Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
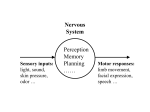
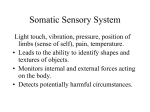
Lecture 19 revised 03/10 The Somatic Sensory System Skin- the largest sensory organ we have Also protects from evaporation, infection. Skin types: hairy and glabrous (e.g. back vs. palm of hand) 2 major somatic sensory systems1- mechanical stimuli- light touch, vibration, pressure 2- for pain, thermoreception Types of sensory nerve endings underlying sensitivity: free nerve endings encapsulated nerve endings- some nerve endings associated w/ specializations/specialized transducing cells that act as filters/amplifiers in either case, stimuli cause change in receptor membrane permeability; results in a receptor potential which can in turn cause action potential(s) strength of stimulus is conveyed by rate of resulting action potential discharge Mechanoreceptors Thought to contain mechanosensitive ion channels (not well understood) with gating depending upon on stretching or changes in tension of the surrounding membrane Mechanoreceptors specialized to receive tactile information fig. 9.5, Table 9.2 Rapidly adapting- sensation of dynamic qualities of mechanical stimuli-i.e. change Fig 9.4 Meissner_s corpuscles- about 1/10 the size of Pacinian corpuscles Capsule composed of several Schwann cell lamellae around nerve ending sense rough texture- e.g. cloth nestled between dermal papillae 30-50Hz sensitivity ~40% of receptors innervating human hand; most abundant receptors of glabrous skin-you tend to use this skin to examine things, thus lots of rapidly adapting receptors note- when you want to carefully discriminate textures, you will explore them so rapidly adapting receptors are effective Pacinian corpuscle- can be 2 mm long and 1 mm in diameter -sense pressure/vibration- e.g. music from speaker; vibration/tickle sensation when stimulated -connective tissue, 20-70 layers surrounds axon (or more than one axon in some cases) 250-350 Hz sensitivity, lower threshold and more rapid adaptations than Meissner's corpuscles ~10-15% cutaneous receptors of human hand thought to detect fine texture, other stiumuli causing high frequency vibrations of skin similar receptors in heron legs (vibes in water), bird wings (air currents) Hair follicle receptors- can be either slow or rapidly adapting Slowly adapting-give info regarding persistence of a stimulus: Merkel_s disks- nerve terminal and flattened, non-neural epithelial cell- epithelial cell makes synapse-like junction with nerve terminal and may be the mechanically sensitive part about 25% of mechanoreceptors of hand located at tips of dermal papillae stimulation in humans produces sensation of light pressure-presumed to underly static discrimination of shapes, edges, rough textures Ruffini corpuscles- not as well understood; deep in skin (and ligaments and tendons); long axis oriented parallel to stretch lines of skin; also found in ligaments and tendons ~20% of mechanoreceptors in hand don't elicit any particular sensation when stimulated probably respond primarily to internally generated stimuli Two-point discrimination fig 9.4 1-2 mm at tips of fingers, to 40 mm on forearms; try a paper clip experiment with a friend, bend the points to different distances, see when can detect as 2 stimuli without looking reflects differences in density of receptor distribution; makes sense Receptive field Varies from 1-2mm at tips of fingers, 5-10mm on palm Reflects area of skin over which a sensory neuron responds-variable because density of receptors varies; want smaller receptive fields where receptors are more dense to allow 2 point discrimination The information pathway to the brain Fig 9.1, 9.8 DRG neurons= first order neurons because they initiate the sensory process DRG neurons send a process thru dorsal root into dorsal horn of spinal cord mechanosensory axons bifurcate into ascending and descending branches, send collaterals to laminae III-V (Rexed_s) in several adjacent spinal segments- latter are responsible for monosynaptic reflexes (e.g. knee jerk); major branch is ascending in dorsal column (posterior funiculus; plural is funiculi), ascends all the way to medulla where it synapses on neurons of nucleus gracilis (lower body) or nucleus cuneatus (upper limbs, trunk, neck). Nuc gracilis and cuneatus referred to collectively as dorsal column nuclei dorsal column lesions have only modest effect on simple tactile tasks but impede ability to detect direction and speed of tactile stimuli as well as proprioception- deficit presumably relatively mild because of presence of spinothalamics. Dorsal column nuclei project to ventral posterior lateral nuc. of thalamus Sensory info from face- via trigeminal nerve (cranial n. V; has opthalmic, maxillary, mandibular branches - each branch innervates specific territories on face and head, including teeth and mucosa of oral and nasal cavities), cell bodies in trigeminal ganglion; projects into brain onto components of the trigeminal brainstem complex= principal nucleus (processes mechanosensory stimuli) + spinal nucleus (painful and thermal stimuli; corresponds to dorsal horn spinothalamic neurons) trigeminal brainstem nuclei neurons (2d order) project to ventral posterior medial nuc. of thalamus neurons of VP thalamus project to layer IV of somatic sensory cortex Dermatomes Box 9A each DRG innervates a field on surface of body called a dermatome DRG dermatomes overlap (larger than in picture) shingles (Herpes zoster; chicken pox virus) - remains dormant in sensory neurons; sometimes infection in single DRG reactivated, inflammation on body area innervated corresponds to dermatome dermatomal maps vary between individuals; overlap more extensive for touch, pressure, vibration than for pain and temperature- thus testing for pain gives more detailed info about location of a segmental nerve injury than testing for touch pressure or vibration segmental distribution of proprioceptors follows pattern of muscle innervation more closely than dermatomal map dermatomal maps vary between individuals; overlap more extensive for touch, pressure, vibration than for pain and temperature- thus testing for pain gives more detailed info about location of a segmental nerve injury than testing for touch pressure or vibration Mechanoreceptors specialized for proprioception- i.e. "receptors for self" fxn- give detailed and continuous info about position of limbs and other body parts in space Muscle spindle afferents- provide info regarding muscle length- fig 9.7 number of spindles varies according to muscle type- e.g. very dense in extraocular and finger muscles; much less dense in large muscles of the leg- why? Output signal depends on many factors; particularly input from CNS; we'll discuss when we talk about motor control innervation of nuclear chain fibers and nuclear bag fibers by gamma efferents allows tuning of the spindle these are the receptors responsible for the knee jerk reflex (can suppress the reflex and annoy doctor w/ CNS input) Golgi tendon organs- provide info regarding muscle tension distributed among collagen fibers that form the tendons joint receptors-rapidly adapting; gather info regarding joint position; poorly understood ; resemble Rufinni_s endings, Golgi tendon organs and Pacinian corpuscles; present in joint capsule and ligaments cortex has somatotopic maps- representation of body arranged w/ surface of cortex; can determine by stimulating body and seeing which neurons respond Fig 9.10, 9.11 info becomes progressively more and more integrated e.g. from response to a single finger, to receptive field corresponding to multiple fingers; preference for direction of stimulation; and more complex, e.g. specific shape adjacent secondary somatosensory cortex (located lateral to S1, can see it by pulling back temporal lobe and peeking under S1) projects to limbic structures (e.g. amygdala and hippocampus) also projections between motor ctx and somatosensory ctx massive descending projections between somatosensory ctx and thalamus, brainstem, spinal cord (actually outnumber ascending projections) thus ctx modulates ascending flow of information-modulates its own input the synapses as info ascends aren_t just relays; info is processed, e.g. sharpened as it moves thru dorsal column nuclei and thalamus Somatotopic maps aren’t completely stable- fig. 24.15 Rapid changes of synapse strength are likely to underly some changes of this nature- maps can rearrange even w/ a peripheral nerve anesthetic