Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
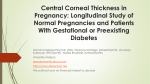
June 2009 A. Elias et al. - CCT 149 ORIGINAL ARTICLE Central Corneal Thickness and Relating Factors - A Prospective Observational Study Dr. Anna Elias DNB, Dr. A. Giridhar MS DO, Dr. Mahesh G. MS DO DNB FRCS(Ed), Dr. Savita Bhat MS DO DNB MNAMS, Dr. Ramkumar DO MS Abstract Aim: To investigate the association between central corneal thickness and degree of myopia, corneal curvature, axial length and age. Methods: It was a prospective observational study. 53 emmetropic subjects and 53 myopes were studied. Central corneal thickness was measured in all patients with an ultrasonic pachymeter. Axial length was measured using an A-scan and corneal curvature was measured using a Keratometer. CCT was correlated with degree of myopia, axial length, corneal curvature and age using the Karl Pearson’s Correlation Coefficient. Results: 106 patients (203 eyes) were recruited for the study. The age of patients ranged from 18 to 45 years, with a mean of 32 years. Myopia ranged from –0.5D to –17.5D with a mean of –2.8D. The mean CCT was 543.11 microns. The mean axial length was 23.69 mm and the mean corneal curvature was 43.68D. Karl Person’s Correlation Coefficient was as follows: CCT & degree of myopia : r = 0.11 p = 0.122 CCT & corneal curvature : r = - 0.23 p = 0.001 CCT & axial length : r = 0.038 p = 0.944 CCT & age : r = 0.0048 p = 0.696 Conclusion: There was no correlation between CCT & degree of myopia. There was a significant negative correlation between CCT & corneal curvature. There was no correlation between CCT & age or axial length. Key Words: Myopia, CCT Introduction Although the true etiology of myopia is still unknown, the cornea is responsible for approximately two-thirds Giridhar Eye Institute, Ponneth Temple Road, Kadavanthara, Cochin – 682 020, Email: [email protected] of optical refraction and its role in myopia has consequently been studied intensely over the years. Most of the changes in the myopic eye are located in the posterior segment namely, thinning of the retina and sclera, posterior staphyloma, choroidal atrophy and 150 Kerala Journal of Ophthalmology a higher incidence of retinal detachment. Changes in the anterior segment associated with myopia are still under debate. The myopic eye is known to be longer than the normal emmetropic eye. If this is the result of general growth, one might expect the cornea to have grown thicker than normal. If instead, the myopic eye is larger due to a mechanism similar to that of a balloon being inflated, one would expect the cornea to be thinner than normal according to a simple stretching theory. An emmotropic eye could then be compared to a sphere and a myopic eye to a prolate spheroid 1. Myopia is increasing in prevalence among the populations of East Asian origin. Estimates of the proportion of myopia in the young population of South East Asian countries range from 30% to 60%. 2 With increasing rates of myopia, refractive surgery such as laser in situ Keratomileusis (LASIK) has become popular in Asia. When undertaking such surgery to correct myopia, central corneal thickness (CCT) is an important consideration to prevent the cornea from becoming too thin after treatment. Studies that have attempted to investigate the effect of refractive errors on CCT have reported conflicting results. Some studies have reported no correlation between corneal thickness and level of myopia 3, whereas some studies have found the cornea to be thinner in more myopic eyes 4. Central corneal thickness (CCT) indicates corneal physiologic health and affects the measurement of intra ocular pressure (IOP). A thin central cornea is a risk factor for development of glaucoma in patients with ocular hypertension 5. A thin scleral bed in deeply excavated optic nerves has been the quintessential finding in advanced glaucomatous eyes. 6 This has further led to a hypothesis that thinness of the corneas may be an indication of generalized weakness of the ocular integument associated with longer eyes with a thin scleral bed of lamina cribrosa. Studies have tried to determine if thin corneas are associated with longer globes. 7 Aim The purpose of the study was to determine the correlation between CCT and 4 variables, namely, degree of myopia, corneal curvature, axial length and age of the patient. Vol. XXI, No. 2 Materials & Methods A prospective observational study was done. 106 consecutive patients were enrolled in the study; 53 patients were myopes and 53 patients were emmetropes. Patients were in the age group 18 years to 45 years. Subjects with previous ocular surgery, glaucoma or any disease affecting the corneal thickness were excluded. All patients underwent a complete ophthalmic evaluation. Central corneal thickness was measured with an ultrasonic pachymeter (Pacscan 300p, digital biometric ruler, Sonomed). Axial length was measured using an A Scan (Echorule2, Biomedix). Corneal curvature was measured using a Keratometer. Statistical Analysis was done using SPSS V.11 and Microsoft Excel. Correlation between CCT and four factors namely, degree of myopia, axial length , corneal curvature and age of patient was studied using Karl Pearson’s correlation co-efficient. A probability of 0.05 was considered statistically significant. Results 106 patients (203 eyes) were recruited for the study. 53 patients were myopes and 53 patients were Table 1 Demographic Features of Study Patients No. of patients No. of Eyes No. of Myopes No. of Emmetropes Age: Range (years) Mean (SD) Median Sex: Females Males 106 203 53 53 18 – 45 32 (8.17) 32 66 40 Table 2. Demographic Features of Myopia & central corneal thickness – split in groups Myopes (Diopters) 0–3 3–6 More than 6.0 CCT (Microns) < 500 500 – 550 550 – 600 > 600 No. of patients 68 21 10 11 51 34 3 June 2009 A. Elias et al. - CCT Table 3. Characteristics of central corneal thickness & Myopia in patients central corneal thickness (Microns) Range Mean (SD) Median Myopia (Diopters) Range Mean (SD) Median 453- 620 543.11 (30.61) 541 17 - 2.8 (2.65) -2 Table 4. Characteristics of Corneal Curvature & Axial Length of patients. Corneal Curvature: (Diopters) Range Mean (SD) Median Axial Length (MM) Range Mean (SD) Median 39.37 – 47.50 43.68 (1.41) 43.62 22.03 – 30.88 23.69 (1.31) 23.48 Table 5. Correlation between central corneal thickness & relating Factors. Karl Pearson’s Correlation Correlation Analysis CCT & degree of myopia CCT & corneal curvature CCT & axial length CCT & age Co-efficient 0.11 -0.23 0.0048 0.038 P value 0.122 0.001 0.944 0.696 emmetropes. There were 66 female patients and 40 male patients. Patients in the age group 18 – 45 years were included in the study. Mean age was 32 yrs. (SD 8.17, median 32 yrs.)(Table 1). Myopia and CCT were split into groups (Table 2) . Most of the patients were in the 0-3.0 diopters group (Fig2). 51 of the 99 myopic eyes had a range of 500-550 microns.(Fig1). Table 3 sumarises the features of central corneal thickness and myopia in study patients. The mean central corneal thickness was 543.11 μm(SD 151 30.61, range 453 – 620 μm, median 541μm). The mean myopia was –2.8 diopters (SD 2.65, range –0.5D to – 17.5D, median – 2D). Table 4 shows the features of corneal curvature and axial length in study patients. The mean corneal curvature was 43.68 diopters (SD 1.41, range 39.37D – 47.50D, median 43.62D) . The mean axial length was 23.69 mm (SD 1.31, range 22.03mm – 30.88 mm, median 23.48). Correlation between CCT and 4 variables was analysed using the Karl Pearson’s Correlation Coefficient. There was a statistically significant negative correlation between CCT and corneal curvature, r = -0.23, P=0.001. (Fig.5). There was no significant correlation between CCT and degree of myopia, axial length or age. (Table 5) (Fig. 3, 4, 6). Discussion The study attempted to determine the correlation between CCT and four variables, namely degree of myopia, corneal curvature, axial length and age of the patient. The mean (SD) CCT was 543.11 (30.61) microns. This is comparable with similar studies. Fam et al 2 in a study on 714 Chinese patients had a mean of 534.5 microns. Chang’s 8 series had a mean of 533 microns, whereas Vijaya et al 9 reported the mean (SD) CCT in a normal rural South Indian population to be 505.9 (31.10)microns. This study showed no statistically significant difference between CCT in myopes and emmetropes. There was no correlation between degree of myopia and CCT (Pearson r = 0.11, P=0.122). This result is in Table 6. Results of Studies showing correlation between central corneal thickness & Myopia Authors Year Country Equipment Results (CCT & Myopia) Liu & Pflugfelder Cho & Lam Price et al Ehlers & Hansen Touzeau et al Srivannaboon Alsbirk Von Bahr Kunert et al 2000 1999 1999 1976 2003 2002 1978 1956 2003 China China USA Denmark France Thailand Greenland Sweden India Orbscan Ultrasound Ultrasound Optical Orbscan Orbscan Optical Optical Ultrasound No correlation No correlation No correlation No correlation Thinner CCT when Myopic Thinner CCT in high Myopes Thinner CCT when Myopic Thinner CCT when Myopic Thinner CCT in high myopia 152 Kerala Journal of Ophthalmology Fig. 1. Histogram showing the distribution of CCT in the study population. Fig. 2. Histogram showing the distribution of myopia in the study population. Fig. 3. Scatter plot showing the association between CCT and degree of myopia. agreement with majority of previous studies (1). Von Bahr 4 first generated interest in the correlation between myopia and CCT in 1956, when he reported thinner corneas in myopia less than –4D. Similar findings were also reported by Tokoro et al 10, Chang et al 8, Touzeau et al, Srivannaboon and Alsbirk from Greenland. However other studies by Liu Z and Pflugfelder 11, Price et al 12 and Pedersen et al 1 could find no correlation between CCT and degree of myopia. Table 6 gives an Vol. XXI, No. 2 Fig. 4. Scatter plot showing the association between CCT and age. Fig. 5. Scatter plot showing the association between CCT and Corneal curvature. Fig. 6. Scatter plot showing the association between CCT and axial length. overview of published papers with information on myopia and central corneal thickness. There was a negative correlation (Pearson r= -0.23) (P=0.001) between CCT and corneal curvature. The correlation was significant at the 0.01 level (2-tailed). Similar results were reported by Atsuo Tomidokoro et al in the Tajimi Study from Japan 13. A study done on Singaporean children 14 showed that the radius June 2009 A. Elias et al. - CCT of corneal curvature correlated with CCT (Pearson r = 0.19, P< 0.001) significantly. There was no correlation between CCT and axial length. Mitsugu Shimmyo et al 7 in their study, corneal thickness and axial length, studied ocular parameters of 1084 eyes. They found no statistically significant association between CCT and axial length. Subgroup analysis by age, gender and race failed to show an association. There was no statistically significant association between CCT and age. (Pearson r = 0.038, P = 0.696). Other studies have shown CCT to be inversely related to age. In the study by Eun Suk Lee et al, CCT of Korean patients with glaucoma showed an inverse relationship between age and CCT (Pearson r = -0.12; P < 0.0001). CCT decreased by 2.8 microns per decade. This relation was also significant in the multivariate model (P=0.01). Myopia is increasing in prevalence and may be a growing problem in the future. Investigations in Denmark, Iceland, Japan and North American aboriginal populations have indicated the increasing prevalence of myopia. Consequently there is a higher rate of refractive surgeries to correct myopia. With Lasik there is a general concern that one should not thin the cornea further than a given amount. It is therefore prudent to measure central corneal thickness prior to surgery. A thin central cornea is a risk factor for the development of glaucoma in patients with ocular hypertension. In the Ocular Hypertension Treatment Study (OHTS), a multivariate model that included IOP, CCT was the most powerful component of the predictive model. CCT is the most heritable aspect of ocular structure (more than refraction, axial length or optic disc size), suggesting it is under exquisite genetic control. Conclusions This study has shown that CCT has no correlation with degree of myopia. CCT was significantly associated with corneal curvature. There was no association between CCT and axial length or age. 153 References 1. Pederson L, HjortdalJ, Ehlers N. Central corneal thickness n high myopia. Acta Ophthalmol. Scand. 2005; 83:539-42. 2. H-B Fam, ACS How, M Bhaskaran, K-L Lim, Y-H Chan, T Aung. Central Corneal thickness and its relationship to myopia in Chinese adults. Br J Ophthalmol 2006; 90:1451-1453. 3. Wensor M, McCarty CA, Taylor HR. Prevalence and risk factors of myopia in Victoria, Australia. Arch Ophthalmol 1999; 117: 658-63. 4. Von Bahr G. Corneal thickness: its measurement and changes. AM J Ophthalmol 1956; 42:251-66. 5. Gordon MD, Beiser JA, Brandt JD etal. The ocular hypertension study : baseline factors that predict the onset of primary open angle glaucoma. Arch Ophthalmol 2002; 12:714-720 6. Quigley HA, Hahman RM, Addicks EM, Massof RW, Green WR. Morphologic changes in the lamina cribrosa correlated with neural loss in open angle glaucoma. Am J Ophthalmol 1983; 95:673-691. 7. Mitsugu Shimmyo, Pasul N. Orloff. Corneal Thickness and Axial Length. Am J Ophthalmol 2005;139: 553-554. 8. Chang SW, Tsai IL, HuFR, etal. The cornea in young myopic adults. Br J Ophthalmol 2001; 85:916-20. 9. Vijaya L, George R, Paul PG, etal. Prevalence of open angle glaucoma in a rural South Indian population. Invest Ophthalmol Vis Sci 2005; 46:4461-7. 10. Tokoro T, Hayashi K, Muto M, et al. central corneal thickness in high myopia. Folia Ophthalmol Jpn 1976; 27:610. 11. Liu Z, Pflugfelder Sc. The effects of long term contact lens wear on corneal thickness, curvature and surface regularity. Ophthalmology 2000; 107:105-11. 12. Price FW Jr, Koller DL, Price MO> Central corneal Pachymetry in patients undergoing laser in situ Keratomileusis. Ophthalmology 1999; 106: 2216-20. 13. Atsuo Tomidokoro, Makoto Araie, Aiko Iwase & the Tajimi Study Group. Corneal Thickness and Relating Factors in a Population – Based study in Japan: The Tajimi Study. AmJ Ophthalmol 2007; 144: 152-154. 14. Tong L, Saw Seang Mei, Siak Jykuen, Gazzard G, Tan D. Corneal thickness determination and correlates in Singaporean school children. Investigative Ophthalmology and amp; Visual Science, 2004; 45:4004-9.