Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
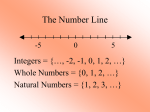
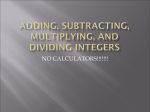
Post-processing subtraction image of T1-weighted from T2weighted image: evaluation of theoretical signal intensity and comparison with STIR image Poster No.: C-1925 Congress: ECR 2015 Type: Scientific Exhibit Authors: M. Nakadate, Y. Machida, Y. Iwasa, Y. Kitazume, U. Tateishi; Tokyo/JP Keywords: Edema, Imaging sequences, Comparative studies, MR, Image manipulation / Reconstruction, MR physics, Musculoskeletal soft tissue, Computer applications, Inflammation, Neoplasia DOI: 10.1594/ecr2015/C-1925 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 8 Aims and objectives Short TI inversion recovery (STIR) is an established sequence that suppresses short T1 tissue signals, such as those from fat, and can visualize inflammatory changes, edematous changes, and tumors with a better contrast [1-3]. However, STIR is not always performed during routine examinations because it requires additional imaging time. On the other hand, T1-weighted (T1W) and T2-weighted (T2W) images are obtained during nearly every examination. With the intention of decreasing the short T1 (fat) signal and accentuating the long T2 (edematous change) signal, similar to the process that occurs in creating a STIR image, we focused our attention on the post-processing subtraction of T1W images from T2W images. The purpose of this study was to evaluate the feasibility of using T2-T1 subtraction (T2T1sub) images, obtained by the post-processing subtraction of T1W images from T2W images, as an alternative to STIR images. Methods and materials A total of 38 consecutive MRI examinations of the extremities during which T1W, T2W, and STIR images had been obtained in the same plane were included in this retrospective study. All the examinations had been performed between January and March 2012. The MR images were obtained using a 1.5-T MRI system. The T1W, T2W, and STIR acquisition parameters were as follows: TR/TE, 360-700 msec/10-15 msec; NEX, 1; and matrix, 256 x 416 (for T1W); TR/TE, 3200-4100/105; NEX, 1; and matrix, 256 x 432 (for T2W); and TR/TE, 5300-6337/80; inversion time (TI), 130-150 msec; NEX, 1, and matrix, 224 x 304 (for STIR). For each examination, the T1W image was subtracted from the T2W image on a workstation to obtain a T2-T1sub image. The high-signal intensities on the T2-T1sub images were then compared with those on the STIR images as a standard reference. Continuous lesions were considered to be a single lesion, and the number of abnormal intensity areas was recorded. All the images were evaluated by a board-certified radiologist with no knowledge of any clinical information. The MR image evaluation and clinical diagnosis were also investigated using the medical records (Table1). Table 1. Patient backgrounds and MR image evaluations Page 2 of 8 Disease number Myositis, Fasciitis 15 Tumor 5 Cystic lesion 3 No abnormal finding 15 In addition, a theoretical spin echo signal intensity contour map of the T2-T1sub image was created and compared with that of the STIR image. The signal intensity equation and protocol for drawing the contour maps were based on previously reported methods [1; 4]. The contour maps for each sequence were created using the spin-echo signal intensity equation for the T1W (TR/TE, 550/10), T2W (TR/TE, 3500/80), and STIR sequence (TR/ TE/TI, 6100/80/150). Results Seventy-six abnormal signal intensity areas were found on the STIR images, and 74 of them were detected on the T2-T1sub images (Table2 and Figures 1-3). Four lesions were identified as false-positive results. The sensitivity and positive predictive values of the T2-T1sub images were 97.4% and 94.9%, respectively. A comparison of Figure 4C and 4D showed that the signal intensity distribution in the T2-T1sub image was similar to that in the STIR image within the physiological T1/T2 range. Table 2. Abnormal intensity areas detected on STIR images Disease Number of abnormal intensity areas Myositis 33 Fasciitis 4 Subcutaneous edema 19 Tumor 17 Cystic lesion 3 Images for this section: Page 3 of 8 Fig. 1: A 74-year-old male with myositis. (A) A T2-T1 subtraction image and (B) a STIR image of the left shoulder and upper extremity show almost the same distribution of high signal intensity areas. Note that the T2-T1 subtraction image contains respiratory motion artifacts. Fig. 2: A 63-year-old male with necrotizing fasciitis of the right thigh. (A) The T2-T1 subtraction image shows an excellent concordance with (B) the STIR image. Page 4 of 8 Fig. 3: A 76-year-old male with a pleomorphic sarcoma in the right thigh. (A) The T2T1 subtraction image shows a marked similarity to (B) the STIR image in terms of tumor characterization, subcutaneous edema, and muscular edematous change. Page 5 of 8 Fig. 4: Examples of the signal intensity contour maps of (A) T1-weighted, (B) T2weighted, (C) T2-T1 subtraction, and (D) STIR sequences plotted on a T1 (horizontal axis) and a T2 (vertical axis) plane. The signal intensity contour map of the T2-T1 subtraction shows a strong agreement with that for the STIR. These contour maps were created using the spin-echo signal intensity equation for the T1-weighted (TR/ TE, 550/10 msec), T2-weighted (TR/TE, 3500/80 msec), and STIR sequence (TR/TE/TI, 6100/80/150 msec). Page 6 of 8 Conclusion The subtraction technique is used in daily clinical practice, such as for the subtraction of pre-contrast from post-contrast enhancement images or out-of-phase from in-phase T1W images. However, subtraction between different sequences is not common. As far as we know, only Bonett et al. [5] has previously reported the usefulness of T2-T1sub images for obtaining evidence of epidural cerebrospinal fluid leakage in cases of spontaneous intracranial hypotension, but they did not evaluate or discuss the actual creation of such images. We observed that T2-T1sub images created in this manner are very similar to STIR images, as shown using clinical images and signal intensity contour maps. False-positive regions were mostly generated by subtraction artifacts, such as position gaps between the T1W and T2W images or magnetic field inhomogeneity. These motion artifacts could be identified as false-positive regions by referring to the original T1W and T2W images. In addition, the signal-to-noise ratio were considered to be better for T2-T1sub images than for STIR images, especially when the subtraction image was generated without a position gap, but this hypothesis could not be proven in the present study. Furthermore, because of the use of basic imaging sequences, the same post-processing subtraction technique can likely be also applied to the head and neck, spine, or pelvic regions. The relative nature of MRI signal intensity could lead to the following study limitations. First, when the receiver gain is different between T1W and T2W image, simple subtraction becomes meaningless and correct weighting is necessary. Second, because these results were obtained using a small sample size and a single MR machine, confirmation using a wide variety of MR machines and institutions is needed to generalize the present findings. In addition, for the widespread using of this subtraction method, the development of useful software capable of creating subtraction images on the PACS viewer or MR console system in a simple and user-friendly manner is essential. In conclusion, the current study has shown that subtraction images obtained by the postprocessing of T1W and T2W images could be a useful alternative to STIR images. Personal information Masashi Nakadate, M.D., Ph.D. Page 7 of 8 Department of Diagnostic Radiology, Medical Hospital, Tokyo Medical and Dental University, Tokyo, Japan; [email protected] Youichi Machida, M.D., Ph.D. Department of Radiology, Kameda Kyobashi Clinic, Tokyo, Japan. Yoshihiro Iwasa, M.D. Department of Diagnostic Radiology, Medical Hospital, Tokyo Medical and Dental University, Tokyo, Japan. Yoshio Kitazume, M.D., Ph.D. Department of Diagnostic Radiology, Medical Hospital, Tokyo Medical and Dental University, Tokyo, Japan. Ukihide Tateishi, M.D., Ph.D. Department of Diagnostic Radiology, Medical Hospital, Tokyo Medical and Dental University, Tokyo, Japan. References 1. 2. 3. 4. 5. Dwyer AJ, Frank JA, Sank VJ, Reinig JW, Hickey AM, Doppman JL (1988) Short-Ti inversion-recovery pulse sequence: analysis and initial experience in cancer imaging. Radiology 168:827-836 Fleckenstein JL, Archer BT, Barker BA, Vaughan JT, Parkey RW, Peshock RM (1991) Fast short-tau inversion-recovery MR imaging. Radiology 179:499-504 Pitt AM, Fleckenstein JL, Greenlee RG, Jr., Burns DK, Bryan WW, Haller R (1993) MRI-guided biopsy in inflammatory myopathy: initial results. Magn Reson Imaging 11:1093-1099 Tamura H, Nagasaka T (2010) A tool to aid optimization of imaging parameters in clinical MRI. Bulletin of School of Health Sciences Tohoku University 19:117-123 Bonetto N, Manara R, Citton V, Cagnin A (2011) Spinal subtraction MRI for diagnosis of epidural leakage in SIH. Neurology 77:1873-1876 Page 8 of 8