Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Hygiene hypothesis wikipedia , lookup
Compartmental models in epidemiology wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Epidemiology wikipedia , lookup
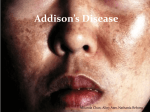
www.healthinfo.org.nz Addison's disease Addison’s disease is a condition where there is deficiency of the hormones made in the adrenal cortex, caused by destruction of the adrenal cortex. Normally there are two adrenal glands located in the abdomen above each kidney. The outer portion of the adrenal called the cortex produces important steroid hormones including cortisol and aldosterone. Cortisol is important for the metabolism of cells, modifying the body’s response to stress. Aldosterone regulates salt and water levels which affects blood volume and blood pressure. Cortisol production is regulated by another hormone, adrenocorticotrophic hormone (ACTH) made in the pituitary gland which is located just behind the nose. Classical Addison’s disease (also called primary adrenal insufficiency) results from a loss of both cortisol and aldosterone secretion due to destruction of both adrenal glands. What causes Addison’s disease? Addison’s disease was first described by Dr Thomas Addison in London in 1855 when the most common cause of Addison’s disease was tuberculosis. Nowadays, the major cause of Addison’s disease in developed countries is an autoimmune condition in which the body’s immune system makes antibodies against cells of the adrenal cortex and slowly destroys them. We do not know why some people’s bodies make antibodies against their adrenal glands but like other autoimmune conditions such as thyroid disease there are likely to be familial or genetic causes. Other less common causes of Addison’s disease include chronic infections besides tuberculosis such as fungal infections, cytomegalovirus (CMV) in association with AIDS, and rarely invasion of the adrenal by cancer cells that have spread from another part of the body, spontaneous haemorrhage into the adrenal glands during shock and surgical removal of both adrenals. Addison’s disease is quite rare with only about six cases diagnosed per million adults per year. What are the symptoms of Addison’s disease? The slowly progressive loss of cortisol and aldosterone secretion that occurs in Addison’s disease usually produces a chronic, steadily worsening fatigue, associated with nausea, poor appetite and some weight loss. Dizziness or light-headedness, particularly on standing, may occur because of lowering of the blood pressure from an excessive loss of salt in the urine. Vomiting may occur and there are often emotional changes including depression. Some people seek out salty foods because of salt loss. The increase in ACTH due to loss of cortisol will often produce a darkening of the skin that may look like excessive suntan. Because the symptoms are slowly progressive they may easily be missed until a sudden event like a flu, accident or need for surgery precipitates dramatic worsening of symptoms because of the inability of the adrenal gland to respond to stress. This is referred to as an “Addisonian crisis” and requires urgent medical treatment. HealthInfo reference: 70626 Issued: 2 August 2016 Page 1 of 3 Addison's disease www.healthinfo.org.nz How is Addison’s disease diagnosed? When symptoms raise the question of Addison’s disease blood tests are usually done to make the diagnosis. These tests measure the amount of cortisol and aldosterone in the blood and usually involve a repeat measure of cortisol after giving an injection of ACTH. An elevated blood level of ACTH is found. Because the salt balance is affected, the kidney hormone renin is also increased. Routine biochemistry and full blood count may also be abnormal with a low blood sodium level, a slightly raised potassium level and a change in white blood cell count. Once the diagnosis of Addison’s disease has been made, tests looking for the cause of the Addison’s disease will usually include a blood test, chest x-ray and sometimes an abdominal scan. How is Addison’s disease treated? Since Addison’s disease is caused by a lack of cortisol and aldosterone the treatment is to replace these hormones. Cortisol is usually replaced by hydrocortisone, which is the same substance as the cortisol naturally produced by the adrenal glands. Hydrocortisone tablets are given as morning and afternoon doses (occasionally patients prefer taking three smaller daily doses). Sometimes cortisone acetate or prednisone are used instead of hydrocortisone. The usual daily dose of hydrocortisone in an adult is between 15 and 25 mg with the larger amount of hydrocortisone given in the morning to mimic the body’s normal cortisol secretion. Some people prefer to take their hydrocortisone in divided doses three times a day. Aldosterone is replaced by a tablet called fludrocortisone (tradename “Florinef”) with the dose ranging between 50 and 200 µg daily. The doses of these medications are adjusted for the individual’s size and other co-existing medical conditions. Since Addison’s disease is a chronic condition, daily replacement medication can never be stopped. Anyone with Addison’s disease should have a medical alert bracelet or pendant so that in an emergency medical staff can give appropriate intravenous fluids and steroids. Do I need to alter my treatment if I am unwell? The body’s normal response to a stress such as an illness is to produce more cortisol. It is therefore important that patients with Addison’s disease know how to alter their medication when they are unwell. Often an individual with Addison’s disease will know more about this than their family doctor who may only have one patient with Addison’s disease in their practice. We recommend that if you have any illness, for example a flu or a bad cold, where you are unwell enough to spend a day in bed then you should double your usual daily dose of hydrocortisone for two days. Provided you are then improving it is reasonable to reduce back to your maintenance dose on the third day. If you have vomiting or diarrhoea then your tablets may not be absorbed properly and you should see your doctor for an injection of hydrocortisone. It is important that you do this sooner rather than later as otherwise you are likely to feel more unwell as time progresses. In this situation we recommend a doctor gives you 50 mg of hydrocortisone either intramuscularly or sometimes into a vein. This can be repeated at eight hourly intervals if you HealthInfo reference: 70626 Issued: 2 August 2016 Page 2 of 3 Addison's disease www.healthinfo.org.nz remain unwell. In a case of a significant accident an injection of hydrocortisone is also indicated. Sometimes people with Addison’s disease or their families are taught how to inject hydrocortisone themselves, particularly if they are going to an isolated area. If you require surgery it is important that the surgeon involved knows you have Addison’s disease as your steroids will usually need to be increased for 24 to 48 hours and they may need to discuss this with an endocrinologist. Are there risks from treatment? The main risk from treatment of Addison’s disease is taking excessive steroids. If too much hydrocortisone is taken over a long period of time it can cause thinning of the bones (osteoporosis). It can also cause you to gain weight and be susceptible to bruising. Too much fludrocortisone can cause headaches and high blood pressure. How is treatment for my Addison’s disease monitored? It is important that your steroid replacement therapy for Addison’s disease is regularly reviewed. This normally requires a visit to an endocrinologist every one or two years for a discussion about symptoms, examination and blood tests. Measuring the blood levels of sodium, potassium, cortisol and a hormone called renin (which tells us whether the dose of fludrocortisone is adequate) are very useful in monitoring the treatment. A scan assessing bone mineral density may also be useful. Are there related diseases? Autoimmune Addison’s disease, the most common cause of Addison’s, can be associated with autoimmune diseases affecting other endocrine glands. The thyroid is most commonly involved and it may be underactive (hypothyroidism) or occasionally overactive. Less frequently associated autoimmune diseases are insulin dependent diabetes mellitus, pernicious anaemia (abnormal absorption of vitamin B12), coeliac disease (a gut disorder) and early menopause. Can people with Addison’s live a normal life? As long the correct dose of replacement steroid medication is taken every day a person with Addison’s disease can have a normal crisis-free life. There are no specific physical or occupational restrictions and life expectancy should be normal. For strenuous exercise such as tramping, a temporary increase in steroid dose may be necessary. In very hot weather, the body loses more salt and additional fludrocortisone is often needed. Having a yearly flu vaccination is a good idea. Pregnancy requires extra monitoring of medication, with increased steroid for labour. Breast feeding is fine. Remember to have regular check-ups and use extra medication during illness. Written by the Department of Endocrinology, Christchurch Hospital.Endorsed by HealthInfo clinical advisers. Updated August 2016. 70626 HealthInfo reference: 70626 Issued: 2 August 2016 Page 3 of 3