Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
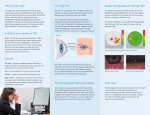
Comparative Investigation of Treatments for Evaporative Dry Eye Introduction The lipid layer of the tear film is the most important evaporation protection for tear fluid and can cause a 90 - 95% reduction in evaporation [24]. Evaporative dry eye is caused by impairments of the lipid layer and is the most commonly encountered category tear film dysfunction in medical practice. The international literature consistently reports on the conspicuously high incidence of hyperevaporative dry eye [12, 16, 23, 34, 39]: Impairments of the lipid layer and/or meibomian glandular dysfunction were diagnosed by Shimazaki et al. in 75% [34] and by Heiligenhaus et al. in 78% [12] of dry eye patients. Horwath-Winter et al. even observed this functional disorder in 87% of patients with reduced tear film break-up time [16]. Whereas under normal conditions about 40% of tear fluid is lost by evaporation, this level can increase up to 100% in persons with meibomian glandular dysfunction [23]. Hyaluronic acid (sodium hyalonurate) based artificial tear formulations have long been part of substitution therapy for dry eye disease and are primarily used to treat tear fluid deficiency [20]. The use of hyalonurate artificial tear formulations specifically for the evaporative form of dry eye does not satisfy the criteria of evidencebased medicine. So far only a single study in the literature has addressed this issue. However, this study with only 10 patients and a follow-up period of no more than 90 minutes [32] cannot be considered an adequate basis for a therapy recommendation. To stabilise the lipid layer of the tear film, a phospholipid-liposome based eye spray is available which is applied to the closed eyelids. Dausch et al. were the first to evaluate in detail the phospholipidliposome therapeutic concept developed in Germany and to assemble material describing its scientific principles [22]. The phospholipid-liposome eye spray is now an established component of sicca therapy [5, 19, 41] and is recommended as the first-line therapy for shortened tear film break-up time [3]. Because of the aforementioned inadequate database relating to the benefits of hyalonurate artificial tears in evaporative dry eye, we have conducted this study to compare the two substitution therapy options so that future therapy recommendations can be based on proven efficacy. Methods 216 patients suffering from evaporative dry eye were included in this prospective, randomised trial at the two participating centres. The first subsample consisted of 173 patients, who were examined at the ophthalmological clinic of the first author. The second subsample comprised 43 patients who were examined at the ophthalmological clinic of the second-named author. 167 of the enrolled patients were female and 49 male. The two sexes were equally represented in terms of age structure (χ2 value = 2.946; df =3; p = 0.400). 9 patients (4.2%) were under 25 years old, 26 (12.0%) in the 25 to 45 year age group and 42 patients (19.4%) were between 45 and 60 years old. The great majority of patients (139) with a proportion of 64.4% were in the over 60 years age group. Altogether 17 patients (7.9%) were contact lens wearers. 19.4% had been suffering for less than a year from dry eye symptoms, 46.5% had already had the symptoms for one to five years. A further 23.9% of the patients had been suffering from the symptoms for 5 to 10 years and 10.3% already for longer than 10 years. The patients were assigned by randomisation to the two treatment groups. The patients of Group A (n= 113) were treated throughout the study with the phospholipid-liposome eye spray (Tears Again, Optima Pharmazeutische GmbH) and the patients of Group B (n= 103) with hyalonurate artificial tears (Vismed light, TRB Chemedica AG). The patients were instructed to use their assigned product as recommended by the manufacturer in the Patient Information Leaflet, but at least three times daily. The evaporative form of dry eye was diagnosed on the basis of the shortened tear film break-up time and the findings of the slit lamp examination of the lids, and especially the signs of chronic blepharitis [9, 12, 13]. The examinations performed before the start of treatment, after 4 and after 12 weeks included grading of the LIPCOF (lid-parallel conjunctival folds), measurement of the NIBUT (non-invasive break-up time), the Schirmer I test as well as a slit lamp examination of the lid margins, in which the degree of the lid margin inflammations was rated between grade 0 (no inflammation) and grade 3 (pronounced inflammation). The LIPCOFs were graded according to the classification of Höh et al. [14]. The subjective assessment of the tolerability and therapeutic efficacy of each product was recorded using a questionnaire to be completed by the patients independently. The assessment was based on the German sixpoint school grading system extending from grade 1 (excellent) to grade 6 (unsatisfactory). The statistical analysis was performed using the SPSS v.17.0 statistical program. Before using a statistical procedure, the preconditions for its use were verified (e.g. the normal distribution of the variables). If the preconditions were largely fulfilled or the robustness of a procedure was demonstrated, parametric methods were used for the evaluation. If the preconditions were not fulfilled, a non-parametric method was selected (see [42]). Taking into account the longitudinal data structure, for example, repeated measures analyses of variance (ANOVAs) were performed in which the treatment group assignment was usually modelled as a betweensubjects factor and the time course as a repeated measures factor. To test different group developments, i.e. improvements in the groups differing over the treatment period, interaction effects were included in the model. The significance of an interaction effect then means that during the course of treatment the groups have experienced substantially different improvements in the measure analysed (see also [42]). If, for example, one product acts more rapidly or potently than another, then this is expressed as a significant interaction effect. The study was designed and conducted in conformity with the applicable regulations of the medical professional code and the Declaration of Helsinki. Results Degree of inflammation of lid margins ● Fig. 1 shows the development during the follow-up period: as regards the degree of lid margin inflammation, there were no differences between the two groups at the start of the study (T= - 0.789; df =211; p>0.431, not significant). An average patient had a degree of inflammation of about 1.6 at the first examination (eye spray group: 1.528; artificial tears group: 1.635). Four weeks after the start of treatment, substantial improvements in the degree of inflammation were observed in both groups (time: F(2.404) = 49.432; p <0.001). The mean improvement, however, was greater in the eye spray group (interaction effect: F(2.404) = 6.590; p = 0.002). While the artificial tears group then showed a mean degree of inflammation of 1.417 (SE = 0.072), the mean degree of inflammation in the eye spray group was 1.056 (SE= 0.068). The eye spray group therefore experienced a threefold greater decrease in the inflammation. Twelve weeks after the start of the study, the mean degree of inflammation was 1.313 (SE = 0.076) in the artificial tears group and 0.833 (SE = 0.072) in the eye spray group. Over the total course, therefore, an average eye spray-using patient improved by a mean 0.695 degrees of inflammation, while the overall improvement in the eye drops group 0.322 was degrees of inflammation. Tear film break-up time(NIBUT) As can be seen from ● Fig. 2, the two treatment groups had the same tear film break-up times at the start of the study (the confidence intervals of the means overlap). As an overall average, tear film break-up time was about 6.87 seconds. Although an improvement in the tear film break-up times occurred in both groups over the total course (factor time: F(2.318) = 29.198; p <0.001), greater improvements were already detectable in the eye spray group after 4 weeks (T= 1.892; df = 162; p = 0.060). The eye spray group improved by a mean 1.413 seconds (20.6%) and the artificial tears group by only 0.253 seconds (3.7%). After altogether 12 weeks, a mean improvement of 3.034 seconds (44.2%) was demonstrated for the eye spray group, while the mean improvement over the total period for the artificial tears group was 1.362 seconds (19.8%). Over the total course, therefore, there was a highly significant difference between the two groups (interaction effect: F(2.318) = 5.968; p = 0.003). The improvement in the tear film break-up times was more than twice as high in the eye spray group than in the artificial tears group. Towards the end of the study, the patients of the eye spray group showed mean tear film break-up times of 9.974 seconds and the patients of the artificial tears group showed tear film break-up times of 8.157 seconds, i.e. a difference of almost 2 seconds. Grade of LIPCOF (lid-parallel conjunctival folds) As shown in ● Fig. 3, the two treatment groups differed substantially at the start of the study as regards their LIPCOF values (T = –2.811; df = 214; p = 0.004). Group B (artificial tears) showed a mean LIPCOF grade of about 3.1 (SE=0.116), while Group A (eye spray) showed a lower LIPCOF grade of about 2.7 (SE = 0.108). Taking into account this à priori difference, after 12 weeks a substantial improvement in the LIPCOF grade was found in both groups (time: F(1.202) = 104.171; p<0.001), but a greater improvement was observed in the eye spray group (interaction effect: F(1.202) = 5.428; p <0.021). For example, the mean LIPCOF grade in the eye spray group improved by more than 28.5%, i.e. 0.771 LIPCOF grades, while the mean LIPCOF grade in the artificial tears group improved by less than 16% (namely by 0.484 LIPCOF grades). Schirmer I test At the start of the study there were no differences between the two treatment groups as regards their tear secretion quantity (T = 0.844; df = 214; p = 0.400; not significant). The mean tear secretion quantity was 12.952 mm (SE= 0.724) in five minutes in the eye spray group and 12.042 mm (SE = 0.761) in five minutes in the artificial tears group. During the further course of the study, neither group-independent, i.e. time-related improvements (factor time: F(2.396) = 0.481; p = 0.619; not significant) nor group-related (condition: F(1.198) = 0.911; p = 0.341; not significant) differences were observed. Neither of the products showed an advantage over the other (interaction effect: F(2.396) = 0.085; p = 0.918; not significant). At no point in time did the mean secretion quantities differ. This applies both within the groups across the three time points and between the groups at every time point. Assessment of tolerability During the course of the investigations, the patients were asked to give an assessment of the tolerability of the product they had used by assigning school grades. ● Fig. 4a and b show the grades assigned in the two treatment groups. While the eye spray group assigned a mean tolerability grade of 1.7 (“2+”), the artificial tears group assigned a mean grade of 2.6 (“3+”). This therefore represented a descriptive difference of almost one grade, which could also be demonstrated by using an inferential statistical method (Mann-Whitney U test: rank [eye spray] = 80.71; rank [artificial tears] = 133.59; U value = 2679.5; p <0.001). The eye spray was rated as significantly better tolerated than the artificial tears eye drops. Assessment of efficacy and duration of action Requested to assess the efficacy of the product, the patients of the eye spray group gave a similarly positive judgement as the patients of the artificial tears group (● Fig. 5a, b). While the patients of the eye spray group gave an average grade of “good” (2.07) for efficacy, the patients of the artificial tears group rated the efficacy of the product they used as “satisfactory“ (3.0). The observed difference of about one school grade was significant (Mann-Whitney U test: rank [eye spray] = 81.21; rank [eye drops]=127.74; U value=2857.0; p<0.001). The efficacy of the eye spray was rated about one grade higher. Asked to state how long the effect of the product had persisted, the patients of the eye spray group responded with a mean 4.53 hours (SD = 1.519). The patients of the artificial tears group reported on average an action persisting for 4.00 hours (SD=1.590). This difference of half an hour was significant in the inferential statistical analysis 2.386; df = 193; p = 0.018). Discussion In addition to tear film stability, tear hyperosmolarity is now regarded as the central mechanism in the development of superficial inflammations, surface lesions and sicca symptoms. [23]. Hyperosmolarity develops as a result of increased evaporation of water from the ocular surface [28]. Clinical excessive evaporative loss is caused especially by meibomian glandular dysfunction (MGD) which leads to an unstable tear film lipid layer and is termed the evaporative form of dry eye. Tear hyperosmolarity causes damage to the surface epithelium by activating a chain of inflammatory events on the ocular surface and release of inflammatory mediators into the tears. The epithelial damage includes cell death by apoptosis, goblet cell depletion and an impairment of mucine expression which leads to instability of the tear film. This instability increases the hyperosmolarity of the ocular surface and thereby contributes to aggravating the condition. The instability of the tear film can also be induced by various etiologies without the prior onset of tear hyperosmolarity. It is now assumed that the two main categories of dry eye, namely the form caused by tear fluid deficiency (aqueous tear deficient dry eye) and the evaporative form (evaporative dry eye) can each develop into a combined form due to interactions occurring over time and can increase the severity of dry eye [10]. The pathophysiological mechanism described here can only be controlled therapeutically by normalising the tear film instability manifesting as early tear film break-up and preventing excessive evaporative loss of tear fluid. While a broad consensus exists regarding the fundamental benefits of hyalonurate artificial tears [1, 2, 18, 40], controversy continues regarding the degree of benefit compared to differently based wetting agents: Johnsen et al. report minor advantages [17]. Nepp et al. in a double-blind study were unable to determine either subjectively or objectively significant differences between treatment with hyalonurate artificial tears and a saline solution [29]. Other authors have even reported on the superiority of other products [26, 30, 33]. Holly, on the other hand, disputes the need for gel-type or high viscosity artificial tears with the noteworthy statement that the extremely thin tear film is controlled solely by surface forces and that its resistance to gravity-induced drainage is due only to the surface forces prevailing in the tear film [15]. The use of hyalonurate artificial tear formulations can in principle provide an increase in the tear film break-up time in the evaporative form of dry eye [32]. On the other hand, the use of eye drops and gels is known to cause an additional increase in evaporation [25]. Firstly, instillation impairs the lipid layer of the tear film [11] and secondly, the natural balance of the various tear film components is considerably affected, since instillation increases the quantity of fluid on the ocular surface seven-fold compared to the normal tear film [9]. The use of artificial tears, therefore, runs counter to an important therapeutic objective, namely to normalise the excessive evaporation. Heiligenhaus et al. critically evaluated the benefits of stand-alone therapy with artificial tears in lipid phase disorders years ago and restricted the indication for artificial tears stand-alone therapy to the rarely occurring isolated and slight impairment of the aqueous layer [13]. Just under 60% of the patients applied the ophthalmological preparations eight times daily [12]. Depending on the severity, hourly to half-hourly administration of artificial tear formulations is generally recommended [21]; with an average sleep duration of 8 hours, this represents a frequency of 16 and 32 applications daily. Bernauer et al. even report excessive drop application frequencies of up to 100 applications daily [4]. Although this author’s case reports are by no means restricted to average sicca patients, the report nevertheless clearly demonstrates the therapeutic limitations of hyalonurate artificial tear formulations. Although these products can provide temporary moistening of the ocular surface, the desired stabilisation or normalisation of the natural tear film and its properties are not achieved. Against this background it appears advisable to intervene as little as possible in the sensitive natural system of the tear film and to maintain the balance between the various endogenous tear film components. The therapeutic goal should therefore be to stabilise the lipid layer, firstly to preserve the tear film stability and secondly to prevent excessive evaporation, whereby tear hyperosmolarity can also be prevented. Craig et al. have demonstrated a significant increase in the thickness of the lipid layer and the stability of the tear film after using the liposomal eye spray [8]. Moreover, treatment with the phospholipid-liposome spray offers significant clinical advantages compared to the use of lipid-containing artificial tear formulations, especially as regards increasing the film break-up time [9]. Phospholipids are an important component of the polar lipids of the endogenous meibomian secretion [38]. The surface active phospholipid molecules carry the hydrophobic, unpolar portion of the lipid layer on the aqueous layer and are what enable its distribution [6]. Impairments of the lipid layer and the resulting hyperevaporative dry eye are attributed to a deficiency of phospholipids [35, 36], especially in association with chronic blepharitis [27, 37]. Phospholipids increase the stability of the tear film and cause a marked increase in the tear film break-up time [31]. In the present study we were able to demonstrate the superiority of treatment with the phospholipid-liposome eye spray in the treatment of evaporative dry eye. Especially the highly significant difference in the improvement in the tear film break-up time proves that the phospholipidliposome eye spray is suitable for treating tear film instability as one of the central aspects involved in tear film dysfunction. It is very probable that the normalisation of the tear film stability which was achieved had also returned the excessive evaporation to normal levels and thereby also counteracted the tear hyperosmolarity, with the result that in the long term the entire natural tear film system can regenerate. The severity of dry eye is greatest, however, when evaporative dry eye and aqueous tear deficiency coincide, especially in Sjögren’s syndrome [7]. The therapeutic strategies developed to date have generally proved unsatisfactory. A therapeutic combination consisting of the phospholipid-liposome eye spray and an artificial tear formulation could result in a considerable improvement in findings in the substitution therapy of severe forms of dry eye and therefore define a therapeutic “gold standard”. In combined tear film dysfunction, combined therapy appears both appropriate and logical. To what extent a therapeutic combination of this kind does in fact offer advantages compared to conventional therapeutic strategies remain to be investigated in further randomised studies. Mean change in degree of lid margin inflammation during the course of treatment Entzündungsgrad: Degree of inflammation Tests der Effekte: Tests of effects Bedingung: Condition Bedingung*Zeit: Condition*time Augenspray: Eye spray Augentropfen: Eye drops Erstuntersuchung: First examination nach 4 Wochen: after 4 weeks nach 12 Wochen: after 12 weeks Fig. 1 Degree of inflammation of the lid margins during the course of therapy (first examination, after 4 and after 12 weeks); the standard errors of the means are shown as vertical bars. Mean change in tear film break-up time (NIBUT) during the course of treatment Tränenfilaufreißzeit: Tear film break-up time Tests der Effekte: Tests of effects Bedingung: Condition Bedingung*Zeit: Condition*time Augenspray: Eye spray Augentropfen: Eye drops Erstuntersuchung: First examination nach 4 Wochen: after 4 weeks nach 12 Wochen: after 12 weeks Fig. 2 Tear film break-up time (NIBUT) during the course of therapy (first examination, after 4 and after 12 weeks); the standard errors of the means are shown as vertical bars. Mean change in mean lid-parallel conjunctival folds (LIPCOF) grade during the course of treatment LIPCOF Faltengrad: LIPCOF grade Tests der Effekte: Tests of effects Bedingung: Condition Bedingung*Zeit: Condition*time Augenspray: Eye spray Augentropfen: Eye drops Erstuntersuchung: First examination nach 12 Wochen: after 12 weeks Fig. 3 LIPCOF values at the start of the study and after twelve weeks (the vertical bars are the standard errors of the means). Tolerability - eye spray Häufigkeit: Frequency Wie beurteilen Sie die Verträglichkeit des Präparats? (in Schulnoten): How do you rate the tolerability of the product? (in school grades) Mittelwert: Mean value Std.-Abw.: SD Tolerability - eye drops Häufigkeit: Frequency Wie beurteilen Sie die Verträglichkeit des Präparats? (in Schulnoten): How do you rate the tolerability of the product? (in school grades) Mittelwert: Mean value Std.-Abw.: SD Fig. 4 a Tolerability ratings of the eye spray by the patient. b Tolerability ratings of the eye drops by the patient. (Rated as school grades: 1 = excellent; 2 = good; 3 = satisfactory; 4 = adequate; 5 = poor; 6 = unsatisfactory). Efficacy - eye spray Häufigkeit: Frequency Wie beurteilen Sie die Wirkung des Präparats? (in Schulnoten): How do you rate the efficacy of the product? (in school grades) Mittelwert: Mean value Std.-Abw.: SD Efficacy - eye drops Häufigkeit: Frequency Wie beurteilen Sie die Wirkung des Präparats? (in Schulnoten): How do you rate the efficacy of the product? (in school grades) Mittelwert: Mean value Std.-Abw.: SD Fig. 5 a Efficacy ratings of the eye spray by the patients. b Efficacy ratings of the artificial tears eye drops by the patients. (Rated in school grades: 1 = excellent; 2 = good; 3 = satisfactory; 4 = adequate; 5 = poor; 6 = unsatisfactory). Conflict of interest: no References