Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
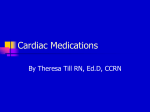
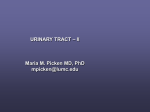
Nuclear Hormone Receptors as Regulators of the Renin-Angiotensin-Aldosterone System Irma Kuipers, Pim van der Harst, Gerjan Navis, Linda van Genne, Fulvio Morello, Wiek H. van Gilst, Dirk J. van Veldhuisen, Rudolf A. de Boer T Downloaded from http://hyper.ahajournals.org/ by guest on May 6, 2017 he renin-angiotensin-aldosterone system (RAAS) has been identified as the main system involved in blood pressure regulation, renal hemodynamics, and sodiumvolume homeostasis. Furthermore, the RAAS directly affects vascular and cardiac remodeling through proliferative and inflammatory signaling. Pharmacological targeting of the RAAS is a consolidated and evidence-based approach in the treatment of various aspects of cardiovascular disease. An exploding number of recent studies have provided novel insights into nuclear receptor biology in relation to cardiovascular (patho)physiology. In particular, members of the nuclear hormone receptor (NHR) superfamily have been identified as key molecules in various relevant cellular processes. As such, NHRs have been proposed as amenable targets for therapy, and their role in cardiovascular disease is currently explored. This review focuses on the potential effects of NHRs on the RAAS, summarizing the extensive body of evidence from experimental, animal, and clinical studies, suggesting that NHRs and the RAAS are closely intertwined. We discuss how these findings might translate into the clinical setting and discuss the (older) trials that evaluated NHR agonists in humans. We postulate that therapies targeting NHRs will cause ancillary effects (ie, modulating the RAAS) that need to be considered. indicated as “orphan” receptors, because their ligands are as yet unknown. After activation by their ligands, NHRs bind to DNA-responsive elements located within target gene promoters or have cross-talk with other signaling pathways. Effects are often modified by nuclear coregulators (coactivators and corepressors). However, if and how different NHRs may affect the RAAS remain largely unknown. Angiotensin II (Ang II) is the main effector peptide of the RAAS. Other end products are generated as well, such as angiotensin IV, angiotensin (1-7), and others (detailed in Figure S1). In this review, we focus mainly on the effects of NHRs on renin, angiotensinogen, and angiotensin receptors. NHRs and Renin Renin is (almost) exclusively secreted from specialized juxtaglomerular (JG) cells, located in the afferent arterioles of the kidney. Renin transcription is tightly regulated.3 It has become clear that several NHRs regulate renin transcription through interaction with specific responsive elements in the renin promoter (Figure 1). Through specific responsive elements, NHRs can act as either positive or negative regulators of renin transcription (Table). Liver X Receptors Liver X receptor (LXR)-␣ and the highly homologous LXR- are important modulators of lipid and glucose metabolism, inflammation, and innate immunity.4 LXR-␣ is expressed predominantly in liver, gut, heart, kidney, and adrenals, whereas LXR- is ubiquitously expressed. Tamura et al5 provided evidence that LXRs play an important role in renin regulation. Previously, they described a specific responsive element in the mouse renin promoter, called cAMP-negative response element (CNRE; Figure 1). LXR-␣ was identified as a CNRE-binding protein that regulates renin mRNA expression. This finding was confirmed recently using a mouse in vivo model.6 Both LXR-␣ and LXR- were shown to be regulators of renin transcription. Renal expression of LXR-␣ was found confined to JG cells (Figure 2). Interestingly, LXR-␣ and LXR- markedly differ in their control of renin NHRs and the RAAS NHRs constitute a superfamily of ligand-activated transcription factors involved in multiple cellular functions, acting as monomers, homodimers, or heterodimers (usually with the retinoid X receptors). The NHR superfamily is divided into 6 subfamilies (Table S1, available in the data supplement online at http://hyper.ahajournals.org).1 Cloning of the NHRs revealed that many of the NHRs share close homology. The fourth, fifth, and sixth classes (not mentioned in Table S1) include various NHRs that are less well described. NHR ligands include hormones, xenobiotics, prostaglandins, fatty acids, and cholesterol derivatives. An overwhelming amount of evidence exists for the role of NHR in cholesterol, lipid, and glucose metabolism.2 Several NHRs are provisionally Received December 19, 2007; first decision January 9, 2008; revision accepted March 17, 2008. From the Departments of Cardiology (I.K., P.v.d.H., L.v.G., W.H.v.G., D.J.v.V., R.A.d.B.) and Nephrology (G.N.), University Medical Center Groningen, University of Groningen, Groningen, The Netherlands; and the IVth Division of Internal Medicine (F.M.), San Vito Hospital, Torino, Italy. Correspondence to Rudolf A. de Boer, Department of Cardiology, University Medical Center Groningen, University of Groningen, PO Box 30.001, 9700 RB, Groningen, The Netherlands. E-mail [email protected] (Hypertension. 2008;51:1442-1448.) © 2008 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.107.108530 1442 Kuipers et al vitamin D retinoic acid RXR VDR Ear2 thyroxine NHRs as Regulators of the RAAS FA, fibrates, TZDs 1443 cAMP, oxysterols RAR P competition TR PPAR RXR LXR TGACCT (N)10 TGACCT AGGTCA caa tGTTCCT AGGTCA (N)1,2 AGGTCA TC(C/T)CA(C/G)AG -2633 to -2615 -1061 to -1046 ?? -607 to -600 T3R/RARE TRHE PPRE CNRE Enhancer elements Eb and Ec Figure 1. Schematic overview of NHR responsive elements in the renin promoter and topographical position in the renin promoter. Ligands are listed above NHRs. NHRs acting as positive regulators are displayed in green boxes; negative regulators are in red boxes. Liganded NHRs have a small triangle on top. P indicates phosphorylated; THRE, thyroid hormone response element. Downloaded from http://hyper.ahajournals.org/ by guest on May 6, 2017 transcription, because the latter constitutively upregulates renin mRNA expression, whereas LXR-␣ increases renin mRNA only in a cAMP-dependent manner. Importantly, high-renin status models were associated with prominent LXR-␣ binding activity to the CNRE. Experiments in LXRdeficient mice confirmed that LXR-␣ is necessary for the cAMP-dependent response of JG cells, whereas LXR- confers a basal constitutive effect on renin transcription and seems not strictly required for the functional responses of the JG apparatus. LXR agonists are currently explored as a novel therapy aimed at enhancing reverse cholesterol transport, thereby inhibiting the progression of atherosclerosis. To our knowledge, no LXR-specific interventions have been put to test in humans yet. The observation that LXRs function as renin regulators may warrant the development of selective modulators of LXR function that circumvent renin activation while retaining the advantageous effects on lipid metabolism. Vitamin D Receptors Li et al7 reported direct evidence that the vitamin D receptor (VDR) acts as a negative regulatory factor of renin transcription. VDR-transfected As4.1 cells treated with calcitriol Table. exhibited an almost complete abolishment of renin expression. Treatment of wild-type mice with vitamin D also suppressed renin expression, whereas in VDR-deficient mice, renin expression was elevated several-fold. So, vitamin D yields a direct negative regulatory effect on renin expression through a VDR-mediated mechanism. These findings are in agreement with the well-known inverse correlation between plasma vitamin D and blood pressure related to decreased plasma renin activity in humans.8 Thyroid Hormone Receptors Thyroid hormone receptor (TR) expression is ubiquitous, including in the kidney. Ichihara et al9 showed that, in cultured rat JG cells, treatment with thyroid hormones induces renin transcription/secretion in a dose-dependent fashion. The same group described 3 candidate thyroid hormone response elements (Figure 1) located in the human renin gene and showed that, in CaLu-6 cells, thyroid hormones stimulate the transcription of the human renin gene.10 In vivo, plasma renin activity and renal renin expression are significantly reduced in hypothyroid rats and elevated in hyperthyroid rats.11 Hyperthyroidism-induced cardiac hypertrophy is accompanied by activation of the cardiac RAAS with a signif- Summary of NHRs Acting as Regulators of Renin Transcription NHR LXR-␣ LXR- Activator Tested Positive/Negative Regulator Heterodimer/Monomer Binding Sequence References cAMP Positive Monomer CNRE 5, 6 Unliganded Positive Monomer CNRE 6 TR Thyroid hormone (T3) Positive Monomer TRHE 9, 10, 12 VDR 1–25(OH)2 vitamin D3 Negative Both? Ec/Eb/DR3 7 Fibrates Positive Unknown Unknown 16, 21 PPAR-␣ PPAR-␥ Fatty acid, TZDs Positive Unknown Unknown 25 9-Cis-retinoic acid, retinoic acid Positive (Hetero/homo) dimer DR2/DR3/DR4/DR5 59 Ear2 Unknown Negative Unknown RARE 60 MR Aldosterone Positive Both Unknown 61 RXR-␣/RAR-␣ THRE indicates thyroid hormone response element; TZD, thiazolidinedione; RXR, retinoid X receptor; RAR, retinoic acid receptor; RARE, rapid acquisition with relaxation enhancement; MR, mineralcorticoid receptor. 1444 Hypertension June 2008 itant blood pressure reduction or other ancillary effects of PPAR agonists (eg, antiinflammatory and antiproliferative effects on the vasculature or increased sympathetic activity). Activation of PPAR-␥ signaling has been consistently shown to lower blood pressure in various animal models and in human studies, at least in part through direct vascular effects.20 –23 However, controversy remains concerning the mechanism of how PPAR-␥ influences blood pressure regulation. In an in vitro study using CaLu-6 cells, it was shown that activation of PPAR-␥, both by endogenous and pharmacological agonists, causes a significant increase in renin transcription.24 In a small clinical study, however, the PPAR-␥ agonist pioglitazone reduced plasma renin levels in humans.25 Overall, there is scarce evidence suggesting that PPAR-␥ is a candidate regulator of JG cell function; further studies should specifically address this issue. Downloaded from http://hyper.ahajournals.org/ by guest on May 6, 2017 Figure 2. LXR-␣ is coexpressed with renin in JG cells in the murine kidney. Strict colocalization is observed with dual in situ hybridization. Both signals colocalized in JG cells (middle panel). Reprinted with permission from Morello et al.6 icant upregulation of renin mRNA in the kidney.12 Taken together, several lines of evidence suggest that TRs function as positive regulators of renin transcription. Peroxisome Proliferator-Activated Receptors Pharmacological targeting of peroxisome proliferator-activated receptors (PPARs; fibrates and thiazolidinediones) has been tested in the treatment of dyslipidemia, diabetes, and established cardiovascular diseases, such as heart failure and myocardial infarction. The 2 isoforms of PPAR are discussed in detail below. Several animal studies have suggested a role for PPAR-␣ in the control of renin expression. PPAR-␣– deficient mice put on a high-fat diet are protected from the development of hypertension.13 Mice deficient for both the low-density lipoprotein receptor and PPAR-␣ have been used to elucidate the role of PPAR-␣ in the development of glucocorticoidrelated insulin resistance.14 In the absence of PPAR-␣, mice were normotensive and euglycemic, despite dexamethasone treatment. When hepatic PPAR-␣ expression was restored by gene transfer, it not only reinduced hyperglycemia, but also increased plasma renin activity, blood pressure, sympathetic nervous activity, and renal sodium retention. Similar results were obtained in PPAR-␣– deficient Tsukuba hypertensive mice.15 Tsukuba hypertensive mice carry the human renin and angiotensinogen genes and serve as a model of Ang IImediated hypertension. PPAR-␣ deficiency in Tsukuba hypertensive mice decreases plasma renin concentration by ⬇50% and prevents hypertension and myocardial hypertrophy. These observations are supported by observations made in spontaneously hypertensive rats16 and healthy, human volunteers.17 The exact role of PPAR-␣ in the regulation of blood pressure remains unclear, because several other studies conducted in various rat models of hypertension have provided inconsistent results.18,19 It is currently not known whether renin activation associated with PPAR-␣ activation is a direct transcriptional effect of PPAR-␣ or if it should be regarded as a secondary phenomenon, attributable to concom- Steroid Hormone Receptors So far, the specific role of the estrogen receptors and progesterone receptors in renin expression has not been addressed directly. Renin levels fluctuate with the menstrual cycle, suggesting that estrogen and progesterone are regulators of renin transcription. In cultured human chorion cells, progesterone, estradiol, testosterone, and aldosterone all affect renin expression levels.26 Estradiol and progesterone seem to synergistically increase renin expression, because the combined treatment with both completely restores renin expression in ovariectomized rats.27 Prorenin and renin are released from placental cytotrophoblastic tissue.28 This release occurs in parallel with other placental hormones but does not appear to be regulated by steroid receptors, human chorionic gonadotrophin, intracellular calcium, or cAMP. Therefore, (pro)renin release from placenta may in fact be regulated in a different fashion from renal renin release, eg, by local factors, such as estrogen and progesterone. Renin Receptor In 2002, a human renin/prorenin receptor was been cloned, which specifically binds renin and prorenin.29 Binding of renin to its receptor increases the catalytic activity of renin, and binding of prorenin renders prorenin enzymatically active, comparable to renin. Although studies revealing transcription mechanisms of the renin receptor are currently underway,30 thus far no “classical” NHRs have been identified as transcription factors for the renin/prorenin receptor. NHRs and Angiotensinogen Presently, only TRs, PPARs, and estrogen receptors have been implicated in angiotensinogen transcriptional activation and will be discussed below. Thyroid Hormone Receptors The thyroid hormone is a positive regulator of angiotensinogen. Hyperthyroidism, induced by treatment with thyroid hormone (T3), causes an increase of plasma angiotensinogen by 85% in rats.31 In parallel, hypothyroidism results in a 71% decrease of plasma angiotensinogen levels. Similar results were found in vitro.32 T3 treatment causes upregulation of angiotensinogen transcription in the human hepatic cell line Kuipers et al HepG2. We speculate that the well-described effects of thyroid hormones on blood pressure can partially be explained through regulation of angiotensinogen expression and consequent activation of the RAAS. Peroxisome Proliferator-Activated Receptors Downloaded from http://hyper.ahajournals.org/ by guest on May 6, 2017 PPAR-␣ acts as a positive regulator of angiotensinogen transcription. In contrast to HepG2 cells, HeLa cells treated with the PPAR-␣ agonist bezafibrate displayed activation of the angiotensinogen promoter.33 This difference between HepG2 and HeLa cells might be explained by the presence of hepatocyte nuclear factor-4 in HepG2. Hepatocyte nuclear factor-4 binds to the same responsive region of the angiotensinogen promoter as PPAR-␣. Hepatocyte nuclear factor-4 is not present in the cervical cell line HeLa, and cotransfaction of hepatocyte nuclear factor-4 expression in HeLa cells attenuated the activation of the angiotensinogen promoter by bezafibrate. A dominant-negative form of the PPAR-␥ gene was cloned to create a transgenic mouse strain.34 The used mutation was equivalent to the P467L mutation in humans causing severe insulin resistance and hypertension. The mouse strain did not develop high blood pressure nor increased kidney renin mRNA content. However, upregulations of angiotensinogen and the angiotensin type 1 receptor (AT1R) were reported. Further research in these mice revealed an increased expression of angiotensinogen in their subcutaneous adipose tissue, suggesting a role for PPAR-␥ in blood pressure regulation, via the RAAS, by modulating angiotensinogen expression in fatty tissue. Steroid Hormone Receptors Early studies demonstrated that estrogens and glucocorticoids can regulate hepatic angiotensinogen production.35 Estrogen treatment results in a prompt and significant upregulation of angiotensinogen mRNA in rodent liver cells.36 Similar findings have been reported in humans, where women receiving oral contraceptives or estrogen replacement therapy develop increased circulating angiotensinogen and Ang II levels.37 Overall, the effects of estrogen receptor on angiotensinogen are potentially important in the pathophysiology of hypertension in susceptible women and should be considered when contraceptive or hormone replacement regimens are prescribed. NHRs and Angiotensin Receptors The effects of Ang II are mainly mediated via 2 plasma membrane receptors, AT1R and angiotensin type 2 receptor (AT2R). Most effects of Ang II are mediated by the AT1R, including an increase of arterial blood pressure, aldosterone secretion, and adverse cardiac and renal remodeling. Rodents express 2 subtypes of the AT1R (A and B), whereas humans express only 1 subtype. AT2R is expressed at high levels in fetal tissues and decreases rapidly after birth. Although the exact function of AT2Rs is less well understood than that of the AT1R, it seems that AT2Rs antagonize AT1R-mediated effects. We discuss the influence of PPARs and steroid hormone receptors on AT1Rs and AT2Rs below. NHRs as Regulators of the RAAS 1445 Peroxisome Proliferator-Activated Receptors The role of PPARs in AT1R expression is well established. It has been convincingly shown that the expression of AT1Rs is decreased by PPAR-␥ agonists in rat vascular smooth muscle cells,38 leading to functional inhibition of Ang II-induced cell proliferation via AT1Rs. Functionally, Diep et al39 showed that treatment with the PPAR-␥ activators rosiglitazone and pioglitazone attenuated the detrimental effects of Ang II infusion in rats. Development of hypertension, small resistance artery remodeling, endothelial dysfunction, proinflammatory mediators, and upregulation of AT1Rs, all of which are increased by Ang II infusion, were blunted in blood vessels of rats treated with rosiglitazone or pioglitazone. Diep et al,39 furthermore, showed that PPAR-␥ ligands are capable of increasing AT2R expression on a protein level. These findings are consistent with the significant increase in myocardial AT2R mRNA found in rosiglitazone-fed rats subjected to an ischemia-reperfusion model.40 Whereas in this model AT1R mRNA expression was reduced after rosiglitazone treatment, AT2R mRNA expression was increased by ⬎100-fold. Cross-talk between angiotensin receptors and PPAR-␥ is, thus, relevant. This is further underscored by the observation that some angiotensin receptor blockers, such as telmisartan and irbesartan are in fact partial PPAR-␥ agonists.41 The influence of PPAR-␣ activator docosahexaenoic acid (DHA) has also been investigated in Ang II-infused rats.42 Like activation of PPAR-␥, activation of PPAR-␣ also attenuated the damaging effects of Ang II infusion in rats, resulting in reduction of Ang II-induced oxidative stress, expression of inflammatory mediators, blood pressure, endothelial dysfunction, and remodeling of small resistance arteries. The potential clinical implications of the interaction between PPARs and the AT1R is discussed in detail below. Steroid Hormone Receptors Sex hormones, especially estrogens, modulate the expression of angiotensin receptors. Estrogen attenuates AT1R mRNA, but increases AT2R gene expression in rat cardiac fibroblasts.43 In line with this, increased AT1R expression was found in estrogen treated ovariectomized rats and cell cultures of rat smooth muscle cells.44 Later, this group showed that progesterone addition to smooth muscle cell cultures upregulated AT1R expression.45 It may be speculated that the contrary effects of female sex hormones on angiotensin receptor expression could be involved in the changes in arterial pressure during the menstrual cycle and perhaps also postmenopausal. Potential Clinical Implications The discussed data suggest that modulation of NHR activity comodulates RAAS activity. Large-scale clinical studies with NHR agonists have been conducted or are underway, with potential clues on the role of NHRs in cardiovascular disease. Specific agonists of PPAR-␣, PPAR-␥, VDR, and steroid hormone receptors have been put to trial, whereas other agonists are yet to enter the clinical arena. Unfortunately, most clinical trials did not include end-points directly linked to the RAAS, such as plasma renin activity or angiotensin- 1446 Hypertension June 2008 converting enzyme activity. We will discuss the limited data available. Vitamin D Receptors Downloaded from http://hyper.ahajournals.org/ by guest on May 6, 2017 Vitamin D acts as a negative regulator of renin and might consequently reduce cardiovascular morbidity and mortality. Currently, no large-scale mortality trials have tested the efficacy of vitamin D in reducing events in patients with established cardiovascular disease. Some clues are available from trials in patients with end-stage renal disease (ESRD), when vitamin D is primarily prescribed to treat secondary hyperparathyroidism. In a small study, analyzing 242 chronic hemodialysis patients, patients treated with alfacalcidol (a vitamin D analogue) had a significantly lower risk of cardiovascular mortality than patients with no vitamin D treatment.46 In fact, several observational studies indicate that there may be a protective effect of vitamin D treatment against cardiovascular disease. This claim is hitherto restricted to hemodialysis patients with ESRD whose main cause of death is cardiovascular. We postulate that in patients with low serum vitamin D levels, and who are at risk for cardiovascular disease, the use of oral vitamin D substitutes may reduce the risk for future cardiovascular events. Peroxisome Proliferator-Activated Receptors PPAR-␣ agonists have been primarily tested in patients with hypertriglyceridemia and end-points in such studies typically were coronary events and death. The clinical use of fibrates preceded the identification of PPAR-␣ as a nuclear receptor, harboring potential ancillary effects beyond lipid lowering. As such, clinical trials with PPAR-␣ agonists could be revisited for clues regarding the impact of presumable PPAR-␣ activation on RAAS activity. There are observations that support the notion that other effects than lipid-lowering effect alone play an important role. For instance, in the Helsinki study, a paradoxical increase in noncoronary death was observed.47 However, to our knowledge, in large scale trials with PPAR-␣ agonist, such as the Helsinki Heart Study, the Veteran’s Administration-HDL Intervention Trial (VA-HIT),48 and the FIELD,49 no analyses were conducted with regard to RAAS activity. PPAR-␥ agonists (thiazolidinediones) exert beneficial effects on the vasculature, including decreased carotid artery intima-medial thickness,50 improved endothelial function, and decreased inflammation.51 Because the RAAS is a dominant player in vascular remodeling, we speculate on some effects to be conferred via the RAAS. In previous sections, we discussed experimental data that show the interaction between PPAR-␥ and the RAAS. This interaction is predominantly at the level of the AT1R. Some angiotensin receptor blockers are partial PPAR-␥ agonists, whereas treatment with glitazones can block Ang II-mediated effects.52 Some metabolic effects of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, including a reduction of new-onset diabetes, as seen in the Heart Outcomes Prevention Evaluation53 and the Losartan Intervention for Endpoint Reduction in Hypertension,54 are suggestive for the existence of PPAR-␥–like effects of RAAS inhibition. Several large-scale randomized, controlled trials with PPAR-␥ agonists have been completed recently. The Prospective Pioglitazone Clinical Trial in Macrovascular Events55 showed rather favorable outcomes, such as a decrease in recurrent myocardial infarction and a decrease in recurrent stroke. The Diabetes Reduction Approaches With Ramipril and Rosiglitazone Medications Study established a decrease in progression to diabetes in prediabetic patients (with impaired glucose tolerance and/or impaired fasting glucose) in rosiglitazone-treated patients.56 Unfortunately, none of these trials reported any parameters of RAAS activity. These outcomes may suggest that PPAR-␥ agonists decrease cardiovascular events over time; however, this remains speculative. Recently, PPAR-␥ agonists have come under fire because of claims that they may increase rather than decrease the risk of myocardial infarction.57 Although the limitations of this meta-analysis have been pointed out by its authors and by others,58 controversy remains concerning the safety of thiazolidinedione treatment. From the trials with PPAR agonists, it becomes clear that the theoretical working profile is not paralleled with a (solely) beneficial clinical efficacy. Likely, the effects that PPARs exert are more global that we currently understand: the beneficial effects may not outweigh adverse effects. We suggest putting combinatorial therapies with RAAS-inhibitors and PPAR-␥ agonists to test in future studies, because from the theory this might be more efficacious than either therapy alone. Perspectives NHRs have emerged as a class of receptors with a wide array of physiological effects pertaining to fatty acid, lipid, and carbohydrate metabolism but also to other pathways, such as inflammation, cellular proliferation, and vascular remodeling. These processes are pivotal in cardiovascular disease, and pharmacological targeting of NHRs might provide a novel and promising treatment approach. Some agonists of NHRs have entered the clinical arena, showing a promising efficacy and safety profile. Because the RAAS is a main player in cardiovascular homeostasis, any effects of NHRs on RAAS activity may likely affect its working and safety profile. In this review, we discussed the levels of interaction between some NHRs and the RAAS. Experimental studies have partially elucidated the molecular mechanisms of the regulation of the RAAS by NHRs. It is speculated that, by exploring the clinical value of NHRs, the effect on RAAS activation may have important repercussions for their efficacy and safety. We, therefore, recommend that future clinical studies include analyses of RAAS activation. Source of Funding This work was supported by the Netherlands Heart Foundation (grant 2004T004). Disclosures None. Kuipers et al References Downloaded from http://hyper.ahajournals.org/ by guest on May 6, 2017 1. Aranda A, Pascual A. Nuclear hormone receptors and gene expression. Physiol Rev. 2001;81:1269 –1304. 2. Desvergne B, Michalik L, Wahli W. Transcriptional regulation of metabolism. Physiol Rev. 2006;86:465–514. 3. Persson PB, Skalweit A, Mrowka R, Thiele BJ. Control of renin synthesis. Am J Physiol Regul Integr Comp Physiol. 2003;285:R491–R497. 4. Barish GD. Peroxisome proliferator-activated receptors and liver X receptors in atherosclerosis and immunity. J Nutr. 2006;136:690 – 694. 5. Tamura K, Chen YE, Horiuchi M, Chen Q, Daviet L, Yang Z, LopezIlasaca M, Mu H, Pratt RE, Dzau VJ. LXR␣ functions as a cAMPresponsive transcriptional regulator of gene expression. Proc Natl Acad Sci U S A. 2000;97:8513– 8518. 6. Morello F, de Boer RA, Steffensen KR, Gnecchi M, Chisholm JW, Boomsma F, Anderson LM, Lawn RM, Gustafsson JK, Lopez-Ilasaca M, Pratt RE, Dzau VJ. Liver X receptors alpha and beta regulate renin expression in vivo. J Clin Invest. 2005;115:1913–1922. 7. Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1,25Dihydroxyvitamin D(3) is a negative endocrine regulator of the renin-angiotensin system. J Clin Invest. 2002;110:229 –238. 8. Resnick LM, Muller FB, Laragh JH. Calcium-regulating hormones in essential hypertension. Relation to plasma renin activity and sodium metabolism. Ann Intern Med. 1986;105:649 – 654. 9. Ichihara A, Kobori H, Miyashita Y, Hayashi M, Saruta T. Differential effects of thyroid hormone on renin secretion, content, and mRNA in juxtaglomerular cells. Am J Physiol. 1998;274:E224 –E231. 10. Kobori H, Hayashi M, Saruta T. Thyroid hormone stimulates renin gene expression through the thyroid hormone response element. Hypertension. 2001;37:99 –104. 11. Kobori H, Ichihara A, Suzuki H, Miyashita Y, Hayashi M, Saruta T. Thyroid hormone stimulates renin synthesis in rats without involving the sympathetic nervous system. Am J Physiol. 1997;272:E227–E232. 12. Kobori H, Ichihara A, Suzuki H, Takenaka T, Miyashita Y, Hayashi M, Saruta T. Role of the renin-angiotensin system in cardiac hypertrophy induced in rats by hyperthyroidism. Am J Physiol. 1997;273:H593–H599. 13. Tordjman K, Bernal-Mizrachi C, Zemany L, Weng S, Feng C, Zhang F, Leone TC, Coleman T, Kelly DP, Semenkovich CF. PPARalpha deficiency reduces insulin resistance and atherosclerosis in apoE-null mice. J Clin Invest. 2001;107:1025–1034. 14. Bernal-Mizrachi C, Weng S, Feng C, Finck BN, Knutsen RH, Leone TC, Coleman T, Mecham RP, Kelly DP, Semenkovich CF. Dexamethasone induction of hypertension and diabetes is PPAR-alpha dependent in LDL receptor-null mice. Nat Med. 2003;9:1069 –1075. 15. Tordjman KM, Semenkovich CF, Coleman T, Yudovich R, Bak S, Osher E, Vechoropoulos M, Stern N. Absence of peroxisome proliferator-activated receptor-alpha abolishes hypertension and attenuates atherosclerosis in the Tsukuba hypertensive mouse. Hypertension. 2007;50:945–951. 16. Shatara RK, Quest DW, Wilson TW. Fenofibrate lowers blood pressure in two genetic models of hypertension. Can J Physiol Pharmacol. 2000; 78:367–371. 17. Subramanian S, DeRosa MA, Bernal-Mizrachi C, Laffely N, Cade WT, Yarasheski KE, Cryer PE, Semenkovich CF. PPARalpha activation elevates blood pressure and does not correct glucocorticoid-induced insulin resistance in humans. Am J Physiol Endocrinol Metab. 2006;291: E1365–E1371. 18. Diep QN, Benkirane K, Amiri F, Cohn JS, Endemann D, Schiffrin EL. PPAR alpha activator fenofibrate inhibits myocardial inflammation and fibrosis in angiotensin II-infused rats. J Mol Cell Cardiol. 2004;36: 295–304. 19. Williams JM, Zhao X, Wang MH, Imig JD, Pollock DM. Peroxisome proliferator-activated receptor-alpha activation reduces salt-dependent hypertension during chronic endothelin B receptor blockade. Hypertension. 2005;46:366–371. 20. Willson TM, Lambert MH, Kliewer SA. Peroxisome proliferator-activated receptor gamma and metabolic disease. Annu Rev Biochem. 2001; 70:341–367. 21. Iglarz M, Touyz RM, Viel EC, Paradis P, Amiri F, Diep QN, Schiffrin EL. Peroxisome proliferator-activated receptor-alpha and receptorgamma activators prevent cardiac fibrosis in mineralocorticoid-dependent hypertension. Hypertension. 2003;42:737–743. 22. Ryan MJ, Didion SP, Mathur S, Faraci FM, Sigmund CD. PPAR(gamma) agonist rosiglitazone improves vascular function and lowers blood pressure in hypertensive transgenic mice. Hypertension. 2004;43: 661– 666. NHRs as Regulators of the RAAS 1447 23. Dobrian AD, Schriver SD, Khraibi AA, Prewitt RL. Pioglitazone prevents hypertension and reduces oxidative stress in diet-induced obesity. Hypertension. 2004;43:48 –56. 24. Todorov VT, Desch M, Schmitt-Nilson N, Todorova A, Kurtz A. Peroxisome proliferator-activated receptor-gamma is involved in the control of renin gene expression. Hypertension. 2007;50:939 –944. 25. Zanchi A, Chiolero A, Maillard M, Nussberger J, Brunner HR, Burnier M. Effects of the peroxisomal proliferator-activated receptor-gamma agonist pioglitazone on renal and hormonal responses to salt in healthy men. J Clin Endocrinol Metab. 2004;89:1140 –1145. 26. Duncan KG, Haidar MA, Baxter JD, Reudelhuber TL. Regulation of human renin expression in chorion cell primary cultures. Proc Natl Acad Sci U S A. 1990;87:7588 –7592. 27. De Vito E, Guardia DC, Cabrera RR. Cyclical changes in plasma renin during the oestrous cycle in the rat: synchronized effect of oestrogen and progesterone. J Endocrinol. 1989;121:261–267. 28. Lenz T. Release of prorenin and placental hormones from superfused minced chorion laeve. Acta Obstet Gynecol Scand. 1997;76:903–906. 29. Nguyen G, Delarue F, Burckle C, Bouzhir L, Giller T, Sraer JD. Pivotal role of the renin/prorenin receptor in angiotensin II production and cellular responses to renin. J Clin Invest. 2002;109:1417–1427. 30. Schefe JH, Menk M, Reinemund J, Effertz K, Hobbs RM, Pandolfi PP, Ruiz P, Unger T, Funke-Kaiser H. A novel signal transduction cascade involving direct physical interaction of the renin/prorenin receptor with the transcription factor promyelocytic zinc finger protein. Circ Res. 2006; 99:1355–1366. 31. Marchant C, Brown L, Sernia C. Renin-angiotensin system in thyroid dysfunction in rats. J Cardiovasc Pharmacol. 1993;22:449 – 455. 32. Lin KH, Lee HY, Shih CH, Yen CC, Chen SL, Yang RC, Wang CS. Plasma protein regulation by thyroid hormone. J Endocrinol. 2003;179: 367–377. 33. Shimamoto Y, Hirota K, Fukamizu A. Effect of peroxisome proliferatoractivated receptor alpha on human angiotensinogen promoter. Int J Mol Med. 2004;13:729 –733. 34. Tsai YS, Kim HJ, Takahashi N, Kim HS, Hagaman JR, Kim JK, Maeda N. Hypertension and abnormal fat distribution but not insulin resistance in mice with P465L PPARgamma. J Clin Invest. 2004;114:240 –249. 35. Eisenfeld AJ, Aten R, Weinberger M, Haselbacher G, Halpern K, Krakoff L. Estrogen receptor in the mammalian liver. Science. 1976;191: 862– 865. 36. Stavreus-Evers A, Parini P, Freyschuss B, Elger W, Reddersen G, Sahlin L, Eriksson H. Estrogenic influence on the regulation of hepatic estrogen receptor-alpha and serum level of angiotensinogen in female rats. J Steroid Biochem Mol Biol. 2001;78:83– 88. 37. Kang AK, Duncan JA, Cattran DC, Floras JS, Lai V, Scholey JW, Miller JA. Effect of oral contraceptives on the renin angiotensin system and renal function. Am J Physiol Regul Integr Comp Physiol. 2001;280: R807–R813. 38. Sugawara A, Takeuchi K, Uruno A, Ikeda Y, Arima S, Kudo M, Sato K, Taniyama Y, Ito S. Transcriptional suppression of type 1 angiotensin II receptor gene expression by peroxisome proliferator-activated receptor-gamma in vascular smooth muscle cells. Endocrinology. 2001; 142:3125–3134. 39. Diep QN, El Mabrouk M, Cohn JS, Endemann D, Amiri F, Virdis A, Neves MF, Schiffrin EL. Structure, endothelial function, cell growth, and inflammation in blood vessels of angiotensin II-infused rats: role of peroxisome proliferator-activated receptor-gamma. Circulation. 2002; 105:2296 –2302. 40. Molavi B, Chen J, Mehta JL. Cardioprotective effects of rosiglitazone are associated with selective overexpression of type 2 angiotensin receptors and inhibition of p42/44 MAPK. Am J Physiol Heart Circ Physiol. 2006;291:H687–H693. 41. Benson SC, Pershadsingh HA, Ho CI, Chittiboyina A, Desai P, Pravenec M, Qi N, Wang J, Avery MA, Kurtz TW. Identification of telmisartan as a unique angiotensin II receptor antagonist with selective PPARgammamodulating activity. Hypertension. 2004;43:993–1002. 42. Diep QN, Amiri F, Touyz RM, Cohn JS, Endemann D, Neves MF, Schiffrin EL. PPARalpha activator effects on Ang II-induced vascular oxidative stress and inflammation. Hypertension. 2002;40:866 – 871. 43. Zhou L, Shao Y, Huang Y, Yao T, Lu LM. 17-Estradiol inhibits angiotensin II-induced collagen synthesis of cultured rat cardiac fibroblasts via modulating angiotensin II receptors. Eur J Pharmacol. 2007; 567:186 –192. 44. Nickenig G, Baumer AT, Grohe C, Kahlert S, Strehlow K, Rosenkranz S, Stablein A, Beckers F, Smits JF, Daemen MJ, Vetter H, Bohm M. 1448 45. 46. 47. 48. 49. Downloaded from http://hyper.ahajournals.org/ by guest on May 6, 2017 50. 51. 52. Hypertension June 2008 Estrogen modulates AT1 receptor gene expression in vitro and in vivo. Circulation. 1998;97:2197–2201. Nickenig G, Strehlow K, Wassmann S, Baumer AT, Albory K, Sauer H, Bohm M. Differential effects of estrogen and progesterone on AT(1) receptor gene expression in vascular smooth muscle cells. Circulation. 2000;102:1828 –1833. Shoji T, Shinohara K, Kimoto E, Emoto M, Tahara H, Koyama H, Inaba M, Fukumoto S, Ishimura E, Miki T, Tabata T, Nishizawa Y. Lower risk for cardiovascular mortality in oral 1alpha-hydroxy vitamin D3 users in a haemodialysis population. Nephrol Dial Transplant. 2004;19:179 –184. Frick MH, Elo O, Haapa K, Heinonen OP, Heinsalmi P, Helo P, Huttunen JK, Kaitaniemi P, Koskinen P, Manninen V. Helsinki Heart Study: primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. N Engl J Med. 1987;317:1237–1245. Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. Veterans Affairs HighDensity Lipoprotein Cholesterol Intervention Trial Study Group. N Engl J Med. 1999;341:410 – 418. Keech A, Simes RJ, Barter P, Best J, Scott R, Taskinen MR, Forder P, Pillai A, Davis T, Glasziou P, Drury P, Kesaniemi YA, Sullivan D, Hunt D, Colman P, d’Emden M, Whiting M, Ehnholm C, Laakso M. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005;366:1849 –1861. Sidhu JS, Kaposzta Z, Markus HS, Kaski JC. Effect of rosiglitazone on common carotid intima-media thickness progression in coronary artery disease patients without diabetes mellitus. Arterioscler Thromb Vasc Biol. 2004;24:930 –934. Campia U, Matuskey LA, Panza JA. Peroxisome proliferator-activated receptor-gamma activation with pioglitazone improves endotheliumdependent dilation in nondiabetic patients with major cardiovascular risk factors. Circulation. 2006;113:867– 875. Benkirane K, Amiri F, Diep QN, El Mabrouk M, Schiffrin EL. PPAR-gamma inhibits ANG II-induced cell growth via SHIP2 and 4E-BP1. Am J Physiol Heart Circ Physiol. 2006;290:H390 –H397. 53. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med. 2000;342:145–153. 54. Dahlof B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, de Faire U, Fyhrquist F, Ibsen H, Kristiansson K, Lederballe-Pedersen O, Lindholm LH, Nieminen MS, Omvik P, Oparil S, Wedel H. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359:995–1003. 55. Dormandy JA, Charbonnel B, Eckland DJ, Erdmann E, Massi-Benedetti M, Moules IK, Skene AM, Tan MH, Lefebvre PJ, Murray GD, Standl E, Wilcox RG, Wilhelmsen L, Betteridge J, Birkeland K, Golay A, Heine RJ, Koranyi L, Laakso M, Mokan M, Norkus A, Pirags V, Podar T, Scheen A, Scherbaum W, Schernthaner G, Schmitz O, Skrha J, Smith U, Taton J. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trial. Lancet. 2005;366:1279 –1289. 56. Gerstein HC, Yusuf S, Bosch J, Pogue J, Sheridan P, Dinccag N, Hanefeld M, Hoogwerf B, Laakso M, Mohan V, Shaw J, Zinman B, Holman RR. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomised controlled trial. Lancet. 2006;368:1096 –1105. 57. Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007; 356:2457–2471. 58. Psaty BM, Furberg CD. Rosiglitazone and cardiovascular risk. N Engl J Med. 2007;356:2522–2524. 59. Shi Q, Gross KW, Sigmund CD. Retinoic acid-mediated activation of the mouse renin enhancer. J Biol Chem. 2001;276:3597–3603. 60. Liu X, Huang X, Sigmund CD. Identification of a nuclear orphan receptor (Ear2) as a negative regulator of renin gene transcription. Circ Res. 2003;92:1033–1040. 61. Klar J, Vitzthum H, Kurtz A. Aldosterone enhances renin gene expression in juxtaglomerular cells. Am J Physiol Renal Physiol. 2004;286: F349–F355. Nuclear Hormone Receptors as Regulators of the Renin-Angiotensin-Aldosterone System Irma Kuipers, Pim van der Harst, Gerjan Navis, Linda van Genne, Fulvio Morello, Wiek H. van Gilst, Dirk J. van Veldhuisen and Rudolf A. de Boer Downloaded from http://hyper.ahajournals.org/ by guest on May 6, 2017 Hypertension. 2008;51:1442-1448; originally published online April 14, 2008; doi: 10.1161/HYPERTENSIONAHA.107.108530 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2008 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/51/6/1442 An erratum has been published regarding this article. Please see the attached page for: /content/52/3/e30.full.pdf Data Supplement (unedited) at: http://hyper.ahajournals.org/content/suppl/2008/04/14/HYPERTENSIONAHA.107.108530.DC1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/ Correction In the Hypertension article by Kuipers et al (Kuipers I, van der Harst P, Navis G, van Genne L, Morello F, van Gilst WH, van Veldhuisen DJ, de Boer RA. Nuclear hormone receptors as regulators of the renin-angiotensin-aldosterone system. Hypertension. 2008;51:1442–1448) there is an incorrect statement in the upper right paragraph on page 1444. The statement “In a small clinical study, however, the PPAR-␥ agonist pioglitazone reduced plasma renin levels in humans.” should read “In a small clinical study, the PPAR-␥ agonist pioglitazone increased plasma renin levels in humans.” The authors regret the error. (Hypertension. 2008;52:e30.) © 2008 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.108.000074 e30 NUCLEAR HORMONE RECEPTORS AS REGULATORS OF THE RENIN-ANGIOTENSINALDOSTERONE SYSTEM Irma Kuipersa MSc; Pim van der Harsta MD; Gerjan Navisb MD; Linda van Gennea BSc; Fulvio Morelloc MD; Wiek H. van Gilsta PhD; Dirk J. van Veldhuisena MD; Rudolf A. de Boera MD From the Departments of Cardiologya and Nephrologyb from the University Medical Center Groningen, University of Groningen, PO Box 30.001, 9700 RB, Groningen, The Netherlands and from the IVth Division of Internal Medicinec, San Vito Hospital, Strada San Vito 34, 10134 Torino, Italy. Short title: NHRs as regulators of the RAAS Word count total manuscript: 5991 words Word count abstract: 136 words Number of figures: 2 figures Please address correspondence to: Rudolf A. de Boer, MD Department of Cardiology, University Medical Center Groningen, University of Groningen, PO Box 30.001, 9700 RB, Groningen, The Netherlands. Phone: +31503612355 / Fax: +31503614391 / E-mail address: [email protected] Table S1: Subfamilies of mammalian nuclear receptors (adapted and modified from2). Class Receptor Subtype Denomination Ligand I LXR , Liver X receptor Oxysterols, bile acids, T090317 Vitamin D receptor 1-25(OH)2 vitamin D3 VDR II III TR , Thyroid hormone receptor Thyroid hormone (T3) PPAR , / , Peroxisome proliferators-activated receptor Eicosanoids; thiazolidinediones (TZD’s); 15-deoxy-12,41prostaglandin J2; polyunsaturated fatty acids RAR , , Retinoic acid receptor Retinoic acid RXR , , Retinoid X receptor 9-Cis-retinoic acid COUP-TF , , Chicken ovalbumin upstream promoter transcription factor Unknown HNF-4 , , Hepatocyte nuclear factor 4 Fatty acyl-CoA thioesters MR Mineralocorticoid receptor Aldosterone GR Glucocorticoid receptor Glucocorticoids Estrogen receptor Estradiol PR Progesterone receptor Progestins AR Androgen receptor Androgens ER , Figure S1: Schematic overview of the RAAS. Renin is the primum movens of the RAAS and cleaves angiotensinogen into angiotensin I. Subsequently, angiotensin I is converted into angiotensin II by angiotensin-converting enzyme (ACE). Angiotensin II mediates its effects via the angiotensin type 1 receptor (AT1R) and type 2 receptor (AT2R).