Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
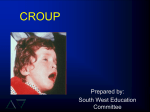
A variety of pediatric medical problems can activate the EMS system The majority of childhood medical emergencies involve the respiratory system Other systems may be involved Infectious diseases may be caused by the infection or infestation of the body by an infectious agent Virus, bacterium, fungus, or parasite Most infections are self-limiting Some infections may be life threatening Meningitis, pneumonia, and septicemia Fever Chills Tachycardia Cough Sore throat Nasal congestion Malaise Tachypnea Cool or clammy skin Petechiae Respiratory distress Poor appetite Vomiting Diarrhea Dehydration Hypoperfusion Purpura Seizures Severe headache Irritability Stiff neck Bulging fontanelle Take all Standard Precautions Become familiar with the common pediatric infections encountered in your area Previous exposure to disease and vaccinations The most common reason EMS is summoned to care for a pediatric patient Your approach to the child with a respiratory emergency will depend on the severity of respiratory compromise Three categories Respiratory distress Respiratory failure Respiratory arrest Learn in to recognize the phase your patient is Mildest form of respiratory impairment Increased work of breathing Increase in respiratory rate Frequently estimated Should be measured for at least 30 seconds Normal mental status deteriorating to irritability or anxiety Tachypnea Retractions Nasal flaring (in infants) Poor muscle tone Tachycardia Head bobbing Grunting Cyanosis that improves with supplemental oxygen Occurs when the respiratory system is not able to meet the demands of the body for oxygen intake and for carbon dioxide removal Characterized by inadequate ventilation and oxygenation Irritability or anxiety deteriorating to lethargy Marked tachypnea later deteriorating to bradypnea Marked retractions later deteriorating to agonal respirations Poor muscle tone Marked tachycardia later deteriorating to bradycardia Central cyanosis The end result of respiratory impairment The cessation of breathing Typically follows a period of bradypnea and agonal respirations Unresponsivenes deteriorating to coma Bradypnea deteriorating to apnea Absent chest wall motion Bradycardia deteriorating to asystole Profound cyanosis Should be based on the severity of the problem Goals of management Increasing ventilation Increasing oxygenation Airway Patency Assure continued maintenance of the airway Breathing Administer high-flow, high-concentration oxygen If no improvement the patient should be treated more aggressively Treatment of late respiratory failure or arrest Mechanical ventilation with a BVM device Endotracheal intubation Consideration of gastric decompression Consideration of needle decompression If suspected pneumothorax Consideration of cricothyrotomy Circulation You should obtain venous access Transport to an appropriate facility Continue to reassess the child Provide emotional and psychological support Upper airway distress Croup Epiglottitis Bacterial Tracheitis Foreign Body Aspiration Viral infection of upper airway Occurs in children 6 months to 4 years of age Leads to edema beneath the glottis and larynx Assessment Child will have a mild cold or other infection Develops loud, brassy cough at night You should never examine the oropharynx Difficult to distinguish from epiglottitis Management Position of comfort Cool, mist oxygen Administration of racemic epinephrine or albuterol may be considered An acute infection and inflammation of the epiglottis Caused by a bacterial infection Haemophilus influenzae type B Tends to strike children 3–7 years old Assessment Child awakens with a high temperature and a brassy cough Pain upon swallowing, sore throat, high fever, shallow breathing, dyspnea, inspiratory stridor, and drooling Never attempt to visualize airway Patients will often assume the “tripod position” Management Appropriate airway maintenance and oxygen administration If the airway becomes obstructed: Two-rescuer ventilation with BVM is almost always effective © Ken Kerr Management Intubation equipment is available (cont.) Contraindicated unless obstruction occurs Immediate transport Handle gently Do not visualize airway Avoid IV sticks Bacterial infection of the airway, subglottic region Afflicts mainly infants and toddlers 1–5 years May follow episode of croup Assessment Presence of a high-grade fever accompanied by coughing up of pus and/or mucous Hoarse voice Inspiratory or expiratory stridor Management Manage airway and breathing Ventilations may require high pressure Oxygen by mask or blow-by Depress pop-off valve on BVM Consider intubation only in cases of complete airway obstruction The number one cause of in-home accidental deaths in children under 6 years Food or foreign objects Assessment Partial Complete Management If the obstruction is partial: Make the child as comfortable as possible and administer humidified oxygen Have intubation equipment available Transport If complete: Utilize basic life support techniques Visualize the airway with a laryngoscope Lower Airway Distress Asthma Bronchiolitis Pneumonia Foreign Body Lower Airway Obstruction Chronic inflammatory disorder of the lower respiratory tract Pathophysiology Characterized by bronchospasm and excessive mucous production Widespread, but variable, airflow obstruction The airways become hyperresponsive Pathophysiology (cont.) “Triggers” Two-phase reaction occurs Release of chemical mediators such as histamine Bronchoconstriction Responds to bronchodilator medications Inflammation of the bronchioles as cells of the immune system invade the respiratory tract Additional edema and further decreases in expiratory airflow Assessment Can often be differentiated from other pediatric respiratory illnesses by history Medications may also be an indicator Usually sitting up, leaning forward, and tachypneic Wheezing may be heard An ominous finding is lack of wheezing Management Establish an airway Supplemental, humidified oxygen Pharmacological interventions Inhaled beta agonist Nebulized bronchodilator medications Steroid administration © Ken Kerr Status Asthmaticus Severe, prolonged asthma attack that cannot be broken by aggressive pharmacological management Child will have greatly distended chest Patient is usually exhausted, severely acidotic, and often dehydrated Prepare for intubation Respiratory infection of the medium-sized airways Caused by a viral infection Respiratory syncytial virus (RSV) Characterized by prominent expiratory wheezing and clinically resembles asthma Assessment Distinguish from asthma A low-grade fever often exists Major distinguishing factor is age Asthma does not occur < 1 year of age Management Administer humidified oxygen by mask or blow-by method Support ventilations Equipment for intubation should be readily available Consider bronchodilator by nebulizer An infection of the lower airway and lungs Bacterial or viral Most commonly appears in infants, toddlers, and preschoolers ages 1–5 years Assessment History of a respiratory infection Low-grade fever, decreased breath sounds, crackles, rhonchi, and pain in the chest area Management Ensure a patent airway and administer supplemental oxygen Support ventilations as needed Emotional and psychological support to the parents A foreign body can enter the lower airway if it is too small to lodge in the upper airway The foreign body can act as a one-way valve May trap air in distal lung tissues or prevent aeration of distal lung tissues Assessment History often includes information about the child having a foreign body in the mouth Considerable, often intractable, coughing May have diminished breath sounds Management Management of an aspirated foreign body is supportive Inadequate Ultimately results in tissue hypoxia and metabolic acidosis Shock perfusion of the tissues is an unusual occurrence in children Will lead to cardiopulmonary arrest Causes Hypothermia, dehydration, infection, septicemia, trauma, and blood loss Compensated shock The body is able to compensate for decreased tissue perfusion through various physiological mechanisms Signs and symptoms Irritability or anxiety Tachycardia Tachypnea Weak peripheral pulses, full central pulses Delayed capillary refill (more than 2 seconds in children less than 6 years of age) Cool, pale extremities Systolic blood pressure within normal limits Decreased urinary output Decompensated Compensatory mechanisms begin to fail Blood pressure falls Signs and symptoms Lethargy or coma Marked tachycardia or bradycardia Absent peripheral pulses, weak central pulses Markedly delayed capillary refill Cool, pale, dusky, mottled extremities Hypotension Markedly decreased urinary output Absence of tears Irreversible Treatment measures are inadequate or too late to prevent significant tissue damage and death Despite resuscitation, organ death occurs Best treatment is prevention Shock Cardiogenic Hypovolemic Obstructive Distributive May can be classified in a number of ways: be classified into two categories: Cardiogenic Non-cardiogenic Hypovolemic Results from loss of intravascular fluids Treatment Airway management Fluid bolus 20 mL/kg Children may require 80–100 mL/kg of fluid Distributive Shock A marked decrease in peripheral vascular resistance Causes include: Septicemia from bacterial infection Anaphylactic reaction Damage to the brain and/or spinal cord Caused by sepsis Result of an infection The septic child is critically ill Management Supplemental oxygen Intravenous Access Fluid bolus 20ml/kg Consider initiating pressor therapy Epinephrine Dopamine Results from exposure to an antigen to which the patient has been previously exposed Results in widespread vasodilation Signs and Symptoms Tachycardia Tachypnea Wheezing Urticaria (hives) Anxiousness Edema Hypotension Management Airway maintenance Intravenous access Decompensated shock Administer epinephrine 1:10,000 intravenously Administer diphenhydramine Compensated shock Administer epinephrine 1:1,000 subcutaneously Sudden peripheral vasodilation Interruption of nervous control of the peripheral vascular system Results from trauma Management Stabilization of the injury and administration of supplemental oxygen Administration of a pressor agent Congenital Primary cause of heart disease in children Common symptom of congenital heart disease is cyanosis Heart Disease Mixing of blood Child with congenital heart disease may develop respiratory distress, congestive heart failure, or a “cyanotic spell” Congenital Administer high-flow, high-concentration oxygen Heart Disease (cont.) Ventilate as necessary Start an intravenous line Monitor ECG If the patient is having a cyanotic spell: Place the child in the knee–chest position facing downward Older child can squat Cardiomyopathy A disease or dysfunction of the cardiac muscle Can be result of congenital heart disease or infection Cardiomyopathy causes mechanical pump failure Signs and symptoms Early fatigue, crackles, jugular venous distension, engorgement of the liver, and peripheral edema Cardiomyopathy Supplemental oxygen should be administered IV access (cont.) Restrict fluids Should be treated with furosemide and pressor agents (dobutamine, dopamine) Dysrhythmias Dysrhythmias in children are uncommon Bradydysrhythmias are most common Dysrhythmias can cause pump failure ultimately leading to cardiogenic shock Very limited capacity to increase stroke volume Supraventricular Narrow complex tachycardia tachycardia HR > 220 bpm Does not allow time for adequate cardiac filling Signs and symptoms Irritability, poor feeding, jugular venous distension, hepatomegaly (enlarged liver), and hypotension Ventricular Tachycardia Rare in children Occasionally seen with drowning or following a prolonged resuscitation attempt Signs and symptoms Poor feeding, irritability, and a rapid, wide complex tachycardia Click here to view the Tachycardia Management Algorithm. Reproduced with permission from “2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care,” Circulation 2005, Volume 112, IV-177. © 2005 American Heart Association. Most common type of pediatric dysrhythmia Most frequently result from hypoxia Signs and symptoms A slow, narrow complex rhythm Child may be lethargic or exhibiting early signs of congestive heart failure Click here to view the Bradycardia Management Algorithm. Reproduced with permission from “2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care,” Circulation 2005, Volume 112, IV-176. © 2005 American Heart Association. Asystole may be the initial rhythm seen in cardiopulmonary arrest Child with asystole is pulseless and apneic Follow pulseless arrest algorithm Ventricular fibrillation/ventricular tachycardia Exceedingly rare in children May be result of electrocution or drug overdose Follow pulseless arrest algorithm Pulseless The presence of a cardiac rhythm without an associated pulse Due to noncardiogenic causes Electrical Activity Correct the underlying problem Follow pulseless arrest algorithm Click here to view the Pulseless Arrest Algorithm Reproduced with permission from “2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care,” Circulation 2005, Volume 112, IV-173.© 2005 American Heart Association. Seizures An abnormal discharge of neurons in the brain May be partial or generalized Status Epilepticus Febrile seizures Occur most commonly between the ages of 6 months and 6 years Assessment History is a major factor in determining seizure type Determine how many seizures occurred during the incident Note any current medications The physical examination should be systematic Fever Hypoxia Infections Idiopathic epilepsy (of unknown origin) Electrolyte disturbances Head trauma Hypoglycemia Toxic ingestions or exposure Tumor CNS malformations Management Do not restrain patients Maintain airway Administer supplemental oxygen Establish IV Medications Diazepam Can be administered rectally Acetaminophen An infection of the meninges May be bacterial or viral Bacterial infections can be rapidly fatal Assessment History Illness, fever, and stiff neck Infants do not develop stiff neck Lethargy and poor feeding Assessment (cont.) The fontanelle may be bulging or full Extreme discomfort with movement Rash may develop Management Supportive Treat for shock Nausea Symptoms of other disease processes and Vomiting Most common causes include fever, ear infections, and respiratory infections Gastroenteritis Risk of dehydration and electrolyte imbalance Treatment is primarily supportive Diarrhea 10 or more stools per day is considered diarrhea The main concern associated with diarrhea is dehydration Treatment is primarily supportive Diabetes can occur in very young children Diabetic children can have great swings in their blood glucose levels Hypo and hyperglycemia possible Very young children can develop hypoglycemia without having diabetes Diabetic children increase their risk of hypoglycemia through overly strenuous exercise, too much insulin, and dehydration from illness Assessment Measure blood glucose with a glucometer Management Monitor the ABCs Obtain glucose In the conscious, alert patient, administer oral fluids with sugar or oral glucose Glucagon or Dextrose 25% © Ken Kerr Hyperglycemia may lead to dehydration and diabetic ketoacidosis Causes include: Eating too much food relative to injected insulin Missing an insulin injection Defective insulin pump Illness or stress Assessment Dehydration A blood sugar reading of greater than 200 mg/dL Management Monitor the ABCs and vital signs If unable to obtain glucose, treat as hypoglycemia Obtain intravenous access Administer an IV bolus of 20 mL/kg Accidental poisoning is a common childhood emergency It is the leading cause of preventable death in children Management Administer oxygen Contact medical direction and/or the poison control center Consider the need for activated charcoal Transport of Responsive Patient Be sure to take any pills, substances, and containers to the hospital Monitor the patient continuously Management of Non-Responsive Patient Ensure a patent airway Administer oxygen Be prepared to provide artificial ventilations Contact medical direction and/or the poison control center Transport Monitor the patient continuously Falls Motor vehicle crashes Car vs. pedestrian injuries Drowning and near drowning Penetrating injuries Burns Physical abuse Falls Most common type of traumatic injury Serious injury or death from accidental falls is relatively uncommon Motor Vehicle Accidents The leading cause of traumatic death in children Prevention strategies Car Particularly lethal form of trauma Stature pushes child beneath vehicle Two phases of injury vs. Pedestrian Injuries First phase occurs when the auto contacts the child Second phase occurs as the child contacts the ground or other objects Prevention strategies Drownings Third-leading cause of death in children between birth and 4 years of age Outcomes are better when the water is cold Prevention strategies Best time for drowning prevention programs is late spring and early summer Penetrating Injuries An increase in violent crime has resulted in an increasing number of children sustaining penetrating trauma Visual inspection of external injuries does not provide adequate evaluation of internal injuries Prevention strategies Burns Children can sustain both burn injuries and smoke inhalation in house fires Prevention strategies Physical Abuse Factors leading to child abuse Poverty, domestic disturbances, younger parents, substance abuse, and community violence Airway Control Maintain in-line stabilization in neutral position Administer 100% oxygen Maintain airway with suctioning and jawthrust © Scott Metcalfe Airway Control (cont.) Be prepared to assist ineffective respirations Intubate the child when the airway cannot be maintained Gastric tube Cricothyrotomy Immobilization Use appropriately sized pediatric immobilization equipment Keep the cervical spine in a neutral in-line position by placing padding from the shoulders to the hips Fluid Insert a large-bore intravenous catheter into a peripheral vein Management Do not delay transport to gain venous access Intraosseous access in children less than 6 years Initial fluid bolus of 20 mL/kg Pediatric Pediatric injuries are painful Commonly used analgesics Analgesia and Sedation Morphine and fentanyl Certain pediatric emergencies may benefit from sedation Traumatic Pediatric head injury classifications Brain Injury Mild —Glasgow coma score is 13–15 Moderate —Glasgow coma score is 9–12 Severe —Glasgow coma score is less than or equal to 8 Signs of increased intracranial pressure Elevated blood pressure Bradycardia Rapid, deep respirations progressing to slow, deep respirations Bulging fontanelle in infants Traumatic Signs of herniation Brain Injury Asymmetrical pupils Decorticate posturing Decerebrate posturing Consider hyperventilation if there is a deterioration in the child’s condition indicating herniation Administer Intubate high-flow, high-concentration oxygen if Glasgow coma score less than or equal to 8 Consider using intravenous or tracheal lidocaine prior to intubation Consider rapid sequence intubation (RSI) for children with a Glasgow coma score of less than or equal to 8 Head, Injuries to the head are the most common cause of death in pediatric trauma victims Face, and Neck Bicycle collisions, falls from trees, car-pedestrian collisions, sporting activities, abuse Diffuse injuries are common in children, while focal injuries are rare Facial injuries Chest Significant injury may occur without external evidence Tension Pneumothorax Injuries Diminished breath sounds over the affected lung Shift of the trachea to the opposite side A progressive decrease in ventilatory compliance Tamponade Hypotension may be only sign Injuries Blunt trauma to the abdomen can result in injury to the spleen or liver to the Abdomen Spleen is most frequent organ injured Signs and symptoms Splenic and hepatic injuries can cause lifethreatening internal hemorrhage Extremities Typically limited to fractures and lacerations Bend fractures, buckle fractures, and greenstick fractures Some types of growth plate fractures can lead to permanent disability Management Burns Most common type of burn injury encountered by EMS personnel is scalding Rule of Nines Burn Management Prompt management of the airway May need to use an endotracheal tube up to two sizes smaller Be sure to maintain body heat With electrical burns, suspect musculoskeletal injuries and perform spinal immobilization The sudden death of an infant during the first year of life from an illness of unknown etiology Occurs most frequently in the fall and winter months More common in males Prevalence Click here to view a video on sids. Infants should be placed supine Avoid placing infants in overheated environments Avoid overwrapping them with too many clothes or blankets Avoid smoking before and after pregnancy Avoid filling the crib with soft bedding Assessment Normal state of nutrition and hydration Skin may be mottled Occasionally blood-tinged, fluids in and around the mouth and nostrils Vomitus may be present Management Common Characteristics Child is seen as “special” and different from others Premature infants and twins Less than 5 years of age Physical and mental handicaps Special needs Perpetrators of Abuse or Neglect Can come from any geographic, religious, ethnic, racial, occupational, educational, or socioeconomic background Characteristics A parent or adult who seems capable of abuse A child in one of the high-risk categories The presence of a crisis in the family Child abuse can take several forms, including: Psychological abuse Physical abuse Sexual abuse Neglect (either physical or emotional) © Scott and White Hospital and Clinic Signs of abuse or neglect can be startling Information in the medical history may also raise the index of suspicion Management Appropriate treatment of injuries Protection of the child from further abuse Notification of proper authorities Common home-care devices Tracheostomy tubes Apnea monitors Home artificial ventilators Central intravenous lines Gastric feeding and gastrostomy tubes Shunts Avoid using the term disability in reference to the child’s special need Never assume that the patient cannot understand what you are saying Involve the parents, caregivers, or the patient, if appropriate, in treatment Treat the patient with a special need with the same respect as any other patient JumpSTART Pediatric MCI Triage Tool To optimize the primary triage of injured children in the MCI setting To enhance the effectiveness of resource allocation for all MCI victims To reduce the emotional burden on triage personnel who may have to make rapid life-or-death decisions about the injured Role of Paramedics in Pediatric Care General Approach to Pediatric Emergencies General Approach to Pediatric Assessment General Management of Pediatric Patients Specific Medical Emergencies Trauma Emergencies Sudden Infant Death Syndrome Child Abuse and Neglect Infants and Children with Special Needs Multiple Casualty Incidents Involving Children