Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
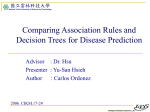
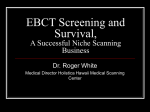
Coronary artery dosimetry for adjuvant left-sided breast radiotherapy: changes in reported dosimetry when the left anterior descending artery (LAD) contour is shifted from it`s true position Poster No.: R-0121 Congress: 2014 CSM Type: Scientific Exhibit Authors: S. Sampaio, P. Graham; KOGARAH/AU Keywords: Breast, Cardiac, CT, Radiation therapy / Oncology, Dosimetric comparison DOI: 10.1594/ranzcr2014/R-0121 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply RANZCR/AIR/ACPSEM's endorsement, sponsorship or recommendation of the third party, information, product or service. RANZCR/AIR/ ACPSEM is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold RANZCR/AIR/ACPSEM harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, .ppt slideshows, .doc documents and any other multimedia files are not available in the pdf version of presentations. Page 1 of 13 Aim Little strong dose-volume dependence data exists for cardiac structures. Undoubtedly radiation dose to the heart results in an increased risk of late cardiac complications and 4 3 6 5 cardiac mortality . The LAD (left anterior descending artery) is at particular risk, given its anterior position on the heart and resultant exposure to high doses of radiation 2 in left-sided tangential radiotherapy . The inferior LAD typically receives higher doses compared to the superior LAD which is anatomically more posteriorly located. The LAD itself can be difficult to contour. In particular, the inferior LAD which is most susceptible to high dose is often poorly defined on planning CT. Feng et al. demonstrated marked variations in coronary artery contouring between radiation oncologists. Whilst that study showed improvement in reported dosimetry with better concordance of target delineation, it did not specifically examine the extent to which a structure such as the LAD can be 'misplaced ' before one sees a significant difference in reported dose. The lack of strong dose-volume response data for coronary arteries is an added barrier to the adoption of routine coronary artery contouring into practice. The Danish Breast Cancer Cooperative Group recommend that the volume of whole heart receiving >40Gy be kept below 5% (www.dbcg.dk) but do not specify limitations for the coronary arteries. Other studies have limited any part of the arch of the LAD to receiving less than 20Gy and 10% of the whole LAD to receiving less than 20Gy but there is little evidence to justify 1 these limitations . By simulating the potential shifts in coronary artery contours that can arise through errors in contouring, we hope to determine to what extent a coronary artery (in this study the LAD) and its subdivisions can be misplaced (and in which direction- medial, lateral, superior and inferior) before one sees a significant change in reported dose. Methods and materials Case selection 70 patients with left-sided breast or chest wall radiotherapy were treated on the STARS Trial (STARS, STudy of Anastrozole and Radiotherapy Sequencing, TROG 08.06) at St George Hospital between September 2009 and March 2012. Of these, 10 patients were Page 2 of 13 selected: 3 with low LAD mean doses (below 10Gy), 4 with medium LAD mean doses (10-20Gy) and 3 with high LAD mean doses (>20Gy). Target Contouring All patients had pre-existing LAD, superior and inferior LAD contours mandated by the STARS trial protocol and these volumes underwent regular auditing. The LAD contour was 3mm in diameter and included the short segment of the left coronary artery before it bifurcates. The superior LAD incorporated the proximal half of the LAD, and inferior LAD, the distal half . Because the surface of the heart is curved, expansions of 5, 10 and 15mm were created around the existing 3mm diameter vessel contour (Figure 1.). Identical vessel contours were then positioned 5, 10 and 15 mm medial and lateral to the existing LAD contour (Figure 2. and 3.). As CT slices were 2mm thick, superior and inferior 'shifts' were in 6, 12 and 18mm increments. Dosimetry For the purpose of this study all dosimetry was calculated without a boost and with a prescribed total dose of 50Gy in 25 fractions. Statistical Methods Mean, maximum doses and V20 (volume receiving 20Gy) figures have been described. An absolute difference in recorded mean dose of 10Gy was considered to be clinically significant. Although there is little data to support its use, a change in whole LAD mean dose from below to above 20Gy (and vice versa) has been reported. As limiting V20 for the whole LAD to <10% has been used in previous studies, changes in V20 from below to above 10% (and vice versa) have also been reported. Images for this section: Page 3 of 13 Fig. 1: Expansions around LAD (5,10,15mm) Page 4 of 13 Fig. 2: Medial Contour Shifts Page 5 of 13 Fig. 3: Lateral Contour Shifts Page 6 of 13 Results For the whole LAD, superior LAD and inferior LAD there was a strong trend towards a decrease in dose when the structure was shifted medially and an increase in dose with lateral shifts. Shifting the whole LAD inferiorly usually increased the reported dose as did a superior shift decrease the dose. Dose to the superior LAD typically increased with inferior shifts, whilst dose to the inferior LAD decreased. This can be explained by these structures moving into or out of the high dose part of the radiation fields. MEAN DOSE Assuming a difference of 10Gy as clinically significant: Whole LAD There were no clinically significant differences seen in mean dose when the whole LAD was shifted up to 15mm in any direction apart from in the medial direction. For medial shifts clinically significant differences were seen for 2 and 6 patients for 10mm and 15mm shifts respectively (insignificant change in dose for shifts up to 5mm). Hence for medial shifts up to 10mm there was no significant change in dose for 8 out of 10 patients (Table1.) Superior LAD There was no clinically significant change in mean dose when the superior LAD was shifted up to 15mm in any direction. Inferior LAD Shifting the inferior LAD in the medial direction resulted in a decrease of mean dose in all ten patients (mean decrease of 8.3Gy, 15.1Gy and 19.7Gy for 5, 10 and 15mm shifts respectively) of which 6 out of the 10 patients had a clinically significant decrease in mean dose with shifts of only 5mm. A lateral shift in the inferior LAD caused an increase in mean dose in all ten patients. The magnitude of change, however was small and required a shift of 10mm or more. Hence, apart from in the medial direction, no patients had a clinically significant change in mean dose when the inferior LAD was shifted only 5mm. Assuming whole LAD mean dose >20Gy is considered clinically significant: Page 7 of 13 For the seven patients who had a baseline mean whole LAD dose of <20Gy, three had an increase in mean dose to >20Gy. This occurred with lateral shifts and inferior shifts as small as 5mm. For the three patients who had baseline mean doses >20Gy, two had a decrease to <20Gy with shifts in the medial and superior direction as small as 5mm. Maximum dose There was significant variability between patients in changes in maximum dose. As seen with mean dose, medial shifts resulted in the largest changes for the superior, inferior and whole LAD. The mean decrease in maximum dose for the whole LAD was 4.2Gy, 12.5Gy and 20Gy for 5mm, 10mm and 15mm shifts respectively, however the range was large (Table 2.) V20 Assuming for the whole LAD V20 >10% is considered clinically significant: For the whole LAD, two patients had a baseline V20 <10%, one of which experienced a rise of V20 to > 10% when the volume was shifted laterally and superiorly (5mm shift). For the remaining 8 patients who had baseline V20 >10%, 6 patients had a drop in V20 to <10% when the volume was shifted medially (6 patients-15mm; 3 patients-10mm; 1 patient- 5mm) Images for this section: Page 8 of 13 Table 1: MEAN DOSE All movements (10 patients x 3 shifts = 30) Direction of change (+ and - = increase or decrease in dose) Table 2: MAXIMUM DOSE All movements (10 patients x 3 shifts = 30) Direction of change (+ and - = increase or decrease in dose) Page 9 of 13 Table 3: MEAN DOSE (Absolute difference as percentage) Page 10 of 13 Conclusion Definition of cardiac structures can be difficult for a number of reasons. Firstly it relies on the precision of planning CT scans. Second, there is much interobserver variability between radiation oncologists in placement of cardiac volumes. Feng et al demonstrated percent overlap of the LAD contours by radiation oncologists with the 'gold standard' 7 ranged from 0-77% . Cardiac and respiratory motion can also influence the uncertainty of target position. A previous study examining displacement of the LAD with respiration found that the displacement was greatest in the inferior direction and lowest in the left-right direction (average of 6mm in the inferior direction at shallow breathing states but up to 8 2.8cm between expiration and deep inspiration) . Wang et al demonstrated the mean displacement of the LAD due to cardiac motion was 2.3mm towards and away from the posterior edge of the treatment fields. The degree of displacement was however very variable and ranged from 3 to 10.9mm and 0 to 4.6mm in the left-right direction. When considering the whole LAD, provided shifts in contouring are within 10mm, there does not appear according to this study to be a clinically significant change in recorded mean dose in 8 out 10 patients. This allows for fairly significant errors in contour placement before one sees a significant change in recorded dose. This also falls within the range of the LAD displacement due to cardiac motion and at least shallow respiration reported in previous studies. However when considering only the inferior LAD, this study demonstrates that whilst there was much variability between patients, the potential margins for error in contour positioning are smaller and are significant for shifts of only 5mm. As expected marked shifts (up to 15mm) of the superior LAD did not result in significant changes in mean dose. This can be explained by posterior location of the superior LAD and thus greater distance from the radiation fields. In this study, patients who had mean whole LAD doses that were 10Gy or above (corresponding to a MMD of 10 or 15mm) were more likely to experience significant changes in dose with shifts, suggesting that such patients should be targeted for review of accurate target delineation. Changes in maximum dose and V20 were variable between patients and can be explained by variability of anatomical relationships between the anterior surface of the Page 11 of 13 heart and the posterior edge of the radiation beams. As a result fairly small shifts can dramatically change maximum dose and V20 values as the volume is shifted in and out of the fields and hence changes in these values may be less predictable. The relevance of establishing the degree to which accurate definition of target volumes influences reported dose is important for future studies of dose-volume effects for cardiac structures. Personal information References 1 M. C. Aznar, S. S. Korreman, A. N. Pedersen, G. F. Persson, M. Josipovic, and L. Specht, 'Evaluation of Dose to Cardiac Structures During Breast Irradiation', Br J Radiol, 84 (2011), 743-6. 2 J. F. Boivin, G. B. Hutchison, J. H. Lubin, and P. Mauch, 'Coronary Artery Disease Mortality in Patients Treated for Hodgkin's Disease', Cancer, 69 (1992), 1241-7. 3 M. Clarke, R. Collins, S. Darby, C. Davies, P. Elphinstone, E. Evans, J. Godwin, R. Gray, C. Hicks, S. James, E. MacKinnon, P. McGale, T. McHugh, R. Peto, C. Taylor, Y. Wang, and Group Early Breast Cancer Trialists' Collaborative, 'Effects of Radiotherapy and of Differences in the Extent of Surgery for Early Breast Cancer on Local Recurrence and 15-Year Survival: An Overview of the Randomised Trials', Lancet, 366 (2005), 2087-106. 4 J. Cuzick, H. Stewart, L. Rutqvist, J. Houghton, R. Edwards, C. Redmond, R. Peto, M. Baum, B. Fisher, H. Host, and et al., 'Cause-Specific Mortality in Long-Term Survivors of Breast Cancer Who Participated in Trials of Radiotherapy', J Clin Oncol, 12 (1994), 447-53. 5 S. C. Darby, M. Ewertz, P. McGale, A. M. Bennet, U. Blom-Goldman, D. Bronnum, C. Correa, D. Cutter, G. Gagliardi, B. Gigante, M. B. Jensen, A. Nisbet, R. Peto, K. Rahimi, C. Taylor, and P. Hall, 'Risk of Ischemic Heart Disease in Women after Radiotherapy for Breast Cancer', N Engl J Med, 368 (2013), 987-98. Page 12 of 13 6 Group Early Breast Cancer Trialists' Collaborative, S. Darby, P. McGale, C. Correa, C. Taylor, R. Arriagada, M. Clarke, D. Cutter, C. Davies, M. Ewertz, J. Godwin, R. Gray, L. Pierce, T. Whelan, Y. Wang, and R. Peto, 'Effect of Radiotherapy after Breast-Conserving Surgery on 10-Year Recurrence and 15-Year Breast Cancer Death: Meta-Analysis of Individual Patient Data for 10,801 Women in 17 Randomised Trials', Lancet, 378 (2011), 1707-16. 7 M. Feng, J. M. Moran, T. Koelling, A. Chughtai, J. L. Chan, L. Freedman, J. A. Hayman, R. Jagsi, S. Jolly, J. Larouere, J. Soriano, R. Marsh, and L. J. Pierce, 'Development and Validation of a Heart Atlas to Study Cardiac Exposure to Radiation Following Treatment for Breast Cancer', Int J Radiat Oncol Biol Phys, 79 (2011), 10-8. 8 R. Jagsi, J. M. Moran, M. L. Kessler, R. B. Marsh, J. M. Balter, and L. J. Pierce, 'Respiratory Motion of the Heart and Positional Reproducibility under Active Breathing Control', Int J Radiat Oncol Biol Phys, 68 (2007), 253-8. 9 G. Nilsson, L. Holmberg, H. Garmo, O. Duvernoy, I. Sjogren, B. Lagerqvist, and C. Blomqvist, 'Distribution of Coronary Artery Stenosis after Radiation for Breast Cancer', J Clin Oncol, 30 (2012), 380-6. 10 L. E. Rutqvist, and H. Johansson, 'Mortality by Laterality of the Primary Tumour among 55,000 Breast Cancer Patients from the Swedish Cancer Registry', Br J Cancer, 61 (1990), 866-8. Page 13 of 13