Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
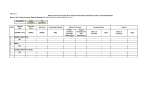
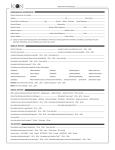
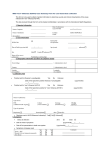
CORE CASE RECORD FORM for Severe Acute Respiratory Infection – 23/04/2013 Please complete sections 1-4 at admission. Complete sections 5-10 after discharge/death. Additional information can be recorded on the SUPPLEMENTARY DATA FORM. Daily information can be recorded on the DAILY RECORD FORM 1. Demographics This page completed: At admission During hospital stay After discharge Patient identification code: ___ ___ - ___ ___ ___ Date of birth (DD/MM/YYYY): ___ /___ /____ OR Estimated age _______ years Clinical centre:____________________________ Country: _________________ Form completed by:_______________________ First name initial: ____ Surname initial: ____ Sex: Male Female Ethnicity: ____________ _____________Unknown Weight (at admission): ______kg/lbs (circle) Height: _______cm/inches (circle) MUAC (if age<5yrs)________cm/inches (circle) Transferred from another facility? Yes No Unknown Admission date at this facility (DD/MM/YYYY): ___ /___/20___ If YES: Date admitted to other facility (DD/MM/YYYY):__ /__ /20____ Name of transferring facility:________________________ Suspected/confirmed infection: H7N9 Novel coronavirus H5N1 Other:_______________________________ History of close contact with a case of infection above? Yes, confirmed case Yes, suspected case No Has the patient travelled within 10 days of symptom onset? Yes No Unknown Unknown If YES, state location(s) below: Country:_________________________ City: __________________________ Return Date (DD/MM/YYYY): ____ /____ /20______ Country:_________________________ City: __________________________ Return Date (DD/MM/YYYY): ____ /____ /20______ In the previous 10 days, did the patient have contact with live animals? Yes No Unknown If YES, specify Animal ______________________ Type of contact:_________________________________________________ 2. Co-morbidities & Risk Factors (existing PRIOR TO ADMISSION & that are active problems) Congestive heart failure Dementia Chronic pulmonary disease (not asthma) Physician diagnosed asthma Rheumatologic disease Mild liver disease Moderate or severe liver disease Yes No Unknown Yes No Unknown Yes No Unknown Yes Yes Yes Yes No No No No Unknown Unknown Unknown Unknown (Charlson Index will be calculated at analysis) Diabetes with chronic complications Hemiplegia or paraplegia Renal disease Any malignancy including leukaemia & lymphoma Metastatic solid tumour AIDS / HIV Obese as defined by clinical staff History of recurrent fever prior to admission? Yes No Unknown Yes Yes Yes Yes No No No No Unknown Unknown Unknown Unknown Yes No Unknown Yes No Unknown Yes No Unknown Proven Malaria? Yes No Unknown Receiving immunosuppressants (including inhaled/oral corticosteroids) prior to admission? Yes No Unknown If YES: Name of immunosuppressant Dose and frequency unknown Pregnant? Yes No Unknown NA Post-partum? Yes No NA Route of administration Duration IV oral inhaled other unknown days weeks unknown Gestation at admission: ________weeks (round to nearest) Delivery date (DD/MM/YYYY) __ /___/20__ Outcome: Live birth Still birth Baby tested for infection above? Yes No Unknown If YES: Positive Negative Method: PCR Other: _________ Infants (<1 year old): birth weight if known: ______kg/lbs (circle) Term-born (≥37wk GA) Preterm(<37wk GA) Unknown Breastfed? Yes No Unknown If YES: Still breastfeeding Discontinued (at _______ weeks) Development appropriate for age? Yes No Unknown Vaccinations appropriate for age & country? Yes No Unknown Any other risk factor(s) considered relevant: 1 CORE CASE RECORD FORM for Severe Acute Respiratory Infection – 23/04/2013 3. Signs and Symptoms at Admission (please complete every line) Date of onset of earliest symptom (DD/MM/YYYY): / /20 OR if unknown, day-of-illness at admission: days Temperature:_________°C/°F (circle) HR: _______beats per minute RR:________ breaths per minute Systolic BP:_______mmHg Diastolic BP: _______mmHg Sternal capillary refill time >2secs? Yes No Unknown Intubated & ventilated? Yes No Unknown If intubated & ventilated: FiO2 ________ Unknown Not ventilated but receiving O2? Yes No Unknown O2 saturation: _____% On room air? Yes No Unknown Severe dehydration? Yes No Unknown Urine output: Oliguria (<1mL/kg/hr infants, <0.5mL/kg/hr children and adults ) Anuria (no urine output) Unknown Admission signs and symptoms (associated with this episode of acute illness) History of fever (>38°C) Yes No Unknown Lower chest wall indrawing Yes No Unknown Cough Yes No Unknown Headache Yes No Unknown with sputum production Yes No Unknown Altered consciousness/confusion Yes No Unknown bloody sputum/haemoptysis Yes No Unknown Seizures Yes No Unknown Sore throat Yes No Unknown Abdominal pain Yes No Unknown Runny nose (rhinorrhoea) Yes No Unknown Vomiting/nausea Yes No Unknown Ear ache Yes No Unknown Diarrhoea Yes No Unknown Wheezing Yes No Unknown Conjunctivitis Yes No Unknown Chest pain Yes No Unknown Skin rash Yes No Unknown Muscle aches (myalgia) Yes No Unknown Skin ulcers Yes No Unknown Joint pain (arthralgia) Yes No Unknown Lymphadenopathy Yes No Unknown Fatigue/malaise Yes No Unknown Bleeding Yes No Unknown Shortness of breath Yes No Unknown Biochemistry & Haematology 4. Admission Laboratory Results If bleeding, specify site: _____________________ Please circle the unit used for each parameter, where appropriate. Enter “NM” if not measured. No results available Date laboratory samples collected (DD/MM/YYYY): ____ /____ /20_____ Haemoglobin ______ g/L, g/dL Haematocrit ____________% WBC count ____________ x 109/L, x103/μL Platelets __________ x 109/L, x103/μL APTT/APRT (circle)__________ PT/INR________________ seconds ALT/SGPT _________ U/L Bilirubin _______μmol/L, mg/dL C-reactive protein ________ mg/L, nmol/L AST/SGOT _________ U/L Glucose _______mmol/L, mg/dL Erythrocyte Sed Rate ______mm/h Blood Urea Nitrogen _____ mmol/L, mg/dL LDH __________ U/L Creatinine _________ μmol/L, mg/dL Creatine kinase (CPK) ______U/L Lactate _______ mmol/L, mg/dL Blood Gas Date blood gas performed (DD/MM/YYYY): ____ /____ /20_____ Blood gas not performed Sample taken on: Room air Supplemental O2 Unknown If receiving O2, specify: _________% or ________l/min Sample type: Arterial Venous Capillary Unknown PO2 kPa, mmHg pH PCO2 kPa, mmHg Base excess mmol/L HCO3- mEq/L Lactate mmol/L, mg/dL Any other significant laboratory results: Patient identification code: ___ ___ - ___ ___ ___ Date of birth (DD/MM/YYYY): ___ /___ /____ 2 CORE CASE RECORD FORM for Severe Acute Respiratory Infection – 23/04/2013 5. Complications: At any time during hospitalisation did the patient experience (please complete every line): Viral pneumonitis Yes No Unknown Cardiac arrest Yes No Unknown Bacterial pneumonia Yes No Unknown Bacteraemia Yes No Unknown Acute lung injury / ARDS Yes No Unknown Coagulopathy or DIC Yes No Unknown Pneumothorax Yes No Unknown Anaemia Yes No Unknown Pleural effusion Yes No Unknown Rhabdomyolysis or myositis Yes No Unknown Bronchiolitis Yes No Unknown Acute renal injury/failure Yes No Unknown Meningitis/Encephalitis Yes No Unknown Gastrointestinal bleeding Yes No Unknown Seizure(s) Yes No Unknown Pancreatitis Yes No Unknown Stroke Yes No Unknown Hepatic dysfunction Yes No Unknown Congestive heart failure Yes No Unknown Hyperglycemia Yes No Unknown Endo/myo/peri-carditis Yes No Unknown Hypoglycemia Yes No Unknown Cardiac arrhythmia Yes No Unknown Other Yes No Unknown Cardiac ischaemia Yes No Unknown If Other, specify: 6. Treatment: At any time during hospitalisation, did the patient receive (please complete every line) If Daily Treatment was recorded on a DAILY RECORD FORM (Section 2), leave this section blank and check here Care on ICU/ITU/IMC/HDU? Yes No Unknown If YES, state the Date of admission to ICU/ITU/IMC/HDU (DD/MM/YYYY): ____ /____ /20____ Date Unknown If YES, state the Total number of days in ICU/ITU/IMC/HDU during this hospital stay: _______days Days Unknown Supplemental oxygen? Yes No Unknown …………………………………………………………….... If YES, duration: _________ days Non-invasive mechanical ventilation? (eg. BIPAP, CPAP) Yes No Unknown…………… If YES, duration: _________ days Invasive mechanical ventilation? Yes No Unknown ……………………….…………………… If YES, duration: _________ days Oscillatory Ventilation? Yes No Unknown ………………………..…………………………………... If YES, duration: _________ days Extracorporeal membrane oxygenation (ECMO) or interventional lung-assist therapy (iLA)? ECMO iLA None Unknown Not available……………………........................... If YES, duration: ________ days Renal replacement therapy (RRT) or dialysis? Yes No Unknown........................... If YES, duration: _________ days RRT required beyond discharge from hospital? Yes No Unknown Plasmapheresis? Yes No Unknown Inotropes/vasopressors? Yes No Unknown Oral rehydration only? Yes No Unknown Intravenous Immunoglobulin? Yes No Unknown Blood transfusion or products? Yes No Unknown OTHER intervention (please specify): Patient identification code: ___ ___ - ___ ___ ___ Date of birth (DD/MM/YYYY): ___ /___ /____ 3 CORE CASE RECORD FORM for Severe Acute Respiratory Infection – 23/04/2013 7. Pathogen Testing Only record results that are not recorded on a DAILY RECORD FORM (Section 4). Was pathogen testing performed? Yes No Unknown If YES, complete each line below. Date (DD/MM/YYYY) ____ /____ /20____ ____ /____ /20____ ____ /____ /20____ ____ /____ /20____ ____ /____ /20____ ____ /____ /20____ ____ /____ /20____ ____ /____ /20____ ____ /____ /20____ ____ /____ /20____ ____ /____ /20____ Sample Type Pathogen Result Method Nasal/NP swab Specify: _______________________ Positive Negative Unknown PCR other: _______________ Throat swab Specify: _______________________ Positive Negative Unknown PCR other: _______________ Combined nasal/NP + Throat swab Specify: _______________________ Positive Negative Unknown PCR other: _______________ Sputum Specify: _______________________ Positive Negative Unknown PCR other: _______________ BAL Specify: _______________________ Positive Negative Unknown PCR other: _______________ ETA Specify: _______________________ Positive Negative Unknown PCR other: _______________ Stool/Rectal swab Specify: _______________________ Positive Negative Unknown PCR other: _______________ Urine Specify: _______________________ Positive Negative Unknown PCR other: _______________ Blood Specify: _______________________ Positive Negative Unknown PCR other: _______________ Other (specify): __________________ Specify: _______________________ Positive Negative Unknown PCR other: _______________ Serology Specify: _______________________ Antibody Titre: ________________________________________ 8. Other Infections: Did the patient test positive for any other infection? Yes No Unknown If YES, specify. (DD/MM/YYYY) Sample Type (choose from list in #7 above) Type of Infection Pathogen ____ /____ /20____ Specify: ___________________________ Bacterial Viral Fungal Other:_________________ Specify: _____________________________ ____ /____ /20____ Specify: ___________________________ Bacterial Viral Fungal Other:_________________ Specify: _____________________________ ____ /____ /20____ Specify: ___________________________ Bacterial Viral Fungal Other:_________________ Specify: _____________________________ ____ /____ /20____ Specify: ___________________________ Bacterial Viral Fungal Other:_________________ Specify: _____________________________ Date of Detection 9. Medication: While hospitalised or at discharge, were any of the following administered? Yes No Unknown Antibiotics? Yes No Unknown Corticosteroids? Yes No Unknown Antifungals? Yes No Unknown Antivirals? Angiotensin converting enzyme inhibitors (ACE-Is) or angiotensin receptor blockers (ARBs)? Yes No Unknown Statins? Yes No Unknown If YES, was the patient taking statins prior to admission? Yes No Unknown Patient identification code: ___ ___ - ___ ___ ___ Date of birth (DD/MM/YYYY): ___ /___ /____ 4 CORE CASE RECORD FORM for Severe Acute Respiratory Infection – 23/04/2013 Medication: List ONLY ANTI-INFECTIVES and CORTICOSTEROIDS administered in hospital or at discharge. Name of medication Start date End date Route of administration Dose and frequency (generic name preferred) (DD/MM/YYYY) (DD/MM/YYYY) ____ /____ /________ On-going ____ /____ /20______ IV oral inhaled other unknown ____ /____ /________ On-going ____ /____ /20______ ____ /____ /________ On-going ____ /____ /20______ ____ /____ /________ On-going ____ /____ /20______ ____ /____ /________ On-going ____ /____ /20______ ____ /____ /________ On-going ____ /____ /20______ ____ /____ /________ On-going ____ /____ /20______ IV other IV other IV other IV other IV other IV other oral inhaled unknown oral inhaled unknown oral inhaled unknown oral inhaled unknown oral inhaled unknown oral inhaled unknown unknown unknown unknown unknown unknown unknown unknown 10. Outcome: Date outcome section completed (DD/MM/YYYY): ____ /____ /20______ Resolution of acute illness? Yes No Unknown If YES, date of resolution (DD/MM/YYYY): ____ /____ /20____ Unknown Still in hospital? Yes No Unknown Transferred to another facility? Yes No Unknown If transferred, date of transfer (DD/MM/YYYY): ____ /____ /20______ Name of new facility: _________________Unknown Discharged? Yes No Unknown If YES, state the date of discharge (DD/MM/YYYY): ____ /____ /20______ Ability to self-care at discharge versus prior to illness: Same as prior to illness Decreased Increased Unknown Respiratory support/treatment? Yes No Unknown Post-discharge treatment (if alive, check all that apply): Renal Treatment? Yes No Unknown Other Treatment? Yes No Unknown If YES, specify: Specify other treatment (multiple permitted): Diagnoses at discharge: 1. 2. 3. 4. 5. Died in hospital or palliative discharge? Yes No Unknown If YES, date of death (DD/MM/YYYY): ____ /____ /20______ Was an autopsy performed? Cause(s) of death: Yes No Unknown Key autopsy results: Patient identification code: ___ ___ - ___ ___ ___ Date of birth (DD/MM/YYYY): ___ /___ /____ 5 DAILY RECORD FORM for Severe Acute Respiratory Infection – 23/04/2013 Please complete daily during hospital admission. Any additional information can be added on paper to the SUPPLEMENTARY DATA FORM, Section 7–Any other additional information or directly to the electronic CRF on the CliRes database, Section 11-Additional Information. 1. Date and Demographics Date (DD/MM/YYYY): ____/____/20____ Study Day: [____][____][____] or 3 months 6 months Patient identification code: ___ ___ - ___ ___ ___ Date of birth (DD/MM/YYYY): ___ /___ /____ OR Estimated age ____ 2. Daily Treatment: (please complete every line daily during admission): Is the patient currently receiving, or has s/he received in the past 24 hours (since the last report from was completed): Care on ICU/ITU/IMC/HDU? Yes No Unknown Supplemental oxygen? Yes No Unknown Non-invasive mechanical ventilation? (eg. BIPAP, CPAP) Yes No Unknown Invasive mechanical ventilation? Yes No Unknown Oscillatory Ventilation? Yes No Unknown Extracorporeal membrane oxygenation (ECMO) or interventional lung-assist therapy (iLA)? ECMO iLA None Unknown Renal replacement therapy (RRT) or dialysis? Yes No Unknown Plasmapheresis? Yes No Unknown Inotropes/vasopressors? Yes No Unknown Oral rehydration only? Yes No Unknown Intravenous Immunoglobulin? Yes No Unknown Blood transfusion or products? Yes No Unknown OTHER intervention (please specify): 3. Daily Laboratory Results – for samples collected on the date listed above Biochemistry & Haematology Please circle the unit used for each parameter, where appropriate. Enter “NM” if not measured. No results available Haemoglobin ______ g/L, g/dL Haematocrit ____________% WBC count ____________ x 109/L, x103/μL Platelets __________ x 109/L, x103/μL APTT/APRT (circle)__________ PT/INR________________ seconds ALT/SGPT _________ U/L Bilirubin _______μmol/L, mg/dL C-reactive protein ________ mg/L, nmol/L AST/SGOT _________ U/L Glucose _______mmol/L, mg/dL Erythrocyte Sed Rate ______mm/h Blood Urea Nitrogen _____ mmol/L, mg/dL LDH __________ U/L Creatinine _________ μmol/L, mg/dL Creatine kinase (CPK) ______U/L Lactate _______ mmol/L, mg/dL Blood Gas Blood gas not performed Sample taken on: Room air Supplemental O2 Unknown If receiving O2, specify: _________% or ________l/min Sample type: Arterial Venous Capillary Unknown PO2 kPa, mmHg pH PCO2 kPa, mmHg Base excess Any other significant laboratory results: mmol/L HCO3- mEq/L Lactate mmol/L, mg/dL DAILY RECORD FORM for Severe Acute Respiratory Infection – 23/04/2013 4. Pathogen Testing Was pathogen testing performed on the date above? Yes No Unknown If YES, complete each line that applies. Sample Type Pathogen Result Method Nasal/NP swab Specify: _______________________ Positive Negative Unknown PCR other: ______________ Throat swab Specify: _______________________ Positive Negative Unknown PCR other: ______________ Combined nasal/NP + throat swab Specify: _______________________ Positive Negative Unknown PCR other: ______________ Sputum Specify: _______________________ Positive Negative Unknown PCR other: ______________ BAL Specify: _______________________ Positive Negative Unknown PCR other: ______________ ETA Specify: _______________________ Positive Negative Unknown PCR other: ______________ Stool/Rectal swab Specify: _______________________ Positive Negative Unknown PCR other: ______________ Urine Specify: _______________________ Positive Negative Unknown PCR other: ______________ Blood Specify: _______________________ Positive Negative Unknown PCR other: ______________ Other (specify): _______________________ Specify: _______________________ Positive Negative Unknown PCR other: ______________ Serology Specify: _______________________ Antibody Titre: _______________________________________________ Patient identification code: ___ ___ - ___ ___ ___ Date of birth (DD/MM/YYYY): ___ /___ /____ DAILY RECORD FORM for Severe Acute Respiratory Infection – 23/04/2013 [TIER3C] 5. Pharmacokinetics (PK) of Antimicrobials / Immunomodulatory Drugs Drug under study: Start date of drug prescription: Prescribed times of administration: Specify: _______________________ Date (DD/MM/YYYY) ____ /____ /20____ Specify All: ___________________________________________________________ *Precise* time of 1st PK blood draw today: Time (24 hour clock H H : M M) ___ ___ : ___ ___ *Precise* time of 2nd PK blood draw today: Time (24 hour clock H H : M M) ___ ___ : ___ ___ *Precise* time of 3rd PK blood draw today: Time (24 hour clock H H : M M) ___ ___ : ___ ___ Please record all doses of the drug given in the last 24hrs: Dose: Amount: ________ Units:_________ Amount: ________ Units:_________ Amount: ________ Units:_________ Amount: ________ Units:_________ Amount: ________ Units:_________ Amount: ________ Units:_________ Route of administration IV oral oral oral oral oral oral ___ ___ : ___ ___ ___ ___ : ___ ___ ___ ___ : ___ ___ ___ ___ : ___ ___ ___ ___ : ___ ___ ___ ___ : ___ ___ ___ ___ : ___ ___ ___ ___ : ___ ___ inhaled other:_______________ Patient identification code: ___ ___ - ___ ___ ___ ___ ___ : ___ ___ inhaled other:_______________ IV ___ ___ : ___ ___ inhaled other:_______________ IV ___ ___ : ___ ___ inhaled other:_______________ IV ___ ___ : ___ ___ inhaled other:_______________ IV *Precise* End Time (infusion only) (24 hour clock HH:MM) inhaled other:_______________ IV *Precise* Time Drug Given (if infusion: Start Time) (24 hour clock HH:MM) Date of birth (DD/MM/YYYY): ___ /___ /____ SUPPLEMENTARY DATA FORM for Severe Acute Respiratory Infection – 23/04/2013 Use this form to record information that does not fit the space provided in the CASE REPORT FORM. All information from the CASE REPORT FORM and SUPPLEMENTARY DATA FORM should be entered into the appropriate sections of the electronic CASE REPORT FORM. 1. Case Tracking Information Demographics should match those entered in the CRF Patient identification code: ___ ___ - ___ ___ ___ Date of birth (DD/MM/YYYY): ___ /___ /____ OR Estimated age ____ First name initial: ____ Surname initial: ____ 2. Has the patient travelled within 10 days of symptom onset – Additional Travel Locations This refers to Section 1-Demographics of the CRF. If more than two locations were visited, enter the details of additional locations below: Country:________________________ City: __________________________ Return Date (DD/MM/YYYY): ____ /____ /20______ Country:________________________ City: __________________________ Return Date (DD/MM/YYYY): ____ /____ /20______ Country:________________________ City: __________________________ Return Date (DD/MM/YYYY): ____ /____ /20______ 3. In the previous 10 days, did the patient have contact with live animals – Additional Animal Contacts This refers to Section 1-Demographics of the CRF. If there was more than one animal contact, enter the details of additional contacts below: Animal ______________________ Type of contact: Animal ______________________ Type of contact: Animal ______________________ Type of contact: Animal ______________________ Type of contact: 4. Receiving immunosuppressants prior to admission – Additional Immunosuppressants This refers to Section 2-Co-morbidities & Risk Factors of the CRF. If more than one immunosuppressant was being taken by the patient prior to admission, please enter the details of additional immunosuppresants below: Name of immunosuppressant Dose and frequency unknown unknown unknown unknown unknown Route of administration IV oral inhaled other unknown IV oral inhaled other unknown IV oral inhaled other unknown IV oral inhaled other unknown IV oral inhaled other unknown Duration days weeks unknown days weeks unknown days weeks unknown days weeks unknown days weeks unknown SUPPLEMENTARY DATA FORM for Severe Acute Respiratory Infection – 23/04/2013 5. Other Infections: Did the patient test positive for any other infection? – Additional infections This refers to Section 8-Other Infections of the CRF. If the patient was positive for more than one of any type of infection, please enter the details of additional infections below: Date of Detection (DD/MM/YYYY) ____ /____ /20____ Sample Type (choose from list in Core CRF #7) Specify: ___________________________ ____ /____ /20____ Specify: ___________________________ ____ /____ /20____ Specify: ___________________________ ____ /____ /20____ Specify: ___________________________ Type of Infection Bacterial Viral Fungal Other:________________ Bacterial Viral Fungal Other:________________ Bacterial Viral Fungal Other:________________ Bacterial Viral Fungal Other:________________ Pathogen Specify: ___________________________ Specify: ___________________________ Specify: ___________________________ Specify: ___________________________ 6. Anti-infective and corticosteroid medications received during hospitalisation or at discharge – Additional Medications This refers to Section 9-Medication of the CRF. If further space is required to list additional anti-infective or corticosteroid medications, please enter them below: List ONLY ANTI-INFECTIVES and CORTICOSTEROIDS administered in hospital or at discharge. Name of medication Start date End date Route of administration (DD/MM/YYYY) (DD/MM/YYYY) (generic name preferred) On-going IV oral inhaled ____ /____ /________ ____ /____ /20______ other unknown On-going IV oral inhaled ____ /____ /________ ____ /____ /20______ other unknown On-going IV oral inhaled ____ /____ /________ ____ /____ /20______ other unknown On-going IV oral inhaled ____ /____ /________ ____ /____ /20______ other unknown On-going IV oral inhaled ____ /____ /________ ____ /____ /20______ other unknown On-going IV oral inhaled ____ /____ /________ ____ /____ /20______ other unknown On-going IV oral inhaled ____ /____ /________ ____ /____ /20______ other unknown On-going IV oral inhaled ____ /____ /20______ ____ /____ /________ other unknown 7. Any other additional information Dose and frequency unknown unknown unknown unknown unknown unknown unknown Enter any other relevant information not captured in the CRF This information can be entered into Section 11-Additional Information of the electronic CRF on the CliRes database. Patient identification code: ___ ___ - ___ ___ ___ unknown Date of birth (DD/MM/YYYY): ___ /___ /____