Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Autism therapies wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Moral treatment wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
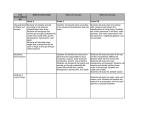
Name of Speaker Lucene Wisniewski, PhD, FAED Affiliation Case Western Reserve University & The Emily Program Title of Keynote Address: DBT in the Treatment of Eating Disorder: How, Why and With Whom? Dialectic Behavior Therapy (DBT) was originally designed to treat chronically suicidal patients diagnosed with borderline personality disorder. Recent empirical evidence suggests that DBT may be an effective treatment for some eating disorder (ED) patients. This keynote address will review the research support, rationale and existing models for using DBT to treat patients suffering from disordered eating. emilyprogram.com Lucene Wisniewski, PhD, FAED Clinical Integrity Officer The Emily Program Adjunct Assistant Professor Case Western Reserve University DBT in the Treatment of Eating Disorders: What? Why ? For Whom? HOW? What Is DBT? • Marsha Linehan, PhD • Originally - suicidal patients – many suicidal patients diagnosed with borderline personality disorder • Combined CBT with mindfulness/acceptance techniques • Promising results emilyprogram.com What Is DBT?: BPD Reorganized • • • • • BPD is a Disorder of Dysregulation: Emotional Interpersonal Self Behavioral Cognitive emilyprogram.com Research on DBT: randomized controlled trials • Fewer and less severe incidents of suicidal behavior • Stay in therapy longer • Fewer inpatient psychiatric days • Cost effective emilyprogram.com What is DBT? the unique assumptions emilyprogram.com DBT Assumptions: Patients • Patients are doing the best they can. • Patients want to improve. • Patients must learn new behaviors in all relevant contexts. • Patients cannot fail in DBT. emilyprogram.com DBT Assumptions: Patients • Patients may not have caused all of their own problems, but they have to solve them anyway. • Patients need to do better, try harder, and be more motivated to change. • For many patients, their current lives are unbearable. emilyprogram.com DBT Assumptions: Therapy • The most caring thing a therapist can do is help patients change in ways that bring them closer to their own ultimate goals. • Clarity, precision, and compassion are of the utmost importance in the conduct of DBT. • The therapeutic relationship is a real relationship between equals. emilyprogram.com DBT Assumptions: Therapy • Behavioral principles are universal, affecting therapists no less than patients. • Therapists need support. • DBT therapists can fail. • DBT can fail even when therapists do not. emilyprogram.com • WHAT is the Structure of DBT? emilyprogram.com : Four Primary Modes of Treatment • Individual psychotherapy • Group skills training • Telephone skills coaching • Team consultation emilyprogram.com DBT Structure • Individual therapy –Reinforce skills –Motivation –Year long commitment emilyprogram.com DBT Structure • Weekly skills group –Emotion regulation –Interpersonal effectiveness –Distress tolerance –Mindfulness emilyprogram.com DBT Structure • Telephone consultation – In vivo skill coaching – Skill generalization – Decrease crisis behavior – Decrease sense of conflict, alienation, distance with therapist. emilyprogram.com DBT Structure • Consultation Team – Help therapist morale – Adherence to the treatment – Adherence to consultation team agreements (esp. assumptions) emilyprogram.com WHAT are the Goals of DBT? emilyprogram.com Standard DBT Goals • To assist patients to move themselves to a “Live Worth Living” • Decrease behaviors that interfere with – Living (e.g. suicide and self-harm) – Therapy – Quality of Life • Increase behavioral skills emilyprogram.com Stages of Treatment: Dialectical Syntheses Pre-treatment ►Commitment and Agreement Stage 1: Severe Behavioral Dyscontrol ► Behavioral Control Stage 2: Quiet Desperation ► Emotional Experiencing Stage 3: Problems in Living ► Ordinary Happiness/Unhappiness Stage 4: Incompleteness ► Capacity for Joy and Freedom emilyprogram.com WHY use DBT with ED patients? emilyprogram.com WHY is New Treatment Needed for EDs? • CBT and IPT: – Multiple controlled clinical trials indicate that these treatments are effective for BN and BED. emilyprogram.com WHY is New Treatment Needed? • However • Treatment adherence problems • Not successful for everyone • Data for AN is limited emilyprogram.com WHY not just CBT? • CBT designed for unwanted thoughts • Binge/purge behaviors are usually unwanted • Restrictive behaviors – Positive emotional response – Positive social response – Sense of satisfaction and purpose – Cannot assume the client and therapist share the same outcome goals- weight gain, stopping behaviors emilyprogram.com WHY DBT? • ED patients have impaired emotion regulation • ED patients have specific problem that can be targeted behaviors – – – – Restriction Binge Eating Purging Compulsive exercise • emilyprogram.com WHY DBT? • Treatment for the treators –ED patients can elicit strong emotions • Strategies to reduce recidivism – may be especially useful with AN • Targets difficult to treat populations emilyprogram.com • FOR WHOM is DBT Indicated ? emilyprogram.com DBT for mild BN/BED • DBT skills for BN or BED – Safer, et al., 2012; Safer, et al., 2010; – Safer, et al., 2001a, 2001b; – Telch, et al., 2001; Telch et al., 2000. Good results for BED: NICE, 2004 & Need more research! For BN emilyprogram.com But what about multi-diagostic patients? emilyprogram.com WK? • Axis I – Anorexia Nervosa • Binge/purge • Treatment History – Major Depressive Disorder, in • Axis II – BPD • Axis III – Hypokalemia – Prolonged QTC – Bradycardia – Hypothyroidism – Eating Disorder • Inpatient partial remission • Residential • Day Treatment • Intensive Outpatient • Individual Therapy – Suidality/Depression • Inpatient • Day Treatment • Individual Therapy – CBT emilyprogram.com Scenario One: The pt enters standard ED treatment – Pros: staff is expertly trained to treat ED behaviors – Cons: Staff not trained/tx protocols not designed to manage comorbid suicidal/self-injurious behavior and significant therapy interfering behaviors Outcome: (1) Multi-diagnostic pts leave tx prematurely, feel like failures, little therapeutic change (2) staff feel frustrated, ineffective, burned out. emilyprogram.com Scenario Two: The pt enters standard DBT for BPD tx – Pros: staff is expertly trained to treat BPD and therapy interfering behaviors – Cons: Staff are typically not trained to manage ED behaviors & related medical complications. Outcome: (1) Multi-diagnostic pts may reduce therapy interfering behaviors but the ED symptoms typically remain strong (2) staff feel frustrated, ineffective, burned out with ongoing ED symptoms emilyprogram.com DBT for Complex ED • Full DBT for BPD with BN or BED – Chen et al., 2008 • Full DBT for ED with BPD or previous treatment failure – Kröger et al., 2010 – Palmer et al., 2003 – Wisniewski et al., 2009 – Federici & Wisniewski, 2013 emilyprogram.com When to Consider DBT for Complex/Co-Morbid ED’s? • Traditional ED treatment has failed • Presentation: significant emotional dysregulation • Behaviors are treatment interfering • Co-morbid BPD emilyprogram.com HOW to provide DBT for Complex/COmorbid ED emilyprogram.com emilyprogram.com • Comprehensive DBT For Complex EDs: • Combines CB techniques shown • to be the cornerstone • of empirically founded treatments for EDs with DBT theory and practice. emilyprogram.com What does it mean to provide Comprehensive DBT? • Individual DBT psychotherapy • Group DBT skills training • Telephone skills coaching • DBT Team consultation emilyprogram.com Comprehensive DBT for Complex EDs CBT for EDs DBT Strategies Diary cards Acceptance Meal planning BCA Focus on emotion regulation In Vivo Food exposure Change Skills Phone Coaching Weight monitoring Exposure Non-judgmental stance ED psychoeduction Cog Mod Dialectical stance emilyprogram.com Think about this…. emilyprogram.com Target 1 Life threatening behaviors • Suicide/Non-suicidal self injury • ED behaviors included when imminently life threatening emilyprogram.com Imminently Life Threatening Conditions in ED Clients • Bradycardia • Heart rate (e.g., < 40) generally warrants hospitalization (Sachs et al, 2016) • Prolonged QTc • >470 needs daily ECG (Sachs et al, 2016) • >500 requires hospitalization emilyprogram.com Imminently Life Threatening Conditions in ED Clients • Electrolyte Abnormalities (Mehler & Walsh, 2016) – Hypokalemia (serum potassium <3.6) – Hyponatremia (serum sodium <120-125) – Metabolic alkalosis (bicarbonate >28) • Chronic Ipecac Abuse • Mallory-Weiss Tear • Diabetic Keto-Acidosis emilyprogram.com Target II • Therapy Interfering Behaviors –Behaviors that interfere with receiving therapy –Behaviors that burn out therapists emilyprogram.com Behaviors that Interfere with Receiving Therapy • Non-attentive behaviors – Cancel appointment/drop out – Getting admitted to hospital – Inadequate intake resulting in inattention during session • Non-collaborative behaviors – – – – Inability/refusal to work in therapy Lying Manipulating weight Refusal to work on eating “in vivo” • Noncompliant behaviors – Not completing diary cards or homework – Not bringing in food for therapeutic meal emilyprogram.com Behaviors that Burn Out Therapists • Pushing the therapist’s personal limits – Phoning too much – Continuing to lose weight and refusing to collaborate on weight maintenance or gain • Behaviors that push the organizational limits – Not waiting for therapist in the waiting room – Vomiting in the lobby restroom • Behaviors that decrease the therapist’s motivation – Slow progress – Lying about intake emilyprogram.com Therapy-Interfering Behaviors for Specific to those with ED • • • • • • • • Exercising against medical advice Restricting intake before treatment Involuntary vomiting Misrepresenting weight (e.g., water loading) Refusing to be weighed Weight loss when underweight Hiding food Omitting symptoms emilyprogram.com Quality of Life Interfering Behaviors • ED behaviors when they are NOT life threatening nor therapy interfering. • Any other quality of life interfering behaviors that are not imminently life threatening –e.g., unemployment, promiscuity, prostitution, relationship issues,substance abuse etc. emilyprogram.com DBT Group Skills Training • Weekly 90 min group • Takes 1 year to cover all skills twice • Four Modules – Mindfulness – Distress Tolerance – Emotion Regulation – Interpersonal Effectiveness emilyprogram.com The function and context of an ED behavior will determine in which target it falls e.g., restriction prior to a therapy session emilyprogram.com Increase Behavioral Skills Core Mindfulness Skills Interpersonal Effectiveness Skills Emotion Regulation Skills Distress Tolerance Skills Treats Identify Confusion & Emptiness Identify emotions, hunger, fullness non-judgmentally Treats Interpersonal Chaos & Fears of Abandonment Inability to identify and gratify needs; ineffective assertiveness re: food Treats Labile Affect & Inappropriate Anger Vulnerability to emotion mind re: food Treats Impulsivity & Suicidal Behavior Eating disorder behaviors emilyprogram.com DBT Phone Coaching • Provide contact BEFORE a problem behavior occurs – Decrease suicide crisis behaviors – Decrease ED behaviors – Increase generalization of DBT skills – Decrease of conflict & alienation with therapist. • NOT THERAPY! Limbrunner, Ben-Porath & Wisniewski, (2011). Cognitive and Behavioral Practice 18, 186-195. Wisniewski & Ben-Porath, (2005). European Eating Disorders Review, 13, 344-350. emilyprogram.com DBT Consultation Team • Therapy for the therapists – Weekly for 90 minutes • Helps with adherence to model • Decrease burnout • Non-judgmental stance emilyprogram.com Data from our program • Case Series Data (n = 7) • Significant improvements with respect to the frequency of: – – – – – – – Suicidal urges/behaviors Self-injurious behaviors ED symptoms Weight gain and nutritional stabilization Therapy Interfering Behaviors Treatment retention Collaboration Federici & Wisniewski (2013) emilyprogram.com What our patients have said • This is the first time I’ve eaten on my own outside of a hospital.” • “I learned to notice emotions and decipher them more clearly, to managing urges from self-destructive behavior, and to take greater self-responsibility.” • “This was the first program that made me feel empowered – all the other treatments took that away from me – they made decisions for me, made me feel helpless. This program believed that I could figure out my problems and be skillful – that was the most important thing for me” emilyprogram.com Where does this leave us? • Start with adherent CBT – If unsuccessful… • Modified DBT: Good for Mild BED/BN – Use the manual! • Comprehensive DBT: to be considered for comorbid/complex patients who have not been helped by EBT for EDs – Get trained! emilyprogram.com emilyprogram.com