Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
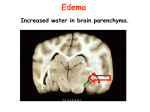
EMERGENCY MEDICINE Liverpool Hospital The Weekly Probe 1st April 2014 Volume 17 Issue 9 Congrats- congratulations to Lucy who passed her Primary exams last weekend! Well done!! Geris admissions- occasionally geris is “hammered “ with admissions. They have pointed out that, the following patients are usually not appropriately admitted under geriatrics: 1) Admitted for a condition which will require a procedure (e.g. gastroscopy, colonoscopy, angio). 2) Patients with single system reason for presentation (even if with other co-morbidities) – e.g. NSTEMI in an elderly patients, or aspiration pneumonia. 3) Patients who have previously been seen by a geriatrician > 1 month ago, and not presenting with a geriatric specific problem. 4) Patients refused by another team on the basis of age. Let Ian or Penny know if ou have any problems with these issues. NSW Police Accident Investigations – a recent memo was received from the MoH regarding the release of information to the appropriate Police Crash Investigators. Below is the relevant part of the flow sheet. THIS WEEK Last weeks case – herniation syndromes Neurosurgical treatment of Ischaemic Strokes Next Week’s Case Joke / Quote of the Week The Week Ahead LAST WEEK’S CASE – Cerebral / cerebellar Herniation A 65yo man presents with 24 hrs of headache, vomiting and unsteady gait. His CT shows evidence of a cerebellar infarct and he is admitted under neurology. However while waiting for a stroke bed he deteriorates neurologically. What can you do? The primary concern is that this patient is developing herniation due to progressive oedema +/- secondary bleeding. A plan needs to be developed ASAP. The skull is a rigid box with rigid partitions internally and holes which allow decompression externally. However when there is localised increase in volume (brain tissue, blood or CSF) this volume rise results in pressure increases and the brain moves through these partitions or externally through natural or surgical “foramen” ie it herniates. What is herniation? There are two major classes of herniation: supratentorial and infratentorial. Supratentorial herniation is of structures normally above the tentorial notch and infratentorial is of structures normally below it. a) Subfalcine (cingulate) b) Uncal herniation c) Central downward hern’n d) External / transcalvarial hern’n e) Tonsillar (cerebellar) hern’n Supratentorial herniation 1. 2. 3. 4. Uncal (transtentorial) Central Cingulate (subfalcine) Transcalvarial Infratentorial herniation Editor: Peter Wyllie 5. Upward (upward cerebellar or upward transtentorial) 6. Tonsillar (downward cerebellar) Uncal herniation- In uncal herniation, a common subtype of transtentorial herniation, the uncus, the innermost part of the temporal lobe is pushed against the brainstem , especially the midbrain. Symptoms : - 3rd cranial nerve compression - dilated pupil precedes ocular movement disorders with compression of surrounding parasympathetic fibres before the central motor fibres. Compression of the ipsilateral post cerebral artery – occipital ischaemia with contralateral homonymous hemianopia descending corticospinal and corticobulbar tract with contralateral hemiparesis (can be ipsilateral) pontine or midbrain compression with decorticate posturing, respiratiory centre depression, death. Central herniation – herniation of intracranial contents upwards through the tentorium cerebelli or more commonly downwards. In this situation, the diencephalon (thalamus, hypothalamus, subthalamus) and parts of the temporal lobes are pushed through the tentorium cerebelli. With herniation there is: - - stretching of the pontine arteries (branches of the basilar) with tearing and haemorrhage (Duret haemorrhage) Small, dilated, fixed pupils with paralysis of upward eye movement giving the characteristic appearance of "sunset eyes". Radiographically, downward herniation is characterized by obliteration of the suprasellar cistern with compression of the cerebral peduncles. This space may also be obliterated with incal herniation.(The suprasellar cistern is a CSF-fluid filled space located above the sella turcica (where the pituitary sits), under the hypothalamus. It contains the optic chiasm, and the circle of Willis - the shape of a pentagon at the level of the optic chiasm, and the shape of a six-point (Jewish) star at the level of cerebral peduncles- best seen when filled with blood from a SAH) . Upwards herniation, on the other hand, can be radiographically characterized by obliteration of the quadrigeminal cistern. May present with vomiting, headaches and obtundation. Editor: Peter Wyllie Cingulate herniation- or subfalcine herniation, the most common type, the innermost part of the frontal or parietal lobe is pushed under part of the falx cerebri. As the cingulate gyrus moves under the falx there is displacement of the septum pellucidum (between the 2 lateral ventricles), compression of the ipsilateral anterior frontal horn of the lateral ventricle and dilation of the contralateral frontal horn. This herniation may result in occlusion of the anterior cerebral artery with contralateral leg weakness, or it may progress to central herniation. Transcalvarial herniation- herniation through a fracture or a surgical site in the skull. Upward herniation- Increased pressure in the posterior fossa can cause the cerebellum move up through the tentorial opening in upward, or cerebellar herniation. usually caused by a slowly growing cerebellar or brainstem process, such as a diffusely infiltrating astrocytoma. O scanning there may be narrowing of the ambient and quadrigeminal cisterns-, with reversal of the “smile”. Hydrocephalus may be seen. The midbrain may also be pushed through the tentorial notch. This also pushes the midbrain down. Tonsillar herniation- also called downward cerebellar herniation or "coning", the cerebellar tonsils move downward through the foramen magnum with compression of the lower brainstem and upper cervical spinal cord- cardiac and resp centre compression. Cerebellar tonsils are seen at the level of the dens on axial images or on sagittal images 5mm below foramen magnum in adults. The level of consciousness will decrease with decerebrate positioing then flaccid paralysis. Blood pressure instability is also evident in these patient. Editor: Peter Wyllie POST STROKE MEASURES When a patient presents after a stroke we have a number of goals - Identify those who may be candidates for revascularisation – this may include those who fit the criteria for thrombolysis or other revascularisation procedures such as stenting or embolectomy, or anticoagulation (eg carotid or vertebral artery dissections, venous sinus thrombosis) - Identify and correct precipitants such as anticogulants, malignant hypertension - Supportive management including avoiding hyperthermia, hyper or hypoglycaemia, hyper or hypotension - Avoiding complications such as aspiration pneumonia (with early speech therapy involvement and appropriate feeding). Agents producing short term reductions in brain volume – mannitol or hypertonic saline- head up- inproving venous return with avoiding constricting tiestransient hyperventilation to produce modest reductions in PaCO2 - Surgical – However tying together the issues of herniation as described above and stroke management, the recent AHA/ASA Scientific Statement titled “Recommendations for the Management of Cerebral and Cerebellar Infarction With Swelling- A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Wijdicks E et al. Stroke 2014; published online before print January 30 2014” looked at neurosurgical options for the management of ischaemic strokes. “In swollen supratentorial hemispheric ischemic stroke, routine intracranial pressure monitoring or cerebrospinal fluid diversion is not indicated, but decompressive craniectomy with dural expansion should be considered in patients who continue to deteriorate neurologically. There is uncertainty about the efficacy of decompressive craniectomy in patients ≥60 years of age.” Note a recent study in the NEJM on hemicraniectomy for elderly patients with “malignant “ MCA infarction found that “the proportion of patients who survived without severe disability/ death was 38% in the hemicraniectomy group, as compared with 18% in the control group. However this difference resulted from lower mortality in the surgery group (33% vs. 70%). Of those who survived more had moderate or severe disability. So something to think about. However there are significant issues with pathology which increases the volume and the pressure particularly in the posterior fossa. The brain can only move down through the foramen magnum (with tonsillar herniation) or upwards through the tentorium with upward transtentorial herniation.The surgical option then is to remove the bone in this region with a sub-occipital craniectomy. Getting back to the AHA guideline they add “ In swollen cerebellar stroke, suboccipital craniectomy with dural expansion should be performed in patients who deteriorate neurologically. Ventriculostomy to relieve obstructive hydrocephalus after a cerebellar infarct should be accompanied by decompressive suboccipital craniectomy to avoid deterioration from upward cerebellar displacement. In swollen hemispheric supratentorial infarcts, outcome can be satisfactory, but one should anticipate that one third of patients will be severely disabled and fully dependent on care even after decompressive craniectomy. Surgery after a cerebellar infarct leads to acceptable functional outcome in most patients.” They conclude “Decompressive craniectomy is a necessary option in many patients. Selected patients may benefit greatly from such an approach, and although disabled, they may be functionally independent” Take home point – look for signs of herniation in the stroke patient - consider your options – look at the age, prexisting or expected quality of life , comorbidities , medications etc and look at your options – for some patients, neurosurgical treatment may be an option. Editor: Peter Wyllie . NEXT WEEK’S CASE 25yo lady presents with a painful right ankle (no kidding!) after falling from a moving vehicle–What is going on? Other than needing a different shade of nail polish , what & when does she need done? Post reduction Xrays JOKE / QUOTE OF THE WEEK Walking into ESSU looking for the lady who was re-teaching on the Dragon Voice recognition system, nursing staff were asked “Have you seen the Dragon-lady?” The replied with a straight face “Oh yeh ... Lyndal is in the Acute Area” Please forward any funny and litigious quotes you may hear on the floor (happy to publish names if you want) THE WEEK AHEAD Tuesdays - 12:00 – 13:45 Intern teaching -Thomas & Rachel Moore Wednesday 0800-0900 Critical Care Journal Club. ICU Conf Room / 12.00-1.15 Resident MO in Thomas & Rachel Moore Thursday 0730-0800 Trauma Audit. Education Centre / 0800-0830 MET Review Education centre / 1300-1400 Medical Grand Rounds. Auditorium. Editor: Peter Wyllie