Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Enfuvirtide (T-20)
Leroy Benons
Medical Advisor / HIV
Roche Products Ltd.
Contents of presentation
•
Overview of T-20 development
•
Summary of study results (Toro 1 and 2)
•
Resistance
•
Paediatric use
•
Side effects - injection site reactions
•
Access in the UK
•
•
When to use T-20
Development plans and T-1249
Overview of T-20 development
Discovery and Development of FUZEON
• Duke University
– Dani Bolognesei and colleagues
– Looking for targets for HIV vaccines
• HR2 had antiviral properties
• Established TRIMERIS
– independent Co, registered on the Stock Exchange
• Marketing of Fuzeon
– Roche / Trimeris - North America
– Roche - ROW
FUZEON - Product description
• The FIRST of a completely new class of ARV for the
treatment of HIV, the fusion inhibitors
• The first new class of ARV to be introduced since the
protease inhibitors (PIs) in 1995.
• No direct competitors until 2006, but indirect competition
from improvements in present / new agents
• 36 amino acid peptide (protein)
• Subcutaneous injection / BID / 90 mg
(abdomen, arm, thigh)
- 2ml vial
NH
FUZEON
O
HN
HO
The most complex molecule ever
chemically synthesized ?
O
H
N
OH
NH
NH2
O
HO
O
O
HN
O
OH
HN
H
N
O
NH
O
O
O
HO
HN
HN
H2 N
O
O
NH
NH HO
O
O
O
HN
HN
OH
O
O
O
NH
NH
HO
OH
HN
HN
O
OH
O
NH
NH
H2N
O
O
O
HN
HN
HO
O
O HO
O
O
H
N
H2 N
O
N
H
H
N
O
O
O
NHH2N
O
O
O
O
H2N
H
N
NH
N
NH2
H
N
O
N
H
O
O
O
NH
O
N
H
O
NH2
HO
O
NH2
ZIDOVUDINE
SAQUINAVIR
T-20
M.W. 267
M.W. 767
M.W. 4,492
O
NH
O
O
O
N
H
O
NH
HN
NH2
NH
O
NH
O
O
N
H
HN
Pharmaceuticals
O
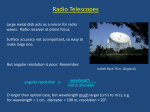
Manufacturing Issues
• 106 steps (chemical reactions - PIs= 8-12 steps)
• 18 secondary suppliers (19 sources of raw materials)
• Complex (synthetic peptide)
• 45 Kg raw materials - 1 Kg of T-20
• Total peptide production 30 kg (worldwide)
• Need to produce 40000-70000 kg T20 /year
to meet demand
Manufacturing Capacities of Peptide
Drugs
Product
Number of
Amino Acids
Annual
Production
Daily
Dose
Calcitonin
32
10 kg
0.5 mg
Leuprolide
9
20 kg
5 mg
Fuzeon
36
3,000 - 5,000 kg
180 mg
Fuzeon - manufacturing Scale
Annual
Batch Size
Production
(T-20)
Facility
# of
Intended Patients
per year
Use
2-5 Kg
0.2 - 0.3 Kg
Laboratory
Toxicology
Clinical
30 - 70
30 Kg
0.5 - 1 Kg
Pilot Plant
Laboratory
Clinical
400
80-90 Kg
3 - 4 Kg
Pilot Plant
Clinical
1100 - 1200
3000-5000 Kg
> 30 Kg
Facility
Commercial 40000 - 70000
Under Construction
Fusion Inhibiton
Fusion
Inhibitors
RNA
Nucleus
Protease
DNA
Reverse
T
transcriptase
Reverse transcriptase inhibitors
Protease inhibitors
Video on Mechanism of
Action of FUZEON
Dosing and Administration of FUZEON
Dosing and Administration of FUZEON
Dosage of FUZEON
• FUZEON is administered bid (usually the morning and evening) as
a subcutaneous injection.
• Each dose consists of 1.0 mL injection containing 90 mg of FUZEON
delivered with a 1 mL NMT Safety Syringe.
Preparation of FUZEON
• FUZEON is supplied as a lyophilized powder, which must be
reconstituted in water for injection.
• All of the necessary components needed for FUZEON injection are
supplied in a kit.
Dosing and Administration of FUZEON
The kit
The FUZEON kit contains the following five components:
•
•
•
•
•
60 vials of FUZEON
60 vials of water for injection
Alcohol pads
60 - 3 mL NMT Safety Syringe
60 - 1 mL NMT Safety Syringe
Dosing and Administration of FUZEON
• The 3 mL NMT Safety Syringe is used for sterile water; the 1 mL NMT
Safety Syringe is used for injecting the FUZEON solution
• FUZEON typically requires 10 to 20 minutes to dissolve in sterile
water, but may take up to 45 minutes
• The injection site should be rotated and should not include the area
around the navel, the belt line, or any area where there is an ongoing
injection site reaction
Convenience Box
358 x 177 x 202.8mm
Convenience Box
"top view"
Convenience Box
"overview"
Efficacy of FUZEON - The Clinical Trials
T-20 clinical synopsis
Phase I/II
Phase II
Phase III
TRI-001
Proof of concept
n = 17
TRI-003
Outpatient dosage form
n = 73
T20-204
Paediatric study
n = 14
T20-205
Chronic safety
n = 70
T20-206
Dose comparison
n = 71
T20-208
Formulation improvements
n = 46
T20-301
Pivotal
n =491
T20-302
Pivotal
n=506
T20-305
Safety study
T20-310
Paediatric study n = 48
Up to = 450
TORO Studies
What is an ‘Individualised / Optimized
background’?
A combination of antiretrovirals, carefully selected to
provide the maximum antiretroviral activity amongst the
available options, used in conjunction with a new agent as
part of an antiretroviral regimen.
Available options
Drug A
Drug B
Drug C
Drug D
Individualized
background
New agent
SELECTED FOR
MAXIMUM ACTIVITY
Drug A
Drug C
Drug E
Individualised / Optimized Background
• Regimens are individualized through selection of
maximally active drugs determined by prior treatment
history and, wherever possible, HIV resistance testing
Treatment
history
Individualized background
SELECTED FOR MAXIMUM ACTIVITY
Resistance
test
information
• Other considerations may include the use of
pharmacokinetic enhancement and, for patients
with few remaining options, attempts to limit HIV
replicative capacity
TORO-2 Study
Pivotal Studies: 24 week primary analyses
TORO 1: (US, Canada, Mexico, Brazil) &
TORO 2: (Europe, Australia)
• Population:
– Prior experience to 1 NRTI, 1 NNRTI
and 1-2 PIs
– 3-6 months experience on each class
or documented viral resistance
– HIV RNA 5000 copies/mL
• Design:
– Open Label, Randomized Multi-Center, International
• Treatments (Planned N=525 each, randomized
1:2):
– Optimized Background [OB, 3-5 antiretrovirals (ARVs)
based on history, viral GT/PT] (n=175)
– Fuzeon (ENF, T-20: 90 mg sc bid) + OB, (n=350)
TORO 2:
Demographics and Baseline Characteristics
ENF+OB
(N=335)
OB
(N=169)
Total
(N=504)
Baseline RNA
(median, log10)
5.1
5.1
5.1
Baseline CD4+ cell count
(median, cells/mm3)
98
102
98
Prior ARVs (median)
12
12
12
Years ARV use (median)
7.4
7.4
7.4
250 (75%)
138 (82%)
388 (77%)
1.4
1.4
1.4
Prior ADEs (N, %)
PSS at entry (mean)
PSS = Number of drugs in OB regimen to which virus was phenotypically
sensitive
Gender, race and age were balanced across treatments
TORO 2: Summary of AEs Related to any
drug in Original Regimen prior to switch
(> 5% through Wk 24, excluding ISRs)
Adverse Event
FUZEON + OB
(N=335)
OB
(N=169)
Total Patients with at least one related AE
241 (71.5%)
114 (67.5%)
Diarrhea
67 (19.9%)
34 (20.1%)
Nausea
38 (11.3%)
25 (14.8%)
Fatigue
29 (8.6%)
11 (6.5%)
Vomiting
25 (7.4%)
14 (8.3%)
Dermatitis
26 (7.7%)
7 (4.1%)
Asthenia
24 (7.1%)
7 (4.1%)
Headache
20 (5.9%)
13 (7.7%)
Insomnia
19 (5.6%)
10 (5.9%)
Pyrexia
19 (5.6%)
9 (5.3%)
Depression
18 (5.3%)
4 (2.4%)
Pruritus
17 (5.0%)
5 (3.0%)
Peripheral Neuropathy
17 (5.0%)
9 (5.3%)
TORO 2:
Primary Study Endpoint
HIV-1 RNA Log Change from BL at Week 24
Change from BL
(log10 copies/ml)
0
FUZEON
+ OB
OB alone
N=335
N=169
-0.65
-1
-1.43
-2
(Delta=0.78,
P<0.0001)
Least Squared Means Log Change from Baseline - Intent-to-Treat Population (LOCF)
TORO 2:
Secondary Analysis
Response at Week 24 (ITT, DC=Failure)
100
% of Patients
FUZEON + OB
OB
80
P<0.0001
60
43
P<0.0001
40
21
20
0
1 log decrease
from BL
28
14
< 400
copies/mL
2 visits required to confirm viral load response
P=0.009
9
12
5.3
< 50
copies/mL
TORO 2:Secondary Analysis
Mean CD4+ Cell Count Change from
BL at Week 24
Change from BL
(Cells/mm3)
100
P=0.023
65
50
0
38
FUZEON
+ OB
OB alone
Least Squared Means Change from Baseline Intent-to-Treat Population (LOCF)
TORO 2:
Conclusions
•
Safety:
– ISRs occur in almost all patients (only treatment limiting in
3%)
– Other AEs comparable across treatments
•
Primary study endpoint:
– plasma HIV-1 RNA analysis
statistically significant favouring the Fuzeon arm
•
Secondary endpoints:
– Responder analyses (1 log drop, <400, <50 c/mL)
statistically significant favouring the Fuzeon arm
– CD4 cell count change from baseline
statistically significant favouring the Fuzeon arm
TORO 1 / TORO 2 Conclusions
• Patient Populations:
– BL RNA (median): 5.2 - 5.1 log10 copies/mL
– CD4 (median): 80 - 98 cells/mm3
– PSS (mean) 1.7 - 1.4
• Primary Efficacy ENF + OB vs. OB:
– TORO 1: -1.7 vs. -0.76; Delta = 0.93; p<0.0001
– TORO 2: -1.43 vs. -0.65; Delta = 0.78; p<0.0001
– Sensitivity analyses and analysis of secondary virologic and immunologic
endpoints consistently demonstrated benefit of ENF+OB over OB
• Safety
– ISRs occur in almost all patients; treatment limiting in 3%
– Other AEs comparable across treatments
TORO 1 / 2:
Conclusions
• Fuzeon, the most clinically advanced fusion
inhibitor, was studied in two separate multinational
studies in a total of approximately 1000 heavily
pretreated patients.
– Injection site reactions were the most common AE;
treatment limiting in only 3%
– Significant benefit in primary and secondary virological
endpoints as compared to OB alone.
– Significant immunologic benefit as compared to OB
alone.
• Results consistent across both studies
TORO 2
(Sub-group Analyses)
TORO 2: Demographic subpopulations:
Subgroup analysis of mean change from baseline in
log10 HIV-1 RNA at week 24 (ITT population)
Gender
Change from baseline
(log10 copies/mL)
Male
Race
Female
White
Age
Non-White
< 40
years
=40
years
0
N=8
N=148
-1
N=109
N=161
N=21
*
*
*
N=60
*
N=146
N=292
-2
N=43
N=316
N=189
N=19
*p < 0.05
OB
ENF + OB
Least Squared Means Log Change from Baseline (LOCF) - Intent-to-Treat Population
TORO 2: Baseline viral load and CD4:
Subgroup analysis of mean change from baseline in
log10 HIV-1 RNA at week 24 (ITT population)
< 40,000
copies/mL
=40,000
copies/mL
< 100 CD4
cells/mm3
=100 CD4
cells/mm3
Change from baseline
(log10 copies/mL)
0
N=39
-1
N=130
*
*
N=81
N=169
*
N=85
*
N=258
N=77
N=166
-2
*p < 0.05
OB
ENF + OB
Least Squared Means Log Change from Baseline (LOCF) - Intent-to-Treat Population
TORO 2: Baseline GSS score:
Subgroup analysis of mean change from baseline in
log10 HIV-1 RNA at week 24 (ITT population)
GSS 0
GSS 1
GSS 2
GSS 3
GSS 4
5
=
GSS
Change from baseline
(log10 copies/mL)
0
N=31
N=60
*
N=50
N=95
N=45
*
N=104
-2
N=5
N=4
*
-1
N=33
*
N=4
N=49
N=13
-3
*p < 0.05
OB
ENF + OB
Least Squared Means Log Change from Baseline (LOCF) - Intent-to-Treat Population
TORO 2: Baseline PSS score:
Subgroup analysis of mean change from baseline in
log10 HIV-1 RNA at week 24 (ITT population)
PSS 0
PSS 1
PSS 2
PSS 3
PSS 4
5
=
PSS
Change from baseline
(log10 copies/mL)
0
N=59
*
-1
N=37
*
N=101
N=4
N=39
N=7
*
N=82
N=22
N=69
-2
*p < 0.05
N=43
N=5
N=21
OB
ENF + OB
Least Squared Means Log Change from Baseline (LOCF) - Intent-to-Treat Population
TORO 2: Multiple regression analyses:
Change from baseline to week 24 in log10 HIV-1 RNA
data (LOCF): ITT
Predictor
Estimate
95% C.I.
p-value
-0.80
-1.01, -0.60
<0.0001
Baseline VL (per log10 copies/mL) -0.30
-0.47, -0.12
0.0009
Baseline CD4 count
(per 100 cells/mm3)
-0.21
-0.28, -0.14
<0.0001
PSS§
-0.19
-0.26, -0.11
<0.0001
Total adherence score* (per 10%)
-0.11
-0.19, -0.04
0.0038
Prior LPV/r experience
0.86
0.65, 1.07
<0.0001
Treatment with ENF
§ Replacing PSS with GSS gives similar results
* Adherence based on 4 day recall
TORO 2: Conclusions
• Primary and secondary categorical analyses all favoured
enfuvirtide and were consistent across TORO 1 and
TORO 2
• Enfuvirtide demonstrated benefit across subgroups
evaluated
• The enfuvirtide effect on viral load was seen across a
range of PSS and GSS scores
TORO 2: Conclusions
Predictors of response included:
• Treatment with enfuvirtide
• Baseline viral load
• Baseline CD4 count
• PSS/GSS
• Adherence
• Prior LPV/r use
(predicted poorer response)
Activities of Daily Living Survey
TORO 1 and 2
Patient acceptance of subcutaneous
self-injections (Activities of Daily Living Survey)
• SIS survey (18-item psychometric questionnaire)
– psychometric properties evaluated and found to be reliable in
assessing of self-injecting in trials
• n=661 (Toro 1 + 2)
• Evaluated patients experience with preparing and injecting
• Administered at 8 and 24 weeks (prior to seeing clinician)
Toro 1 & 2 - Activities of Daily Living
(SIS Survey)
Giving yourself injections
68.1%
Keeping medication refrigerated
81.4%
Dissolving medication in water
74.4%
92.4%
Disposing of needles and vials
0
20
40
60
80
Patient Responses (%)
Very easy or Easy
Neutral
Green et al., Poster, HIV6, Glasgow
Difficult
Very difficult
100
Toro 1 & 2 - Activities of Daily Living
77.8%
Participating in recreational
activities/sports
70.1%
Maintaining privacy about your health
84.2%
Socializing (or interacting)
with family or friends
77.5%
Being intimate or having sexual
relations with a partner
68.6%
Traveling away from home
89.2%
Getting around locally
84.7%
Working at a job or attending school
Sleeping
90.4%
0
20
40
60
80
100
Patient Responses (%)
Not at all or a little
Moderately
Quite a bit
Extremely
Patient acceptance of SC self-injections
Conclusions
• In the Phase III trials, TORO 1 and TORO 2, patient acceptance of
self-injections of FUZEON remained high over the 24 week treatment
period.
• Most patients reported that self-injections were easy to administer
and that injections had ‘little’ or ‘no impact’ on their daily routines.
• This should allow good treatment compliance, helping to ensure
successful therapy.
• Additional analyses are planned once the 48-week data is available.
Injection Site Reactions (ISR)
Picture of Injecting Site Reactions (ISR)
ISR and related variables
• Severity of local ISRs is not dose related in the range used in
adults.
• Grade 3 & 4 ISRs were comparable in patients with and
without fat redistribution.
• Trend towards more frequent grade 3 signs/symptoms with
low BMI.
• Incidence of Grade 3/4 ISRs was not increased in patients
with a higher CD4 cell count.
ISRs - Drug-demographic interactions
• Demographic Subpopulations:
– Gender (male or female)
– Race (white or non-white)
– Age (<40yrs or 40yrs)
– Gp41 Antibody
• No apparent differences seen for subpopulations on:
– Incidence
– Most common symptom & signs
– Severity of symptom & signs
– Severity with duration of treatment
– Duration of lesions
– No. of lesions at any given visit
ISR discontinuation rate remains low
& similar from week 24 to safety update
cut-off (week 48)
• Low ISR discontinuation rate and high adherence to
treatment despite high overall incidence of ISR
• Week 24: 3% of patients discontinued due to ISRs
• Safety update: 4% of patients discontinued due to ISRs
(majority patients reached Week 48)
Possible reasons for low discontinuation
rate and high adherence to treatment
despite high incidence of ISRs
• Motivated patients: heavily experienced
– Median duration of prior therapy: 7 years
– Median number of ARVs: 12
– Mean PSS: 1.6
• ISRs mostly mild to moderate in intensity
• While rate of ISR remain stable overtime, no apparent
increase in severity overtime
ENF is the predominant factor for
eliciting ISRs
• Animal studies suggest some role of vehicle, but a major
contribution of enfuvirtide.
• Cannot be evaluated clinically
(no placebo-control)
• Conclusions limited by:
– repeated injections in animals vs. “single” injections
in humans
– placebo is not ideally matched (hypo-osmotic)
– uncertain relevance of animal findings to humans.
Pathological characterization of injection
site changes in animals
• Gross (visible) changes:
– swelling, hardening, discoloration
• Microscopic changes:
– mixed inflammatory infiltrate (primarily macrophages,
lymphocytes, eosinophils)
– nonspecific changes of hemorrhage, edema
– repeated injections of high concentrations resulted in
granulomatous reaction (foreign-body type?)
No data currently available for guidance
with medical management of local ISRs
• Anecdotal reports:
– massaging injection site or applying ice helpful in adult patients
– proper injection technique reduce severity/frequency
• Pediatric patients: optional use of topical anesthetic
– however, effect of topical anesthetic use not prospectively studied
• Three ongoing studies may assist in determining appropriate
measures to prevent and/or treat ISRs
– Intervention study (T20-305): massage, topical steroids, heat, self injected
vs. partner injected
– Clinical, histological, and immunochemical characteristics of ISRs at
various times after the injection of ENF
(T20-306)
– Injection site pathology study (NV16471)
FUZEON and RESISTANCE
Resistance testing
Drug resistant HIV can be identified by two in vitro methods;
• Genotyping and
• Phenotyping
Genotypic Resistance - 1
• Fuzeon
– a completely new class of ARV
– a unique MoA
• Mutations in the target enzymes of protease and the
reverse transcriptase cause no reduction in
susceptibility to T-20
• Baseline resistance to T-20 is rare.
Genotypic resistance - 2
• In vitro resistance:
– HIV- 1 isolates with substitutions in amino acids (aa) 36–
38 of the gp41 ectodomain correlated with varying levels
of reduced FUZEON susceptibility in HIV site-directed
mutants.
• In vivo resistance:
– Treatment- emergent substitutions in aa 36– 45 of gp41
HR 1 region have been observed in viruses from patients
receiving FUZEON in Phase II and Phase III clinical
studies. The substitutions observed in decreasing
frequency were at amino acid positions 38, 43, 36, 40, 42
and 45.
Genotypic resistance - 3
• In Phase 11 studies (T20-205, 206 and 208) the most
common substitutions in plasma virus on treatment were as
follows;
– V38A (n=18)
– G36D (n=15)
– G36S (n=11)
– N43D (n=10)
– N42T (n=5)
• At the time of protocol defined virological failure, viruses from
a total of 31/40 (78%) patients showed substitutions in gp41
aa 36-45.
Resistance testing - Phenotype
Antiviral EC50 values are dependent
upon the assay type/protocol
DATA FOR WT (PRE-TREATMENT) HIV
• Using a cMAGI cell assay the geo mean EC50 was
0.016 g/ml (n=130)
• Using a JC53-BL cell assay mean EC50 was
0.16 g/ml (n=35) (Derdeyn et al)
• Using a PhenoSense Assay the mean EC50 was
0.26 g/ml (n=612)
• All are valid assays
Enfuvirtide susceptibility of isolates
from Phase II clinical studies
60%
Percent of Patients
GM+2SD=0.218 µg/mL
Geometric Mean (GM) EC50 = 0.020 µg/mL
40%
20%
0%
0.000
0.001
0.003
0.010
0.032
0.100
Patient Virus EC50 (µg/mL)
The relationship between in vitro susceptibility and in vivo
activity has not been established
0.316
1.000
T20-301+T20-302
Histogram of Baseline EC50 (µg/mL)
GM+2SD=1.956 µg/mL
Percent of Patients
40
Geometric Mean (GM) EC50 = 0.259 µg/mL
20
0
0.01 0.02 0.03 0.07 0.16 0.34 0.73 1.59 3.45 7.48
EC50 (µg/mL)
Patients carrying the least sensitive virus
pre-treatment respond similarly to FUZEON
treatment
• Patients carrying viruses with an EC50 value > (mean +
2SD) respond comparably to the total treated
population in terms of reduction in viral load (HIV
plasma RNA)
Fold-change in ENF susceptibility at
virological failure through week 24
T20-301
T20-302
Overall
5 (5.4%)
14 (12.4%)
19 (9.2%)
4 to 10- fold
11 (11.8%)
17 (15.0%)
28 (13.6%)
Greater than
10- fold
77 (82.8%)
82 (72.6%)
159 (77.2%)
< 4-fold
PHENOTYPIC CHANGES IN VIRUSES EMERGING WITH
SINGLE T-20 RESISTANCE MUTATIONS: PHASE 2 STUDIES
Poster 22 : Seville, 2002
PHENOTYPIC CHANGES IN VIRUSES EMERGING WITH
DOUBLE T-20 RESISTANCE MUTATIONS: PHASE 2 STUDIES
Poster 22; Seville 2002
FUZEON treatment emergent substitutions
in gp41 aa 36-45 in virological failure
patients
• Of the patients who met virological failure, 94% carried virus
with ENF-associated substitutions
• The most common substitutions were
– V38A, N43D, Q40H, G36D
• These mutations are associated with diminished
– ENF sensitivity in vitro
– replicative capacity in vitro
The high incidence of resistance to
FUZEON at VF reflects the lack of sensitivity
to the OB regimen
• 43.5% of patients had a PSS of 0
• 38.5% of patients had a PSS of 1 or 2
• A large proportion of patients were essentially treated with
ENF as monotherapy
Failure rates for FUZEON+OB vs. OB only
through week 24
Score at
Baseline
No.
Pts
FUZEON + OB
No.
Failed (%)
No.
Pts
OB
No.
Failed (%)
PSS
0
1-2
3-4
5
191
288
144
21
131 (68.6%)
116 (40.3%)
40 (27.8%)
7 (33.3%)
99
148
73
10
94 (94.9%)
103 (69.6%)
33 (45.2%)
4 (40.0%)
GSS
0
1-2
3-4
5
112
368
152
18
82 (73.2%)
159 (43.2%)
49 (32.2%)
6 (33.3%)
53
188
82
8
52 (98.1%)
133 (70.7%)
46 (56.1%)
4 (50.0%)
Viruses with aa36-45 resistance mutations
are less fit than wild-type
• Wild-type virus outgrows mutants in in vitro grow competition
• Mutants are outgrown by wild-type in vivo on cessation of
FUZEON therapy
FUZEON-resistance mutations are not
seen in pre-treatment HIV
• There is a low incidence of variants in aa 36-45 of pretreatment HIV gp41
– these are not resistance mutations in in vitro assays
• Patients carrying viruses with pre-treatment variants or wildtype respond equally to FUZEON treatment in terms of VF
• Viruses carrying the most common pre-treatment variant,
N42S, are slightly more sensitive to FUZEON in vitro
Resistance summary
• Unique virus target and mode of action
• No cross resistance with approved ARVs
• Active against
– Multidrug-resistant isolates
– CCR5, CXCR4, and dual tropic isolates
• Pre-existing resistance to ENF is rare
• Specific substitutions in gp41 aa 36-45
– are associated with reduced susceptibility to
FUZEON in vitro
– are associated with diminished in vitro
replicative capacity
Paediatrics
Paediatric Question
•
Roche acknowledges that there is a medical need for
alternative ART also in children.
– To summarise the available clinical data in children and
provide an outline of ongoing and planned paediatric
trials
– To discuss if a dose recommendation for children of 6
years and older can be supported by available data
– To discuss the need for a specific paediatric formulation
or presentation that would facilitate flexible and accurate
dosing of enfuvirtide in children
Current and future paediatric clinical program
Study
Population
Treatment
Enrolled*/
Planned
T20-204/
P1005**
Treatment experienced Part A (single dose, IV
Part A 12/12
HIV RNA>10,000 c/ml
& SC): 15, 30 , 60 mg/m2 Part B 14/12
Age 3-12 yrs
Part B (chronic dosing):
30, 60 mg/m2 SC BID
96 weeks/
completed
T20-310/
NV16056
Treatment experienced 2.0 mg/kg up to 90 mg
deliverable SC BID
HIV RNA5,000 c/ml
Age 3-16 yrs
48 weeks+
extension/
ongoing
40/48
* As of March 2003
**Conducted by Pediatric AIDS Clinical Trials Group (PACTG)
Duration/
Status
Current and future paediatric clinical program
Study
Population
Treatment
Enrolled*/
Planned
T20-204/
P1005**
Treatment experienced Part A (single dose, IV
Part A 12/12
HIV RNA>10,000 c/ml
& SC): 15, 30 , 60 mg/m2 Part B 14/12
Age 3-12 yrs
Part B (chronic dosing):
30, 60 mg/m2 SC BID
96 weeks/
completed
T20-310/
NV16056
Treatment experienced 2.0 mg/kg up to 90 mg
deliverable SC BID
HIV RNA5,000 c/ml
Age 3-16 yrs
40/48
48 weeks+
extension/
ongoing
T20-305
Treatment experienced 2.0 mg/kg up 90 mg
HIV RNA >10,000 c/ml deliverable SC BID
Age 6-16 yrs
9/50
Infant/children
study
Treatment experienced 2.0 mg/kg
HIV RNA5,000 c/ml
Age 6 mos - 6 yrs
0/16-20
Until
commercial
availability/
ongoing
2 weeks/
planned
* As of March 2003
**Conducted by Pediatric AIDS Clinical Trials Group (PACTG)
Duration/
Status
Paediatric data currently available
(Nov 02 safety update)
• Patient
– 47 paediatric pts included
• 35 patients aged 6–16 yrs
• Exposure
– 35 paediatric patients 6–16 years of age with duration of ENF
exposure ranging from 1 dose to 48 weeks
• 30 patients 6yrs with exposure to at least 24 weeks
– 10 patients 6yrs with exposure to at least 48 weeks
• Pharmacokinetic
– 32 paediatric patients 3–16 years
• 20 patients 6–16 years
Dose recommendation for patients 6 – 16
yrs: safety (2mg/kg BID dose)
• Based on a limited number of patients:
– ENF was well tolerated with comparable safety profile
to adults
– Most common AEs were mild-to-moderate injection site
reactions (ISRs)
– Two related SAEs
• Cellulitis and ISR
Dose recommendation for patients 6 – 16 yrs:
(2mg/kg BID dose)
Cross-study comparison
100
90
% of Patients
80
71
T20-206 N=16
Paediatric P1005 N=12
Double-class
experienced
Double- or tripleclass experienced
70
60
50
38
40
43
25
30
21
20
10
ND
0
1 log decrease
from BL
<400 copies/ml
<50 copies/ml
Alternative dosage forms
• Current adult formulation allows for dosing in children and is
being used in ongoing paediatric trials
• Roche is exploring the potential for alternative dosage forms
which may also allow flexible dosing in children
Conclusion
• Given the need for alternative ART in children, enfuvirtide at a
2mg/kg BID dose in children 6 to 16 years of age is
supported by the available clinical data
Access in the UK
Early Access Programme (IPS)
• EAP - small and short lived
• From November 2002 - March 03 ( extended to May
2003)
• Europe and RoW - 600 patient slots
– allocated based on HIV prevalence (WHO)
– 43 patient slots in UK (37 used to date)
• EAP with free drug (no hidden costs)
EAP (IPS): Global criteria
• Male and female HIV-1 infected adults or adolescents
( 16 years of age)
• CD4 lymphocyte count 100 cells/mm3 and HIV-1 RNA
viral load > 10,000 copies/mL while on HAART (latest
available measurement must be within the last 90 days)
• Also:
– Patients should have prior documented genotypic and /
or phenotypic resistance and /or;
– At least 6 months exposure to all 3 current classes of
antiretrovirals and /or
– Treatment limiting toxicity
FUZEON
IPS- Status (22nd April 03) - Location of patients
• London (20)
• Royal London (1)
• UCL (3)
• St Mary’s (3)
•
•
•
•
Chelsea & Westminster (7)
London and Barts (3)
St Thomas’ (1)
Kings (1)
• Outside London (17)
Regulatory Timelines Update
• Status
– USA
• Approval received March 03
• EU
– Expedited review
– Positive Opinion (20 March 03)
– Approval expected end-April 03
• UK
– Stock receipt (4-6 weeks after approval)
– Launch end-May 03
When to use enfuvirtide ?
When to use enfuvirtide ?
• Not too early
– after failure of NNRTI and PI (3rd line)
– patient with tolerability problems to Nukes or PIs
– optimal response with 2 other active drugs
• Not too late
– need active agents to construct OB
– avoid functional monotherapy
Development plans and T-1249
T-1249
Designed 39-amino acid synthetic peptide
Binds to a slightly different sequence of gp41 than ENF
NH2
FP
HR1
cc
HR2
tm
COOH
ENF
T-1249
Maintains antiretroviral activity against most isolates with
reduced susceptibility to ENF in vitro
Demonstrates potent short term antiviral activity in most
patients failing an ENF-containing regimen
Further studies will evaluate efficacy and safety in this
patient population
T-1249 Demonstrates Potent Antiviral Activity
over 10 Day Dosing in Most Patients who Have
Failed a Regimen Containing Enfuvirtide (ENF):
Planned Interim Analysis of T1249-102,
a Phase I/II Study
GD Miralles1*, J Lalezari2, N Bellos3, G Richmond4,
Y Zhang1, H Murchison1, B Spence1, C Raskino5 and
R DeMasi1 for the T1249-102 Study Group
1Trimeris,
Inc., Durham, 2Quest Research, San Francisco, CA;
3Southwest ID, Dallas, TX; 4Ft. Lauderdale, FL; 5Roche, Welwyn, U.K.
T1249-102
Objective
To evaluate the safety and short term activity of
T-1249 on ENF resistant isolates in vivo
Design
Ten day add on therapy where T-1249 at a dose of 192
mg/daily replaces ENF in a failing regimen
Entry Criteria: Stable ENF-containing ARV regimen for the
past 8 weeks. Two most recent viral loads of 5,000 and
500,000 copies/mL (with protocol defined VF)
Patients are permitted to dose 192 mg QD or 96 mg BID
Sample Size of 50 Patients
T1249-102
Study Design
Stable antiretroviral background
ENF with VL 5,000
T-1249 192 mg
x 10 days
Stop ENF
BL (Day 1) Day 5
Start T-1249
Day 8
Day 11
Viral Load taken at BL and each Study visit
GT and PT performed at BL (Day 1) and at Day 11
T1249-102
Baseline Patient Characteristics:
Planned Interim analysis
Treated Population (25 patients)
22 (88%) Males; 3 (12%) Females; Mean age 42 years
Median exposure to ENF: 70.1 weeks (range 38.1 - 176.0)
Median Time from ENF Failure (n=25): 59.9 weeks
(range 28.3-136.0)
Median baseline HIV RNA: 5.0 log10 copies/mL
(range 3.8-5.5)
6 (24%) subjects enrolled from ENF Phase II studies
19 (76%) subjects enrolled from TORO 1
T1249-102
Patient Disposition
All 25 patients completed 10-day dosing
After completion of T-1249 dosing, one patient with advanced COPD
died on Day 11 from pneumonia resulting in respiratory failure
T1249-102
Baseline Resistance Testing
Planned Interim Analysis
At baseline, 23 patients had both GT and PT, 1 patient had
GT only, and 1 patient had neither. 24/25 (96%) had
Baseline GT or PT results (ITT population).
All 24 patients demonstrated GT substitutions associated
with ENF-resistance.
The GM change in ENF susceptibility between BL in TORO
1 and BL in T1249-102 was 77-fold compared with a 2-fold
GM change for T-1249 susceptibility (n=15)
T1249-102
Treatment-Emergent
Serious Adverse Events (SAE)
Five SAEs reported in three patients
3 (12% SAP*)
Patient #
Preferred Term
N (%)
Related
T-1249
200764
Alanine aminotransferase (ALT)
increased
Aspartate aminotransferase (AST)
increased
Bronchitis acute NOS
Pneumonia
Respiratory failure
1 (4%)
No
1 (4%)
No
1 (4%)
1 (4%)
1 (4%)
No
No
No
202730
200148
Possible Allergic Reaction: AE of rash (Grade 2) associated with fever
observed in one patient after completion of dosing (night of Day 11).
Resolved without treatment in 48 hours.
* Safety Population (SAP): n=25
T1249-102
Incidence TE Grade 3 & 4 Laboratory Toxicities
(reported by n=3 patients {12%})
Laboratory Events
Chemistry
ALT
AST
Calcium
Creatinine
Glucose
Hematology
ABS Neutrophils
Grade 3
N (%)
Grade 4
N (%)
Total
N (%)
0
0
0
1 (4%)*
1 (4%)*
1 (4%)
1 (4%)
1 (4%)*
0
0
1 (4%)
1 (4%)
1 (4%)
1 (4%)
1 (4%)
1 (4%)
0
1 (4%)
* All reported from the same patient prior to demise with multiorgan failure
Change From BL
T1249-102
Log10 HIV RNA Mean and Median
Change from Baseline (ITT)
-0.25
Day 11
Median -1.12
(CI -1.50; -0.83)
-0.75
-1.25
-1.75
0
N=24
5
22
Study Day
8
11
24
24
Percent of patients with 1 log10 drop
in HIV RNA according to length of ENF
therapy after VF
100
90
80
70
Percent of
patients with 60
1 log drop
50
40
30
20
10
0
Median drop -1.6
Median drop -0.94
7/7
8/17
24-48 wk > 48 wk
T1249-102
Percent of patients with 1.0 log Decline (ITT*)
Percent of Patients
100%
80%
63%
60%
40%
50%
29%
20%
0%
5
8
Study Day
* Missing=Failure
11
T1249-102
Conclusions Interim analysis
First 25 patients
T-1249 demonstrates potent short term antiviral activity in
most patients failing an ENF-containing regimen.
The time on ENF following virological failure inversely
correlates with short-term antiviral responses to T-1249
The safety and efficacy of T-1249 remains to be tested in
clinical trials during chronic administration.
The results from this study demonstrate that fusion inhibitors
constitute an expanding class of antiretroviral agents with the
potential to be sequenced
T1249
Timelines
• Phase II trials will start in late 2003
• Followed by Phase 111 trials
•
Hope to launch in 2006
BACK -UPS
Mechanism of Action
Representation of the HIV binding process
Working model of HIV fusion
Representation of gp41 showing
the HR1 and HR2 region
Working model of HIV fusion inhibition
How do we interpret resistance tests?
One possible approach:
PSS: Phenotypic
sensitivity score
•
•
•
•
GSS: Genotypic
sensitivity score
The number of drugs in a
regimen to which a
patient’s virus is
considered
sensitive by phenotyping
The number of drugs in a
regimen to which a
patient’s virus is
considered
sensitive by genotyping
Phenotypic resistance
determined by reference to
‘cut-off’ thresholds of
fold-resistance
Genotypic resistance
determined by mutation
analysis algorithms
Resistance does not always have a binary classification (ie: ‘fully sensitive’ or ‘fully
resistant’). PSS and GSS may not be integer
New regimens are selected to give maximal PSS or GSS
A PSS or GSS of at least 2 may be needed for durable suppression
A PSS or GSS >2 is preferable if possible
Phenotypic cut-offs used in
resistance testing
TECHNICAL
• Based on assay
reproducibility
• Not drug-specific
• Being superceded
by biological and
clinical cut-offs
BIOLOGICAL
• Based on upper
limit of
susceptibility
range observed in
panel of wild-type
isolates
• Drug specific
CLINICAL
• Based on direct
fold change/
response
correlation from
clinical studies
A test may give only a partial answer
to drug sensitivity
Low fitness of resistant
strains
Patient stops
drugs
Cause resistance to
‘ARCHIVE’
RECHALLENGE RE-EMERGENCE
THEREFORE
Resistance tests must be performed on
therapy
Prior resistance test results and/or full
clinical history must be factored in to new
drug selection
Reversion to
wild type
BUT
• Undetectable minority
populations remain
• HIV sanctuary sites in
body compartments
• Latently infected
CD4 cells
TORO- 1 Study
Fuzeon (ENF, T-20) in Combination with an
Optimized Background (OB) Regimen vs. OB
Alone in Patients with Prior Experience or
Resistance to Each of the Three Classes of
Approved Antiretrovirals (ARVs) in North America
and Brazil (TORO 1)
K. Henry, J. Lalezari, M. O'Hearn, B. Trottier,
J. Montaner, P. Piliero, S. Walmsley, J. Chung,
L. Fang, J. Delehanty, M. Salgo on behalf of the
TORO 1 study group.
TORO 1: Demographics and
Baseline Characteristics
ENF+OB
(N=326)
OB
(N=165)
Total
(N=491)
Baseline RNA
(median, log10)
5.2
5.2
5.2
Baseline CD4+ cell count
(median, cells/mm3)
76
87
80
Prior ARVs (median)
12
12
12
Years ARV use (median)
7.0
7.1
7.0
273 (84%)
148 (90%)
421 (86%)
1.7
1.8
1.7
Prior ADEs (N, %)
PSS at entry (mean)
PSS = Number of drugs in OB regimen to which virus was phenotypically
sensitive
Gender, race and age were balanced across treatments
TORO 1:
Patient Disposition (ITT)
ENF+OB
(N=326)
OB
(N=165)
Remain on Original
Randomized Treatment
Non-VF
VF
(N=190) (N=136)
Total
(N=326)
No. Discontinued
20
17
37
(11.3%)
Safety
AE/Lab
11
5
16 (4.9%)
6
3
9 (2.8%)
2
1
0
0
1
0
4
4
3
1
4
4
ISR
Non-Safety
Admin/Other
Failure to return
Insuff ther resp.
Refused Trt
Remain on Original
Randomized Treatment
VF, No
Non- Switch
VF
(N=25)
(N=59)
8
10
5
5
Total
(N=84)
(N=81)
18
(21.4%)
6
(7.4%)
10 (11.9%)
2 (2.5%)
1 (1.2%)
Not applicable
0
1
0
2
VF, Switch OB
to ENF + OB
1
0
2
2
Discontinuations: ENF + OB 11.3%, OB 21.4%
For further details see poster LbOr19b
1
1
2
4
0
0
1
2
TORO 1: Summary of AEs Related to any drug on
Original treatment prior to switch
(> 5% on ENF + OB, through Wk 24, Excluding ISRs)
Adverse Event
ENF + OB
(N=326)
OB
(N=165)
Total Patients with at least one related AE
253 (77.6%)
123 (74.5%)
Diarrhea
79 (24.2%)
63 (38.2%)
Nausea
72 (22.1%)
48 (29.1%)
Fatigue
64 (19.6%)
28 (17.0%)
Peripheral Neuropathy
36 (11.0%)
9 (5.5%)
Insomnia
32 (9.8%)
10 (6.1%)
Headache
29 (8.9%)
15 (9.1%)
Appetite Decreased
26 (8.0%)
5 (3.0%)
Vomiting
25 (7.7%)
21 (12.7%)
Dizziness (Excl. Vertigo)
24 (7.4%)
7 (4.2%)
Weight Decreased
18 (5.5%)
6 (3.6%)
Flatulence
17 (5.2%)
13 (7.9%)
TORO 1: Primary Study Endpoint
HIV-1 RNA Log Change from Baseline at Week 24
Change from BL
(log10 copies/ml)
0
Fuzeon
+ OB
OB alone
N=326
N=165
-0.76
-1
-2
-1.70
(Delta=0.93,
P<0.0001)
Least Squared Means Log Change from Baseline - Intent-to-Treat Population (LOCF)
TORO 1: Secondary Analysis
Response at Week 24 (ITT, DC=Failure)
100
% of Patients
Fuzeon + OB
80
60
40
OB
P<0.0001
P<0.0001
52
37
P=0.0002
29
16
20
20
7.3
0
1 log decrease
from BL
< 400
copies/mL
2 visits required to confirm viral load response
< 50
copies/mL
TORO 1: Time to Virological Failure
1-Prob (Virological Failure)
1
0.75
P<0.0001
ENF+OB
0.5
OB
0.25
Time to protocol defined
VF starts at week 6*
0
0
4
8
12
16
Study Week
* For definition of virologic failure, see Back-up slide
20
24
TORO 1:
CD4+ Cell Count Change from
Baseline at Week 24
Change from BL
(Cells/mm3)
100
76
50
0
P=0.0001
32
Fuzeon
+ OB
OB alone
Least Squared Means Change from Baseline Intent-to-Treat Population (LOCF)
TORO 1:
Conclusions
•
Safety:
– ISRs occur in almost all patients (only treatment limiting in
3%)
– Other AEs comparable across treatments
•
Primary study endpoint:
– plasma HIV-1 RNA analysis
statistically significant favoring the Fuzeon arm
•
Secondary endpoints:
– Responder analyses (1 log drop, <400, <50 c/mL)
statistically significant favoring the Fuzeon arm
– CD4 cell count change from baseline
statistically significant favoring the Fuzeon arm
TORO 2:
Patient Disposition (ITT)
ENF+OB
(N=335)
Remain on Original
Randomized Treatment
No. Discontinued
Safety
AE/Lab/Death
ISR
Non-Safety
Admin/Other
Insuff ther resp.
Refused Trt
Non-VF
VF
(N=170) (N=165)
23
34
OB
(N=169)
Remain on Original
Randomized Treatment
VF, Switch,
OB to ENF +
OB
Total
(N=335)
57
(17.0%)
Non-VF
(N=39)
2
VF
(N=16)
6
Total
(N=55)
8
(14.7%)
(N=114)
9
(7.9%)
1
1
2 (3.6%)
4 (3.5%)
12
11
23 (6.9%)
6
5
11 (3.3%)
2
1
2
1
13
4
3
14
6
3 (2.6%)
Not Applicable
0
0
1
0
4
1
Discontinuations: ENF + OB 17.0%, OB 14.7%
For further details see poster LbOr19a
0
4
2
0
2
0
ISR Severity rating scale in the T20-208 Study
Parameter
Erythema:
diameter (mm)
of skin redness
at the site
of injection
Induration:
diameter (mm)
of palpable
hardness of
the skin at the
site of injection
Pain:
subjective
report
Grade 1
(Mild)
Grade 2
(Moderate)
Grade 3
(Severe)
Grade 4*
(Potentially
Life-threatening)
<25 mm
(size of a
quarter)
>25 mm
but <50 mm
>50 mm
but <85 mm
>85
Slight
present but <25
>25 mm
but <50 mm
>50 mm
Mild tenderness
at injection site
Moderate pain
without limitation
of usual activities
Severe pain
requiring analgesics
and/or limiting usual
Severe pain
requiring
narcotic
analgesics
or not responding
to analgesics
*Grade 4 local reactions require a clinic visit within 12 to 24 hours of the event