Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
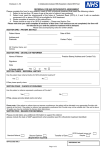
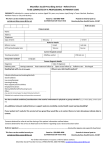
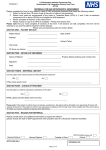
Referral to WLMHT Gender Identity Clinic All sections of the form are compulsory and must be completed to ensure the referral is accepted. Date of Referral _ _ /_ _ / 20 _ _ Patient Details Name D.O.B NHS Number Sex assigned at Birth please circle: Postcode Address Patient Telephone Patient Mobile Interpreter Required ☐ Yes ☐ No If required, what language Can patient attend clinic independently ☐ Yes ☐ No If no, please give more information GP Doctor Details GP Name GP Practice Name GP Address GP Telephone GP Fax GP E-mail Referrers Details only applicable if the referrer is not the patient’s GP Referrer Name Referrer Job Title Referrer Address Referrer Telephone Referrer Fax Referrer E-mail _ _ /_ _/ Female 19 _ _ Male The Referrer (if the referrer is not the GP) may need to liaise with the patient’s GP to obtain this information Please provide us with a detailed reason for referral Medical history including computerised printout Please provide us with any mental health history which you are aware of, including any known substance misuse or risk history Up-to-date mental state examination Please provide us with a background family history Any other agencies involved Any other relevant information or comments Physical Health AssessmentThe Referrer (if the referrer is not the GP) may need to liaise with the patient’s GP to obtain this nformation Date of Physical Health Assessment at GP NHS Number: Height (metres): Weight (kg): Waist (cm) : BMI: Blood Pressure: Heart Rate: Polycystic ovarian syndrome ☐ Yes ☐ NO ☐ N/A Physical intersex condition ☐ Yes ☐ Do you? Details how many, how much, units etc. Do you smoke? Do you drink alcohol? Do you take recreational drugs? ☐ Yes ☐ Yes ☐ Yes ☐ ☐ ☐ NO NO NO NO Do you have or have you had any of the following? Details if answered Yes to any of the questions Epilepsy ☐ Yes ☐ NO Pulmonary Embolus/ Deep Vein Thrombosis (Blood clot) ☐ Yes ☐ NO Heart disease or Stroke ☐ Yes ☐ Yes ☐ Yes ☐ ☐ ☐ ☐ Yes ☐ ☐ Yes ☐ Yes ☐ Yes ☐ Yes ☐ ☐ ☐ ☐ Breast Cancer High Blood Pressure Diabetes (Please indicate) Gynaecological issues Other Medical Conditions Past Surgical Operations Allergies/ Other NO NO NO Type 1 NO Insulin Type 2 Tablets Diet NO NO NO NO Does your patient’s family history have any of the following? Details if answered Yes to any of the questions Pulmonary Embolus/Deep Vein Thrombosis/blood clots ☐ Yes ☐ NO Heart disease or Stroke ☐ Yes ☐ NO Please write which area i.e. bowel, breast etc. Any type of cancer? ☐ Yes ☐ NO Diabetes ☐ Yes ☐ NO Type 1 Insulin Type 2 Tablets Diet On a scale of 1 to 10 (10 being good 1 being poor) rate Your energy, Drive (your ‘get up and go’ feeling) And libido (sex drive): Energy 1 2 3 4 5 6 7 8 9 10 Drive 1 2 3 4 5 6 7 8 9 10 Libido 1 2 3 4 5 6 7 8 9 10 Blood tests Please ensure the following blood tests are completed and a computerised printout is sent with this referral: ☐ FBC ☐ TFT’s ☐ U&E’s ☐ SHBG ☐ LFT/Gamma GT ☐ FSH ☐ Serum Calcium ☐ LH ☐ B12 & Foliate ☐ Vitamin D ☐ Cholesterol ☐ Prolactin ☐ Triglycerides ☐ Testosterone ☐ Fasting ☐ Dihydrotestosterone and Oestradiol ☐ Blood Sugar Have you previously taken any hormones at all? If so please list below: Name Dose Details i.e. from Internet, GP/ Other and duration of taking. Please list any current medications (not just hormones): Name Dose Prescribed? If yes, by whom? Duration ‘In common with all people who risk losing their fertility through scheduled medical treatment, people with gender dysphoria are entitled to gamete storage (sperm or egg storage) and if patient's agree at the point of referral that they want to arrange this, it would be prudent for an early referral to be made to local fertility services in order that subsequent hormone treatment is not avoidably delayed’. Any additional comments (if applicable): Please note the requirements regarding GPs’ commitment to hormone treatment when making the referral. The Gender Identity Clinic will recommend and advise on hormone treatment and monitoring as appropriate Referrer’s Job Title Referrer’s Signature: Please return this form to: Referral and Funding Team WLMHT Gender Identity Clinic 179-183 Fulham Palace Road London W6 8QZ Tel: Fax: Email: Website: 0208 483 2801 0208 483 2873 [email protected] www.gic.wlmht.nhs.uk Date: