Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
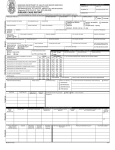
Report of an Individual Safety Information (ISI) 1) Reporter Name (First/Last) Address 2) Patient Phone / Email / Fax Country Initials Gender Select 3) Reaction Occupation: Date of Birth/Age at onset/ Age Category Height (cm) Diagnosis Weight (kg) Date of Onset Reaction description, signs & symptoms, possible causes, progression, treatments, relevant medical history, investigations, disease registry name Please check if the reaction led to one of the followings: Death Life-Threatening Inpatient/ Prolonged Hospitalization Congenital Anomaly/ Birth Defect Persistent or Significant Disability / Incapacity Suspected transmission of infectious agent Required Intervention to Prevent Permanent Impairment or Damage (Devices) 4) Action Taken None Dose changed specify: Discontinued Did reaction reoccur after drug was restarted? Corrective treatment was required, 5) Outcome of Reaction: Recovered Yes No Did reaction abate after drug was stopped or dose changed? Unk Yes No Unk specify: Date of Resolution, if not available, reaction duration: Recovered with sequelae: specify: Fatal, specify date & cause of death. _ ___ Recovering Not Recovered __________________________________________________ Autopsy: Yes No Unknown Unk 6) Medication/Device potentially causing the reaction Trade/Brand name & or INN (strength & form) Indication Dosage/Unit/ Freq/ amount Route Treatment start date Treatment stop date /duration Lot/Batch Company (C) or noncompany (NC) Select Select 7) Other Medication/ Device Select Select Select Select Case submitted to any Regulatory Authority Signature / Date: First received Date: Name: ( First /Last) Local PV received Date: Name: ( First /Last) Local PV Ref. No. Local PTC No. Global PTC No. AWARE Case No. Grey fields for Company use only. (Please send this completed page to [email protected]. Please contact +91- 98200 69843 for any assistance) Unsolicited Individual Safety Information (ISI) Report Form and Instructions QSD-001034 Version Number: 9.0 1/7 General Instructions for Individual Safety Information Form Completion These instructions are designed to assist you in completing this Individual Safety Information (ISI) form used by Sanofi to collect and document safety information on their products. Although not all fields are detailed in the following instruction, all of the fields must be completed if applicable. Type or print using black ballpoint pen only. Make changes or corrections by drawing a single line through the ERROR. Initial and date all corrections. DO NOT use correction fluid. Answer questions as concisely as possible. If the safety information does not fit into the structured fields, you may use additional pages as necessary. Ensure each additional page includes the page number and the total number of pages forwarded. Enter dates in DD-MON-YYYY format (e.g. 20-Apr-2011). Partial dates are acceptable. For example: Apr-2011 2011. Do not fill out Grey fields on the ISI form. They are for Sanofi use only. Unsolicited Individual Safety Information (ISI) Report Form and Instructions QSD-001034 Version Number: 9.0 2/7 Section 1): Reporter Field: Instructions for completion: Reporter Name Enter the primary reporter’s First and Last Name or initials as appropriate. This field should be anonymized before transmission to Core Teams. Phone / Email / Fax Enter the primary reporter’s Phone number, Email address, and/or Fax number, as available and as appropriate. Address Enter the primary reporter’s address including street address, state, country, as appropriate. Country Enter reporter’s country. Occupation Enter reporter’s occupation, e.g. consumer, physician, nurse, dentist, pharmacist… Section 2): Patient Field: Initials Instructions for completion: Enter patient’s Initials. Use the first letter from the “first, middle, last (family)” names. If no middle initial, or it is unknown, enter first letter of “first, last” names. For example: o RAB, RB, R-B If the case includes a group of patients (e.g., literature article) and there are no initials, the identifier would be “Patient 1”, “Patient 2, or note a number of patients (e.g., patient 1 to patient 6). Gender Enter Patient’s gender – Male (M) or Female (F) or unknown (Unk) Date of Birth / Age at time of onset / Age Category Enter Patient’s date of birth. If not available, enter the age at the time of onset of the primary reaction. If none available, enter Patient’s Age Category. Height / Weight Age Group Category Definition (defined in completed days, months or years) Fetus During gestation, prior to birth Neonate 0 to <28 days Infant ≥ 28 days to <24 months Child ≥ 2 years to < 12 Adolescent ≥ 12 years to < 18 years Adult ≥ 18 years to < 65 years Elderly ≥ 65 years years Enter Patient’s height in cm / Enter Patient’s weight in kg Unsolicited Individual Safety Information (ISI) Report Form and Instructions QSD-001034 Version Number: 9.0 3/7 Section 3): Adverse Reaction Field: Diagnosis Instructions for completion: Enter the diagnosis as reported. Provide final reporter’s diagnosis rather than signs and symptoms whenever possible. If there is more than one (1) reaction, capture the most significant one in this field, and the additional reactions in the reaction description of the ISI form Date of Onset Enter the Date of Onset of the diagnosis. Reaction Description Provide a detailed chronological description of the reaction, including alternative etiology (including relevant medical history or concomitant diseases etc.), confounding factors, treatment of reaction, and outcome. Include relevant tests/ investigation results (specify test type and results with units), and applicable dates. Specify any abuse, lack of efficacy, medication error, misuse, occupational exposure, off label use or overdose. Clearly delineate follow-up / additional information from initial information when possible. Provide list of available information and attach if relevant. E.g., hospital notes, discharge summaries, etc. Unsolicited Individual Safety Information (ISI) Report Form and Instructions QSD-001034 Version Number: 9.0 4/7 Section 3): Adverse Reaction Field: Please check if the reaction led to one of the following Instructions for completion: Death should be indicated if the subject died at the time of, or at some time after the onset of this reaction. Please note that death is an outcome and not a reaction. Record the reaction that resulted in death Life Threatening is a reaction in which the subject was at immediate risk of death at the time of the reaction as it occurred; it does not refer to a reaction that hypothetically might have caused death if it was more severe Inpatient/Prolonged Hospitalization should be indicated if the reaction resulted in the subject formally being admitted to hospital as an in-patient or prolonged the stay of an existing hospitalization. An Emergency Room visit does not qualify Congenital Anomaly / Birth Defect should be indicated if the reaction is a congenital abnormality/birth defect Persistent or Significant Disability / Incapacity should be indicated if the reaction resulted in a substantial disruption of a person’s ability to conduct normal life and functions Suspected transmission of infectious agent is any suspected transmission of an infectious agent via a medicinal product (e.g., product contamination) Required Intervention to Prevent Permanent Impairment or Damage (Devices) should be indicated If you believe the intervention was necessary to preclude permanent impairment of a body function, or prevent permanent damage to a body structure, either situation suspected to be due to the use of a medical product Unsolicited Individual Safety Information (ISI) Report Form and Instructions QSD-001034 Version Number: 9.0 5/7 Section 4): Action Taken Field: Action taken Instructions for completion: Check what action was taken concerning the suspect product(s). None – no change in the regimen of the suspect drug. Discontinued – drug was discontinued Dose changed, specify the change. E.g., dose decreased, increased, frequency decreased… As applicable: Check Yes/No/Unk if reaction reoccurred after the drug was restarted. Check Yes/No/Unk if reaction abated after the suspect drug was stopped or dose was changed Check the tick box if corrective treatment was given. Specify all treatments given to treat the reported reaction. Note: If more then one suspect product, with different actions taken, detail in reaction description section. Section 5): Outcome of Reaction Field: Instructions for completion: Outcome of Reaction Check the outcome of the Main reaction at the time of this report. Check one: Recovered, Recovered with sequelae, (Specify sequelae), Recovering, Not (yet) recovered, Unknown, Fatal. (If the person died, specify the causes, circumstances and date of death) o Autopsy: Check Yes/No/Unk, if an autopsy was performed, attach report if available Date of Resolution or Duration Enter the Date of Resolution of the main reaction, if the reaction has resolved at the time of report completion. Enter duration if date of resolution is not available. Unsolicited Individual Safety Information (ISI) Report Form and Instructions QSD-001034 Version Number: 9.0 6/7 Section 6): Medications / Devices potentially causing the reaction Field Instructions for completion: Trade / Brand name & or INN (strength & form) Provide the local trade / brand name or International Nonproprietary Name (INN) of the suspect medication or device if available. Specify the strength and dosage form. Indication Provide the reason the drug / device was prescribed or taken by the patient (approved or unapproved indication) If the indication is unknown, indicate this. Dosage/ Unit / Frequency / Amount Enter the dosage, dosage unit and frequency. If different dosages and frequencies were used, use multiple lines or another page to enter the appropriate information with the most recent dosage and frequency first. If a Device, specify the amount used, or implanted if applicable. Route Enter the route of administration. If product was administered via an incorrect route, specify the actual route of administration. Treatment Dates Enter the start date of treatment. Enter the stop date of treatment, if applicable. If no start date or stop date, enter approximate duration of treatment. Lot/Batch No. Provide the lot/ batch number and expiration date if available. Company or NonCompany product Note if company (C) or non-company (NC) product Section 7): Other Medication or Device Field Other Medication / Device Instructions for completion: Other medications are those taken or administered within at least two weeks prior to the onset date of the primary clinical reaction. Exclude drugs used to treat the reaction. NOTE: See section 6) for instructions for similar fields. Case Submitted to any Regulatory Authority Check if submitted to any Regulatory Authority. Date / Signature Reporter’s signature Unsolicited Individual Safety Information (ISI) Report Form and Instructions QSD-001034 Version Number: 9.0 7/7