .33% Saline (100 con), Hypotonic fluids are used to expand the intracellular fluid compartment. Hypotonic fluids that contain sodium are used to expand both extracellular and intracellular compartments. Because hypotonic solutions are dilute (have a lower osmolarity than body fluids), the water in the solution passes through the semipermiable membrane of cells, causing them to swell. This can temporarily increase blood pressure because it expands the circulating volume. The water may also pass through capillary walls and become distributed within other body cells and the interstitial spaces. How much of the hypotonic fluid enters the cells depends on whether the solution contains sodium. If a hypotonic solution does not contain sodium approximately 2/3 of the fluid infused enters the cells, the remaining 1/3 of the fluid stays in the extracellular compartment (vascular & interstitial). If a hypotonic solution contains sodium its distribution can best be understood by considering it to be normal saline with extra water added. The saline portion of the fluid distributes into the extracellular compartment; approximately 2/3 of the extra water enters the cells. Nursing Orientation IV Therapy They are used with patients who need to be rehydrated, ie, diarrhea and dehydration. CONTRAINDICATED in patients with anasarca and cerebral edema. Complications can include shock and increased ICP. Also, hypotonic solutions are NOT recommended for use in children - use isotonic or mildly hypertonic ie D51/3NS (335 con) instead. Hypertonic solutions – more concentrated than body fluid. They draw fluid into the intravascular compartment from the more dilute areas within the interstitial spaces and cells, causing them to shrink. A solution with higher osmotic pressure than blood serum (above 325). Solutions include: D5 1/2 NS (406 con), D5NS (565 con), D5RL (575 con) D5.225NS (329) Used much less frequently -10%Dextrose (D10W), 3% Saline, 20% dextrose in water CONTRAINDICATED with CHF and hyperosmolar states. Complications include Circulatory overload, because they pull fluid into the vascular space by osmosis resulting in an increased vascular volume particularly in clients with cardiac or renal disease. Nursing Orientation IV Therapy Check Your Knowledge Indicate if true or false 1______ Tubing and filters must be changed every 6 days. 2._____ Flush after blood withdrawal from an implanted port with 10cc saline using push stop technique 3.______ Always use a 10 cc syringe or larger when accessing a central line 4.______ The best way to prevent infection is through meticulous care of the system 5.______ The best way to prevent occlusion of a central line is through adequate flushing 6. Routine tubing should be changed every 96 hours except for TPN/PPN, lipids and neutropenic patients. 7. The skin’s degree of thickness should be assessed prior to venipuncture to determine whether it can adequately support an access device. T F 8. If a patient is cold veins tend to expand. 9. TPN, PPN, tubing changes should occur every 48 hours. T F T F 10. Which of the following areas should be avoided when selecting an intravenous access site 1. 2. 3. 4. a. b. c. d. An extremity with an AV shunt or fistula Damaged skin area Affected arm of an axillary dissection The non affected side of a stroke patient 1, 2, 3 1, 3, 4 1, 2, 4 None of the above 11. The bevel should always point down when inserting the cannula T____ F___ 12. Date of insertion, catheter size, direction of catheter, and the initials of person performing venipuncture are to be placed on the dressing. T___ F___ 13. Lipids should always be filtered. T ___ F ___ 14. Document site care on the IV flow sheet. T ___ F ___ 15. When flushing a pediatric patient’s male adapter with Heparin it is not necessary to have 2 nurses double check the heparin dose. T F __ 16. You must always check for placement of a Central Line prior to using by Radiologist confirmation of placement T _____ F _____ IVTherapyNO-13Rev070213