Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
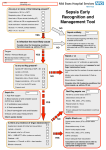
MedEd Portal/ POGOe Human Patient Simulation Title: Altered Mental Status Target Audience: Resident Learning Objectives: - Primary – Recognize a septic patient – Identify etiology of sepsis Urosepsis and Sacral Decubitus Ulcer – Appropriate Management of Sepsis - Secondary – Aggressive resuscitation – Transfuse Packed Red Blood Cells (PRBC) – Central Venous Pressure (CVP) by ultrasound or by monitor via central line – Vasopressors – Identify Do Not Intubate (DNI) status and do not intubate the patient - Critical Actions Checklist 2 large bore intravenous access (IV) Oxygen Monitor Blood and Urine Cultures Appropriate Labs Chest X-ray (CXR) Identify Pyelonephritis Identify Infected Sacral Decubitus Ulcer Antibiotics PRBCs transfusion Vasopressors Patient is a DNI - Do not intubate patient Intensive Care Unit (ICU) consultation Surgery Consultation Environment: - Environment – Rural Emergency Department Manikin Set Up – Elderly female - Props – – – – Sacral decubitus ulcer moulage, Foley catheter containing cloudy yellow fluid Electrocardiogram (EKG) CXR Actors: (All roles may be played by residents participating) - Resident Physician - 2 Nurses - Intern - Family Member Case Narrative: - Chief Complaint – Altered Mental Status - History – Patient is an 82 year old female who presents from a nursing home via EMS for evaluation of altered mental status and fever. Per paramedics, the nursing home staff noted a fever of 102.2 and the patient has not been as alert as she was 2 days ago. She has been a resident there for two months while trying to rehabilitate from a hip fracture. - Additional history given only if nursing home or husband is called – Nurse states she usually takes care of the patient during the week and last Friday she was doing well, but something happened over the weekend. – She still is not getting out of bed. – She had a foley catheter placed recently. – Her Primary Medical Doctor (PMD) is treating her with amoxicillin. – The patient has a son, but he only has been to the nursing home once or twice to see his mother. – Patient resuscitation status is DNI. The only way to obtain this information is to contact her husband listed on the nursing home demographic sheet or the nursing home personal. The DNR/ DNI sheet did not arrive with the patient. - Past Medical History – Hypertension (HTN) – Urinary Tract Infection (UTI) – Dementia – Hyperlipidemia (HLP) - Social History – Pt used to live at home with her husband. He was her primary caretaker until she fell and suffered a hip fracture. – No alcohol, tobacco, or drug use - Medications – Amoxicillin for UTI over the past few days – Namenda, Lipitor, Hydrochlorothiazide, Atenolol, Lantus, Lovenox - Surgical History – Hip fracture 2 months ago status-post arthroplasty – Hysterectomy - Allergies – No known drug allergies (NKDA) - Review of Systems – Deconditioning, decreasing appetite, fevers – No shortness of breath, no cough – No chest pain or palpitations – No vomiting, no dysphagia, no abdominal pain, no bloody stools – No focal weakness or numbness, no headache – Intermittent delirium for the past 48 hours – No lower extremity edema – Mild diaphoresis, no rashes or lesions - Physical Exam – Heart Rate (HR) 123, Blood Pressure (BP) 82/45, Respiratory Rate (RR) 31, O2 – 95% on room air, Temperature 39.1 – Accucheck – 52 (only if asked for) – General – Lethargic, moaning, Glasgow Coma Scale – 11 (eyes 3, Verbal 4, Movement 4) – Head, Eyes, Ears, Nose Throat (HEENT) – dry mucous membranes, no meningismus, pupils equally reactive and responsive to light and accommodation (PERRLA) – Cardiovascular (CVS) – tachycardic, regular rhythm and rate , no murmurs, rubs, or gallops, no palpable distal pulses, but palpable femoral and carotid – Respiratory – tachypnea, clear to auscultation bilaterally with no wheezes, rales, or rhonchi – – – – – - Abdominal – wincing and increased moaning with suprapubic palpation, no rebound or guarding, rectal heme-occult negative Genitourinary – foley catheter in place with cloudy urine Extremities – no edema, no rashes Skin – tinting, no cyanosis Only if asked for Large 10 cm sacral decubitus ulcer stage 4 with surrounding erythema, yellowish-green base, and foul sweet smell. Scenario Branch Points – The resident participant must identify the septic patient. This will be evident through her general appearance, physical exam, and vital signs. – The etiology of her sepsis is obtained not only by labs (UTI / pyelonephritis), but also by a thorough physical exam. Only if she is rolled with they identify the infected decubitus ulcer, suspicious for pseudomonas. – Aggressive resuscitation should be initiated with IVF, antibiotics, and vasopressors. – Fluid resuscitation can be guided by a CVP through a central venous line or by evaluating IVC compression with an ultrasound. – Antibiotic coverage must be tailored to include methicillin resistant Staphylococcus aureus, Pseudomonas, and urinary flora. – The patient will require at least 4 liters of fluid resuscitation, 2 units of PRBCs, and vasopressors before vital signs, urinary output, or perfusion will improve. – The patient will appear to need mechanical ventilation, but this should not be done. The resident needs to obtain the patient’s code status, and this can only be done by contacting her husband or nursing home. – If the patient is intubated, her husband will spontaneously arrive in the Emergency Department requesting she be taken off the ventilator. – The resident should consult both the Medical Intensivist and Surgeon for evaluation and admission. Instructors Notes: - Tips to Keep the Scenario Flowing – The director should give the paramedic report – The director should answer questions as if they were the patient – Make the patient be very vague, altered and toxic appearing – Do not give tips regarding the presence of a sacral decubitus ulcer. – – – – - Tips to Direct Actors – – - Nurses will be new grads and unfamiliar with management of sepsis. They will need specific drug dosages and instructions for what type of IV access, lines, etc… The Patient’s Husband - You will be very distinct regarding the patient’s DNI status if contacted over the phone. If not contacted and the patient is intubated, you should let your disappointment be known once you arrive to the Emergency Department. Request that your mother’s breathing tube be removed. Scenario Steps – – - The patient must not improve unless the appropriate amounts of fluids are given. The patient’s appearance, vitals and perfusion will not improve with only 1-2 liters of IVF and vasopressors. Allow the resident to intubate the patient if they so choose. If intubated, the patient’s husband will arrive in the ED with disapproval of the decision to intubate and request she be taken off the ventilator. Optimal Management Path Identify sepsis and likely etiology (UTI, pyelonephritis, infected sacral decubitus ulcer) IVF Resuscitation guided by CVP (via central venous line or IVC using U/S) Blood and Urine Cultures Tailored Antibiotics Contacting Family Respecting patient’s DNI status Potential Errors Path Not recognizing sepsis Not obtaining cultures Not rolling the patient and identifying the sacral decubitus ulcer likely infected with pseudomonas Under resuscitation with not enough IVF Starting vasopressors without completely resuscitating the patient with IVF beforehand Not contacting family members Intubating the patient Imaging and Labs – CBC – WBC 18, Hgb 7, Hct 26, Plt 180 – – – – Debriefing Plan: - Topics to discuss – Identifying the signs and symptoms of Systemic Inflammatory Response Syndrome and Sepsis – The importance of physical exam – Correct Management of Sepsis – Management of DNR/DNI patient’s and how to update a patient’s DNR/DNI status in the Emergent Department – Communication challenges during transitions of care for the elderly (aka need to call the nursing home) Pilot Testing and Revision: - Chem 7 – Na 148, K 4.9, Cl 111, CO2 13, BUN 64, Cr 1.9, Glu 180 Lactate – 7.2 U/A – WBC >182, Many Bacteria, + LE, + Nitrates ABG 7.21 / 29 / 158 / 14 / 95% / - 11 Number of Participants – 4 Anticipated Management Mistakes – Under resuscitation – No antibiotics or not treating pseudomonas – Intubation Evaluation form for participants – generic handout Authors: - John B. Seymour, MD. University of North Carolina Department of Emergency Medicine. Rochelle Chijioke, MD. University of North Carolina Department of Emergency Medicine. Amar Patel, MS. Director of the Center for Innovative Learning at WakeMed Health & Hospitals. Graham Snyder, MD. Assistant Professor and Medical Director of the Center for Innovative Learning at WakeMed Health & Hospitals Kevin Biese. MD, MAT. University of North Carolina Department of Emergency Medicine, Assistant Professor and Residency Director Jan Busby-Whitehead, MD. University of North Carolina Professor & Chief, Division of Geriatric Medicine; Director, Center for Aging and Health.