Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
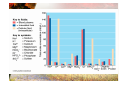
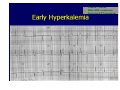
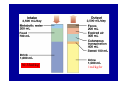
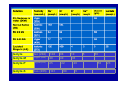
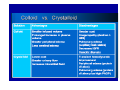
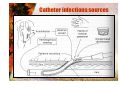
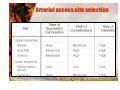
Fluid and Electrolyte Balance Pervin BOZKURT Professor of Anaesthesiology Total Body Water (TBW) Male 60% 50% Newborn 80% Aged <50% 40% TBW 60% TBW • Semipermeable membranes – Water in and out freely – Acts as barrier to other substances • Osmosis is movement of water from less concentrated solution to more concentrated solution in semipermeable membranes • Osmolarity: is amount of solute per volume of solvent (mosm/L) • Osmolality ( mosm/kg) Serum Osmolarity Normal: 280-300mosm/L What keeps water in balance? • • • • THIRST Hormones (affect balance of water and Na) – ADH: retains or secretes water – Aldosterone: • ↑causes Na and water retention and K loss • ↓causes Na and water loss and K retention – ANF Plasma protein – Albumin (major plasma protein) – Regulates blood volume – Prevents water in blood from diffusing into interstitial fluid Kidneys – Control concentration and volume of blood by removing water and waste (1 - 2 l urine daily) – Regulate blood pH – Filter 170 l of plasma Negative Balance • volume depletion (hypovolaemia) – total body water ↓, osmolarity normal • haemorrhage, severe burns, chronic vomiting or diarrhea • dehydration – total body water ↓, osmolarity rises • lack of drinking water, diabetes, profuse sweating, diuretics – infants are more vulnerable – affects all fluid compartments – most serious effects: circulatory shock, neurological dysfunction, death Why Hypovolemia is Important for Anaesthesiologist • PTs are more vulnerable to vasodilation – (-) inotropic effect of inhalation agents and barbiturates – Histamine release (morphine, meperidin, NMB) • Dose requirements decrease—volume of distribution drugs decrease • Regional anesthesia esp. Central blocks are contrandicated – Due to extensive sympathetic block Hypervolemia • • • • Increased fluid intake Decreased fluid excretion Stress—Secretes ADH Importance for anesthesia – Main role of anesthesiologist to achieve gas exchange – Hypervolemia- pulmonary interstitial edema, alveolar edema, pleural fluid and ascitis –cause derangements. cations Na+ K+ Ca2+ Mg2+ anions 142 4.5 2.5 1 ClHCO3PO42SO42protein organic acids 150 100 27 2 1 15 5 150 ↑ anion gap: ↑ protein, organic acids, PO42-, SO42↓ Ca2+, Mg2+ abnormal anion - eg drugs (salicylate, methanol, ethanol etc) cations Na+ K+ Ca2+ Mg2+ anions 142 4.5 2.5 1 ClHCO3PO42SO42protein organic acids 150 100 27 2 1 15 5 150 ↓ anion gap (rare): ↓ unmeasured anion (hypoalbuminaemia) ↑ Ca2+, Mg2+ abnormal cation - IgG myeloma Sodium Na • Major extracellular cation • Affects water distribution – ↓Na level (promotes water excretion) – ↑Na level (promotes water retention) Na • Maintains osmotic pressure of ECF • Maintains acid-base balance • Promotes neuromusc. function • Influences Cl and K levels Na Na Na Na Hypernatremia • For elective surgery Na <150mEq/mL • Consequences in anesthesiology practice similar to HYPOVOLEMIA Treatment according to derangement SLOWLY Calculation of water deficit in hypernatremia • Normal TBW X 140= Existing TBW X Plasma Na • Example: • 70kg M N a160 mEq/LT. What is the amount of fluid deficit • (70X0.6)X140= Existing TBW X160 • Existing TBW=36.7 • Fluid loss = (70X0.6)-36.7)=5.3 • Give 5% D in wter in 48 hours hypernatraemia - management general principles correct slowly to avoid cerebral oedema - 0.5 - 0.7 mmol / l / h treat underlying cause Hyponatremia • For elective surgery Na >135mEq/mL • Consequences in anesthesiology practice • similar to HYPERVOLEMIA • Special issue : TURP syndrome Hyponatraemia - emergency treatment controversial rapid correction → central pontine myelinosis hyponatraemia → encephalopathy ( if severe and rapid onset) Eg. TURP Syndrome Potassium • Major intracellular cation – Maintains cellular osmotic equilibrium – Regulates muscular activity (cardiac/skeletal muscles) – Maintains acid-base balance • Na and K relationship:↑in one will cause↓ in the other – Body usually conserves Na – But has no method to conserve K – Kidneys will excrete K (even in K depletion) Daily diet - 40mEq of K Normal diet: 60-100 Banana 12.8 Dried apricots 5 OJ 11.4 Broccoli, carrots Tomato 5-10 Meats 12 Scallops 30 Hypokalemia Paralytic Ileus Postural Hypotension Cardiac dysrhythmias Increased sensitivity to Digitalis toxicity Muscle cramps and tenderness Paralysis Confusion Depression • For elective surgery K >3.5mEq/L Metabolic Alkalosis • K– – – – – supplements Liquid: KCL 10 - 20, 40 mEq/15cc Tablets: KCL (extended-release) Slow-K K-Lyte Single dose should not exceed 20mEq • • • Peaked T waves Wide QRS complexes Depressed ST segments Treatment of Hyperkalemia • Avoid foods containing K • Avoid drugs – containing K- crystalized penicillin – increasing K- sucsinilcholine • Avoid intravenous solutions containing K – Ringer’s Lactate – Isolyte ( P, M, S) – Kadalex Bicarbonate H+ ions moves oppositely to K Na HCO3- (50 mmol iv) (if severe acidosis pH <7.2) Clinical effects hypokalaemia hyperkalaemia neuro-muscular weakness, paralysis weakness, para depressed tend reflexes cardiac arrhythmias ECG changes arrhythmias ECG changes GI ileus ileus nausea, vomitin pain renal tubular dysfunction, polyuria - metabolic alkalosis acidosis Clinical effects hypokalaemia prolonged PR T-wave flattening/inversion prominent U waves hyperkalaemia tall, peaked T wave QRS widening QRS fusion with T wave producing sine wave AV dissociation, VT, VF “Crush Syndrome” Criticisms After Marmara Earthquake • “Crush syndrome was not properly recognized in some cases.” • “Most of these patients received only 2,000 to 3,000 mL/day of infused fluids during the initial 3 days.” • “…we need to avoid such failure to recognize crush syndrome and to start infusion without Oda et al, J Trauma March 1997 delay.” Definitions • Direct Mechanical Crush - physical disruption and immediate death of cells • Crush Injury - interference with normal membrane function and circulation of blood to an area of tissue which leads to cell death • Compartment Syndrome - a form of crush injury caused by swelling inside a muscle body surrounded by inelastic fascia • Crush Syndrome A group of systemic manifestations that occur after crush inhury. Blood then returns to the affected part after the compressive force is removed allowing toxic products to enter the systemic circulation. Pathophysiology • Crush injury interrupts the supply of blood which causes cells to function anaerobically • Integrity of cells breaks down causing them to become leaky which results in swelling, rupturing or otherwise being destroyed • Extreme force causes immediate muscle cell disruption and death Pathophysiology • Mechanisms cause buildup and cellular release of: – – – – – – – Lactic Acids – Oxygen free radicals Potassium – Superoxides Myoglobin – Histamines Uric Acid – Leukotrienes Phosphate – Peroxides Lysozymes Enzymes (CPK and others) Pathophysiology • As patient is extricated, the compression force is lifted allowing blood to re-perfuse the injured area. • Patient dies because of one or more of the following primary causes: – – – Hypovolemia Dysrhythmia and Cardiotoxicity Renal Failure Causes of Death • Hypovolemia – – ruptured blood vessels bleed freely capillaries leak fluid into tissue (third spacing) • Dysrhythmia and Cardiotoxicity – – – high blood toxins return to central circulation severe acid load causes Ventricular-fib high K level causes dysrythmias • Renal failure – – enzymes digest cell membranes myoglobin precipitates in kidney tubules Post-Extrication Assessment – Symptoms may be subtle and develop gradually • entrapped limb may appear dusky to black in color – – – ecchymotic lesions marked edema/swelling +/- distal pulses • watch for symptoms of hypovolemia • arrhythmias - enlarged or “peaked” T waves; prolonged PR or QRS complex; loss of P wave; PVC, V-tach or V-fib • urine may appear dark reddish-brown like coca-cola Treatment I. Patient monitoring: hypovolaemia (arterial pressure, urine output), electrolyte disorders and serum creatinine kinase levels II. Volume replacement: target of 200 ml/h urine output – Physiological serum while muscle remains under pressure – After removal of patient from the subsidence and haemodynamic stabilisation, give a liquid formula of 75–110 mmol/l NaCl in 5% dextrose( 5%dextrose in water + 40 mEq NaHCO3 ( 4 amp NaHCO3) + 10g/l mannitol (50ml 20% mannitol) – An average of 12 litres per day should be given for 3 days – Na HCO3 stopped at 36 h III. If the systemic pH >7.5, then acetazolamide is administered IV. If diuresis has still not been achieved, CVP monitoring should be instituted V. If no response occurs, furosemide is used (40 mg, up to a maximum of 200 mg) VI. Haemodialysis Management: Hypovolemia • Large bore I.V.s (NS preferred); Fluid replacement prior to extrication. – – consider all injuries including possible ICP and cardiac overload consider high volumes of NS may lead to chemical imbalance Management: Renal Failure • Increase urine output – – – fluid replacement alkaline diuresis catheterize patient ASAP to monitor output • Consider availability of dialysis equipment Additional Considerations • Immobilization of crushed parts • Dress wounds meticulously to prevent infection; consider I.V. antibiotics • It is imperative that the rescue team be made aware of the importance of treating the patient PRIOR to extrication Calcium • Daily amount needed: 1gram – 98% (bone & teeth, small amount in ECF) – Ca able to shift in & out of these structure • Needed for: – Neuromusc. & enzyme activity – Skeletal development – Blood coagulation • Body absorbs Ca from GI tract • Vit. D needed • Excreted in urine & feces Causes, Signs & symptoms Hypercalcemia Hypocalcemia Diet Renal failure Loss of Ca from bone S/S Cardiac arrest (↑ST segment) Deep bone pain, flank pain Diet Renal failure Mg deficit S/S Depressed ST segment Tetany, tingling Trousseau’s, Chvostek’s signs Magnesium “ forgotten electrolyte” (ICF) Signs & symptoms Hypermagnesemia (↑4mEq/L) CNS: insomnia Hypomagnesemia (NIDDM,ETOH) Drowsy, lethargic, coma CV: ↓P, BP, cardiac arrest Arrhythmias Neuromusc: ↓reflexes, weakness Weakness, seizures, tremors Resp. depression 30-35ml/kg 1ml/kg/hr What happens to fluids given İV? IV therapy • Goals ¾Maintain hydration ¾Replace fluids (water, calories, protein, vitamins/minerals, electrolytes) ¾Restore acid-base balance ¾Restore blood volume ¾Provide access for medications IV fluids • Isotonic – Osmotic pressure same as body fluid • Expands & stays in intravasc. space • Uses: bloodloss, hypotension ¾ Normal saline (NS) 0.9% ¾ LR (lactated Ringer’s): Na, K, Cl, Ca, lactate ¾ D5W (fluids, calories) acts as hypotonic – Hydrates cells, depletes circ. System • Hypotonic – Less osmotic pressure than ICF (cell swells) • Hydrates cells but depletes circ. System • Hypertonic – Expands intravascular space,depletes intracellular compartments (cell shrinks) Isolyte Iso (294) 140 Isolyte-M Hyper (400) 40 Isolyte-P Hyper(350) 25 Isolyte-S Iso (295) 141 98 40 22 98 10 5 50 35 20 5 50 23 Colloid Solutions Albumin Dextran40 Rheomacrodex ( microcirculation) 70 Macrodex Hydroxyethystarch Isohes Expahes Varihes Gelatine Gelofuscine İsotonic Contain Na and Cl 154 mEq/L Catheter types • Peripheral • Central – Short term • Cvp • Swan • Dialysis – Long term • Ports Catheter infections:sources Peripheral IV insertion Peripheral IV insertion Peripheral IV insertion IV Complications • Infiltration – Fluid outside vessel causing swelling, pain, little or no IV flow • Catheter shear – Piece of catheter separates • Air embolism – Air enters blood stream (10-100 cc have been fatal) • Infection – Localized or systemic Home Temporary central venous catheters Seldinger technique • Trendelenburg position • Stiff,soft tipped guide wire • Flouroscopy • CXR Catheter Complications : early • Infections • Injury – Cardiac,lymphatic, • Malposition • Air embolism – Insertion and removal – Cardiovascular collapse, wheel mill murmur – Left lateral decubitus positioning, air aspiration if possible, thoracotomy if necessary Arterial access • Hemodynamic monitoring • Frequent blood gas evaluations • Chemotherapy infusion – Limb perfusion – Hepatic arterial infusions Arterial access:site selection