Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
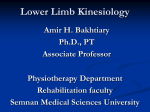
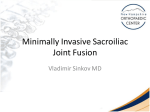
5 Scientific Proceedings Equine Programme Proximal Limb Lameness in the Horse Thomas K. Hughes, MA VetMB CertES(Orth) MRCVS, The Liphook Equine Hospital, Forest Mere, Liphook Hampshire. GU30 7JG, UK, [email protected] Principles Lameness associated with structures proximal to the elbow and stifle is uncommon but poses a particular challenge in terms of diagnosis. The accurate placement of local anesthetic solution within or around proximal limb structures can be difficult owing to a lack of practice and their deep location. The structures of the proximal limb are covered by muscle and closely associated with the thorax and pelvis limiting the number of radiographic views that it is possible to obtain. As a result, scintigraphic and, increasingly, ultrasonographic 308 | Abstracts European Veterinary Conference Voorjaarsdagen 2008 examination of affected structures is important in establishing a diagnosis. Treatment of many of the diseases in this region is symptomatic and revolves around corticosteroid injection or infiltration combined with a rest and rehabilitation program. The outcome in such cases varies with the disease identified. Intertubercular Bursa As it passes over the point of the shoulder, the biceps tendon divides into medial and lateral lobes that lie within the two grooves formed by the cranial parts of the greater and lesser tubercles and the intermediate tubercle of the humerus (1). The synovial intertubercular bursa (bicipital bursa) lying between the bilobate tendon and Scientific Proceedings Equine Programme Conditions affecting the proximal humerus that may improve to analgesia of the intertubercular bursa include both septic and non-septic bursitis, tendonitis of biceps brachii, osteitis of the humeral tubercles, osseus cyst-like lesions of the proximal humerus in communication with the bursa and fragmentation of the supraglenoid tubercle(2,5,6). Treatment of non-septic conditions revolves around intrathecal medication with corticosteroids and sodium hyaluronate combined with rest and in some cases bursoscopy. Septic bursitis requires directed lavage via bursoscopy. As a general rule, conditions that resolve without enlargement of the tendon, roughening of the surface of the humerus, or adhesion formation within the bursa have a fair prognosis for return to athletic function. Any condition that affects the smooth movement of the tendon through the grooves of the humerus will lead to chronic lameness(2). Figure 1. A - Lateral scintigraphic image of the right shoulder of a 25 year old Arab gelding showing marked increased radiopharmaceutical uptake over the scapulohumeral joint. B - Mediolateral radiograph of the right shoulder of the same horse as in A showing marked degeneration of the scapulohumeral joint. the humerus, facilitates movement of the tendon within the intertubercular groove. The biceps muscle flexes the elbow joint, tenses the fascia of the forearm and fixes the shoulder and elbow during weight bearing (1), therefore, abnormalities of the proximal tendon tend to lead to abnormalities of limb protraction during the swing phase of the stride as well as during weight bearing(2). Lameness may be sudden and severe, or mild and insidious in onset; lameness may only be observed when the horse is ridden in an outline or lunged with side reins. Abnormalities of the intertubercular bursa are rarely painful on palpation (2). An intrathecal injection of local anesthetic solution should improve lameness associated with the intertubercular bursa. Several techniques are described and the accuracy of the injection is improved by ultrasound guidance(3). Abnormalities of the proximal humerus may be apparent on scintigraphy and radiography but lesions affecting the biceps tendon or bursa are most apparent on ultrasonographic examination and the ultrasonographic anatomy of the bursa has been well described(4). Endoscopic evaluation of the bursa has been well described and allows inspection of the fibrocartilage covered surface of the intertubercular grooves of the humerus as well as the biceps tendon itself (5). Sacroiliac disease The sacroiliac joint lies between the wing of the ilium and the wing of the sacrum supported by extensive sacroiliac ligaments, the anatomy of which has been well described(7). The joint is flat, L-shaped and orientated at approximately 30 degrees to the horizontal plane. The sacral surface of the joint is covered by hyaline cartilage and the iliac surface is covered by fibrocartilage and, though the joint surface area is large, it contains only approximately 1ml of synovial fluid(8). Though there is evidence that inflammatory and degenerative disease can affect the joint and the supporting sacroiliac ligaments, the site from which pain originates in most horses (and humans) affected by lameness associated with the sacroiliac region is unknown(8,9,10). Lameness originating from the sacroiliac region may be acute and marked, mild and insidious in onset, or present as poor performance rather than overt lameness(10,11). If disease is acute then resentment may be seen to digital pressure over the lumbosacral region, the tuber sacrale or tuber coxae and any lameness present may be exacerbated by flexion or abduction tests(10,11). In more Figure 2. A transverse ultrasonographic image of the lateral lobe of the biceps brachii tendon of the right forelimb of a 13 year old TB gelding showing enlargement and heterogeneity of the tendon indicative of tendonitis. Abstracts European Veterinary Conference Voorjaarsdagen 2008 | 309 5 5 Scientific Proceedings Equine Programme chronic cases, overt lameness is frequently absent as are any localizing signs(9). number of cases of sacroiliac disease, has not, to the author’s knowledge, been published. As few localizing signs may be apparent on clinical examination, diagnostic analgesia is of great importance in diagnosing sacroiliac disease. The sacroiliac joint is inaccessible to standard injection techniques but in the majority of affected horses, local anesthetic infiltration of the sacroiliac region immediately adjacent to the joint will lead to an improvement in lameness(9). Several injection techniques have been reported(12). Care must be taken to avoid anesthesia of the sciatic nerve particularly if bilateral blocks are performed. A volume of local anesthetic greater than 10ml is likely to diffuse over a large area, confounding diagnosis and making unwanted neurological signs more likely(12). References 1. Sisson S. Equine mycology. In:Getty R. Eds. Sisson and Grossman’s The Anatomy of the Domestic Animals. Philadelphia: WB Saunders, 1975;376-453 2. Dyson SJ. The elbow, brachium and shoulder. In: Ross MW, Dyson SJ. Eds. Diagnosis and Management of Lameness in the Horse. Philadelphia: Saunders, 2003;399-416 3. Schumacher J, Livesey L, Brawner W, Taintor J, Pinto N. Comparison of 2 methods of centesis of the bursa of the biceps brachii tendon of horses. Equine vet J 2007;39:356-9 4. Crabill MR, Chaffin MK, Schmitz DG. Ultrasonographic morphology of the bicipital tendon and bursa in clinically normal quarter horses. Am J Vet Res 1995;56:5-10 5. McIlwraith CW, Nixon AJ, Wright IM, Boeing KJ. In: McIlwraith CW, Nixon AJ, Wright IM, Boeing KJ. Eds. Bursoscopy. Edinburgh: Elvsevier, 2005; 409-426 6. Coudry V, Allen AK, Denoix JM. Congenital abnormalities of the bicipital apparatus in four mature horses. Equine vet J 2005;37:272275 7. Sisson S. Equine syndesmology. In:Getty R. Eds. Sisson and Grossman’s The Anatomy of the Domestic Animals. Philadelphia: WB Saunders, 1975;349-375 8. Goff LM, Jeffcott LB, Jasiewicz J, McGowan CM. Structural and biomechanical aspects of equine sacroiliac joint function and their relationship to clinical disease. The Veterinary Journal 2007;doi:10.1016/j.tvjl.2007.03.005 9. Dyson S, Murray R. Pain associated with the sacroiliac joint region: a clinical study of 74 horses. Equine vet J 2003;35:240-245 10. Jeffcott LB. Disorders of the thoracolumbar spine of the horse - a survey of 443 cases. Equine vet J 1980;12:197-210 11. Haussler KK. Diagnosis and management of sacroiliac joint injuries. In: Ross MW, Dyson SJ. Eds. Diagnosis and Management of Lameness in the Horse. Philadelphia: Saunders, 2003;501-508 12. Engeli E, Haussler KK. Review of sacroiliac injection techniques. In: 50th Annual Convention of the American Association of Equine Practitioners, 2004, Denver, Colorado. Ithaca: International Veterinary Services (www.ivis.org) P1466.1204 13. Gorgas D, Kircher P, Doherr MG, Ueltschi G, Lang J. Radiographic technique and anatomy of the equine sacroiliac region. Vet radiol & ultrasound 2007;48:501-506 14. Erichsen C, Berger M, Eksell P. The scintigraphic anatomy of the equine sacroiliac joint. Vet radiol & ultrasound 2002;43:287-292 15. Tomlinson JE, Sage AM, Turner TA. Ultrasonographic abnormalities detected in the sacroiliac area in twenty cases of upper hindlimb lameness. Equine vet J 2003;35:48-54 16. Engeli E, Yeager A, Haussler KK. Use and limitations of ultrasonography in sacroiliac disease. In: 50th Annual Convention of the American Association of Equine Practitioners, 2004, Denver, Colorado. Ithaca: International Veterinary Services (www.ivis.org) P1468.1204 Diagnostic imaging of the sacroiliac region is a challenge. Radiography is only possible in small anesthetized horses(13). Scintigraphy is useful in identifying inflammation of the sacroiliac joints however, diagnosis should not be based on scintigraphic findings alone as there is significant overlap in the appearance of this region between normal horses, horses affected by sacroiliac disease and horses affected by other causes of hindlimb lameness(9,14). Ultrasonographic examination of the dorsal sacroliliac ligaments, tuber sacrale, iliac wings, and lumbosacral junction is possible but subtle lesions are difficult to identify and the clinical significance of any abnormal findings is presently unknown. Transrectal ultrasonography may be used to image the ventral aspect of the sacroiliac joints but the same limitations apply(15,16). Treatment of sacroiliac disease includes the local infiltration of corticosteroids combined with a rest and rehabilitation program(11). In human patients a specific physiotherapy program based on biomechanical findings is employed but as yet our lack of understanding of sacroiliac disease in horses means that such therapy is not available(8). Long-term follow-up on a meaningful 310 | Abstracts European Veterinary Conference Voorjaarsdagen 2008