Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
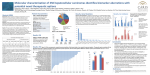
Evaluation Of High Stage Skin Squamous Cell Carcinoma (SSCC) By Next Generation Sequencing (NGS) Opens The Door For New Routes To Targeted Therapies 1 1 2 1 1 2 2 2 2 2 2 2 2 RN Al-Rohil , A Tarasen , K Wang , CE Sheehan , JA Carlson ,GA Otto , G Palmer , R Yelensky , D Lipson , SM Ali , D Morosini , VA Miller , PJ Stephens , JS Ross 1Department 1, 2 of Pathology and Laboratory Medicine, Albany Medical College, Albany, NY, 2Foundation Medicine, Inc., Cambridge, MA Abstract Background: Although skin squamous cell carcinomas (SSCC) are rarely high stage, on occasion they can be life threatening both due to local extension or metastasis. We hypothesized that comprehensive genomic profiling of high stage SSCC could identify genomic-derived drug targets of therapy for patients with conventional therapy-resistant disease. Methods: Hybridization capture of3,769 exons from 236 cancer-related genes and 47 introns of 19 genes commonly rearranged in cancer was applied to ≥ 50ng of DNA extracted from 25 SSCC FFPE specimens and sequenced to high, uniform coverage. Genomic alterations (base substitutions, small indels, rearrangements, copy number alterations) were determined and then reported for these patient samples. Actionable GA was defined as those identifying anti-cancer drugs on the market or in registered clinical trials (CT). Results: There were 23 male and 2 female SSCC patients with a median age of 70 years (range 48-91 years). Fourteen (56%) SSCC were grade 2 and 11 (44%) grade 3. Fourteen (56%) SSCC were stage III and 11 (44%) were stage IV at time of sequencing. A total of 161 alterations were identified for an average of 6.44 alterations per tumor with 25/25 (100%) of patients harboring at least one alteration. The dominant mutational signature reflects DNA damage due to ultraviolet light exposure, a known risk factor for SSCC. The most common nonactionable GA were alterations in TP53 (88%), NOTCH2 (20%) and MLL2 (20%). Twenty-one (84%) of SSCC had at least 1 actionable GA with an average of 2.08 actionable GA per patient including mutation, amplification or homozygous deletion of CDKN2A (60%), NOTCH1 (40%), ERBB2 (12%), FGFR3 (12%), NF1 (8%), NF2 (8%), PIK3CA (8%), SMARCACB1 (8%), BRAF (4%), BRCA1 (4%), BRCA2 (4%), CCND1 (4%), EGFR (4%), HRAS (4%), PIK3R1 (4%), PIK3R2 (4%) and PTCH1 (4%). Conclusions: More than three-quarters of SSCC patients harbored actionable GA which has the potential to treat high stage tumors with targeted therapeutic agents in addition or in replacement of the currently available treatment options. Design and Methods • Hybridization capture of 3,769 exons from 236 cancer-related genes and 47 introns of 19 genes commonly rearranged in cancer • ≥ 50ng of DNA extracted from 25 SSCC FFPE specimens • Samples were sequenced to high (average 774X), uniform coverage • Genomic alterations (base substitutions, small indels, rearrangements and copy number alterations) were determined and then reported for these patient samples • Actionable GA were defined as those identifying anti-cancer drugs on the market or in registered clinical trials (CT). Case Examples Results • • • • • • 23 male and 2 female SSCC patients with a median age of 70 years (range 48-91 years) 14 (56%) SSCC were grade 2 and 11 (44%) grade 3. 14 (56%) SSCC were stage III and 11 (44%) were stage IV at time of sequencing. 161 total GA were identified for an average of 6.44 GA per tumor 25/25 (100%) of patients harboring at least one alteration The dominant mutational signature reflects DNA damage due to ultraviolet light exposure, a known risk factor for SSCC. • The most common non-actionable GA were alterations in TP53 (88%), NOTCH2 (20%) and MLL2 (20%). • 21 (84%) of SSCC had at least 1 actionable GA with an average of 2.08 actionable GA per patient including mutation, amplification or homozygous deletion of CDKN2A (60%), NOTCH1 (40%), ERBB2 (12%), FGFR3 (12%), NF1 (8%), NF2 (8%), PIK3CA (8%), SMARCACB1 (8%), BRAF (4%), BRCA1 (4%), BRCA2 (4%), CCND1 (4%), EGFR (4%), HRAS (4%), PIK3R1 (4%), PIK3R2 (4%) and PTCH1 (4%). Clinical Features and Genomic Alterations in 25 Cases of High Stage Cutaneous Squamous Cell Carcinoma Case Sex Age Specimen Tumor Tumor Total Therapies Therapies Clinical Altered Genes # used for Grade Stage at GA w/ w/ lack of trials NGS time of potential response NGS benefit 1 2 3 4 5 6 M M M M M M 51 53 84 87 88 76 7 M 69 8 9 10 11 12 13 14 15 16 17 F M M M M M F M M M 62 58 70 79 70 64 91 73 48 61 18 M 19 20 21 22 23 24 25 SKIN SKIN SKIN SKIN SKIN SKIN PAROTID GLAND SKIN SKIN SKIN BONE SKIN SKIN SKIN SKIN SKIN SKIN II II II II II III III III IV III III III 7 7 4 9 6 3 1 2 0 9 5 0 0 0 0 0 0 0 7 13 3 12 6 0 CDKN2A; FGFR3; NOTCH1; SMAD4; TP53 ATR; BRCA1; CDKN2A; PIK3CA; SMARCB1;TP53; USP3X CDKN2A; GARA1; NOTCH1; TP53 APC; CDKN2A; KIT; NF2; TP53 CDKN2A; CTNNB1; EGFR; EZH2;TP53 NOTCH1; TP53 II IV 2 0 0 0 NOTCH1; TP53 II II III III II II II III III III III III III IV III III IV III IV IV 7 7 2 6 9 5 7 10 6 8 0 2 0 0 0 0 0 0 2 3 0 0 0 0 0 0 0 0 0 0 6 8 2 5 1 3 5 5 5 5 ATM; BRAF; CDKN2A; TP53 ALK; ASKL1; MYCN; PIK3CA; SMARCB1; TP53 CDKN2A; MLL2; CDKN2A; DNMT3A; GNA11; HGF; TP53 ASXL1; LRP1B; NOTCH1; NOTCH2; TP53 CDKN2A; NOTCH2; SMAD2; TP53 ASXL1; BRCA2; CDKN2A; KDMA6; LRP1B; NOTCH2; TP53 CDKN2A; NOTCH1; PALB2; RUNX1; TP53 CCND1; FGFR3; FGF13; PIK3R2; TP53 ARID2; CDKN2A; ERBB4; MLL2; NOTCH1; NOTCH2; TP53 77 SKIN III IV 1 0 0 2 M M M M 48 83 75 84 SKIN SKIN SKIN SKIN II III II III III III IV IV 17 2 8 6 3 0 2 12 0 0 0 0 7 1 5 9 M M M 69 SKIN 54 SKIN 71 SKIN III II III IV IV III 8 9 5 3 7 7 0 0 0 5 9 6 NRAS; ARID2; ASXL1; BARD1; BRCA2; CDKN2A; CREBB2; GRIN2A; MLL2; MPL; NF1; PIK3R1; SMARCB1; TP53 RB1; TP53 CREBB2; FGFR3; KDM6A; MCL1; RB1; SETD2; TP53 CDKN2A/B; KDR; KIT; MLL2; NOTCH1; TP53 APC; ARID2; CDKN2A; NF1; NOTCH1; NOTCH2; TET2; TP53 ERBB4; MLL2; NF2; NOTCH1; TET2; TP53 ARID1A; ERBB4; PIK3CA; PTCH1; Case 5. Stage III cutaneous SCC in an 87 year old man with EGFR amplification and mutation. EGFR R831H is a missense mutation that is located in the protein kinase domain of the protein. This mutation has been reported to be activating (Foster J et al 2010). EGFR has reported to be mutated in 1% of the skin squamous cell carcinoma samples examined (COSMIC). Amplification of EGFR has ranged from 1% of the skin cancers analyzed (The cBio Cancer Genomics Portal) to 20% of (Toll A et al 2010). Activating mutations, amplification, or overexpression of EGFR may predict sensitivity to Egfr inhibitors Cetuximab is approved in head-and-neck squamous cell cancer and other Egfr-targeted therapies, such as erlotinib and gefitinib, are being studied in clinical trials of metastatic cutaneous SCC. EGFR kinase domain missense mutation (Integrated Genomics Viewer, Broad Institute) Copy number plot showing EGFR amplification. Case 25. A stage III cutaneous SCC with basaloid features in a 71 year old man with alterations in ARID1A, ERBB4, PIK3CA and PTCH1. PTCH1 encodes the protein Ptc1, a receptor for sonic hedgehog (Shh), indian hedgehog (Ihh), and desert hedgehog (Dhh) (Kogerman et al 2002). The two alterations in PTCH1 in this case are both inactivating. PTCH1 mutations have been reported in 8% (6/73) of skin squamous cell carcinoma (SCC) samples (COSMIC). PTCH1 mutation in cutaneous SCC has not been significantly studied in the scientific literature. Alterations in PTCH1 have been observed in lung and head and neck SCC and correlated with an increased rate of recurrence and poor prognosis (Ghosh et al 2013). Loss of PTCH1, by mutation, deletion, or silencing, has been shown to result in constitutive activation of the hedgehog signaling pathway and may predict sensitivity to Smo inhibitors such as vismodegib. Trials of vismodegib and other Smo inhibitors continue in multiple tumor types including metastatic cutaneous SCC.. PTCH1 Q576* and splice site 1347+1G>A mutatations (Integrated Genomics Viewer, Broad Institute) Conclusions More than three-quarters of SSCC patients harbored actionable GA which has the potential to treat high stage tumors with targeted therapeutic agents in addition or in replacement of the currently available treatment options. References Frampton GM, Fichtenholtz A, Otto GA et al. Development and validation of a clinical cancer genomic profiling test based on massively parallel DNA sequencing. Nat Biotechnol. 2013;31(11):1023-31.