Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
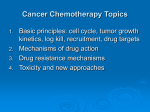
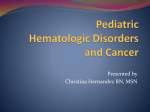
The Child With a Malignancy Jan Bazner-Chandler CPNP,MSN, CNS, RN Developmental and Biologic Variances Most childhood cancers arise for embryonic mesodermal germ layer Involves tissues of: CNS, bone, muscle, endothelial tissue, connective tissue, blood, lymph tissue Grows in a short period of time 80% have metastasis at time of diagnosis Assessment Unusual mass or swelling Unexplained paleness and loss of energy Spontaneous bruising Prolonged, unexplained fever Headaches in morning Sudden eye or vision changes Excessive – rapid weight loss Diagnostic Tests X-ray Skeletal survey CT scan Ultrasound MRI Bone marrow aspiration CBC with absolute neutrophil count Urinalysis Lumbar puncture Urine catecholamines Treatment Modalities Determined by: Type of cancer Location Extent of disease Surgical Management The oldest form of cancer treatment Surgery plays important role in initial diagnosis: biopsy of primary tumor. Excision of tumor when possible Facilitating treatment: insertion of catheters for long-term treatment Radiation Therapy The use of ionizing radiation to break apart bonds within a cell causing cell damage and death. External beam therapy accounts for the majority of radiation treatments in children. Problems: radiation beams cannot distinguish between malignant cells and healthy cells. Chemotherapy Primary treatment modality used to cure many pediatric cancers. Chemotherapy is the use of drugs to destroy cancer cells. The destruction is accomplished by inhibiting cells within the body to divide, which eventually leads to cell death. Chemotherapy Can be given in addition to another form of therapy such as radiation or surgery. Drugs may be administered before surgery to reduce size of tumor. Adjuvant chemotherapy is used after surgery or radiation therapy to prevent relapse. Chemotherapy Combination chemotherapy is the use of more than one class of drug. Administering different classes of chemo drugs ensures a greater chance of achieving complete cancer cell destruction and achieving remission. Administration Chemotherapy can be given by mouth, subcutaneous or intramuscular injections, intravenously, or intrathecally. Oral route used if drug is well absorbed and non irritating to the GI tract Sub-q or IM: Slow systemic release IV push, piggyback or intravenous infusion Goals of Chemotherapy Reducing the primary tumor size Destroying cancer cells Preventing metastases and microscopic spread of the disease Chemotherapy Drugs Alkylating drug: attack DNA Antimetabolites: interfere with DNA production Antitumor antibiotics: interferes with DNA production Plant alkaloids: prevent cells from dividing Steroid hormones: slow growth of some cancers Bone Marrow Transplant HSCT: Hematopoietic Stem Cell Transplant: CHLA has one of the largest program. The option of HSCT depends on the patients disease, disease status, and general physical condition. Involves: Umbilical cord blood Parent’s stem cells Gene Therapy Use of gene therapy in the treatment of childhood cancer is promising yet complex and still in early phases of clinical application. Management Patient / family education Begins at time of diagnosis Continues through treatment phases Maintained in post-survival years Support if death of child Pain Management Pain caused by disease Pain with procedures and treatments Pain associated with side effects of treatment Pain Management Pharmacologic Non-Pharmacologic Sedation or anesthetic medications EMLA cream Conscious sedation Pain Control Immunosuppression and Infection Children with cancer become immune impaired from a number of causes: Lymphocyte production is altered Splenic dysfunction can prevent maturation of blood cells and alteration is inflammatory response. Cancer therapy can decrease immunoglobulin concentrations. Neutropenia Significant neutropenia can develop during chemotherapy creating an increased risk of infection in the child with cancer. Neutropenia occurs when the absolute neutrophil count decreases below 500. Treatment for Neutropenia Granulocyte colony stimulating factor decreases the duration of neutropenia by stimulating the proliferation of the progenitor cells of the granulocytes, specifically the neutophils. G-CSF: 5mcg/kg/day given subcutaneous Varicella If an immunosuppressed child with no history of varicella infection or varicella immunization has direct contact with an individual with chickenpox or shingles, varicella zoster immune globulin should be administered. Acyclovir IV is used in some cases. Varicella Immunizations Three months after chemotherapy Off prednisone Many will have already had the immunization as a toddler since it is now a required immunization. Central Venous Access Devices Two decades ago, CVAD were introduced as an integral part of the pediatric oncology patient’s treatment plan. Used to deliver chemotherapy, blood components, antibiotics, fluids, TPN, medications and blood sampling. CVAD Infection Prevention • • • • Teach family to report signs of catheter infections: fever, chills, swelling, pain, drainage, or erythema. Aseptic technique for dressing changes and heparin flushing. Avoid trauma to device Observe for catheter occlusion Chemotherapy Side Effect Drugs affect not only the cancer cells but also healthy cells. Cells most affected are rapidly growing cells such as hair follicles, reproductive system, bone marrow and gastrointestinal tract. Management of Side Effects Malnutrition Occurs in 8 to 32% of the pediatric oncology population Nutritional goals focus on maintaining normal growth and development as well as preventing nutritional deficiencies. Nutrition Interventions Initial nutritional assessment History of child’s eating habits, food allergies, use of nutritional supplements, base line weight and height measurements. Enteral feedings at night: preserve intestinal mucosa by keeping it functional Nausea and Vomiting Most common side effect of cancer treatment. Chemotherapy-associated vomiting is a reflex controlled by chemoreceptor trigger zone that stimulates the vomiting center in the brain. Tumor location Radiation therapy Anticipatory nausea Interventions Antiemetics such as Phenothiazines: (Trilafon), (Phenergan)and (Thorazine) block dopamine receptors from stimulating the chemoreceptor trigger zones. Serotonin-receptor antagonist such as Granisetron (Kytril) and Ondansetron (Zofran) are very effective. (>3 years) Antihistamines: benadryl Administer before chemotherapy Mucositis Progressive, inflammatory, ulcerative condition of the oral and gastric mucosa. Occurs due to the interruption of cell renewal process of the epithelium leading the mucosal atrophy and ulceration Thrombocytopenia or physical trauma may lead to bleeding and further mucosal damage. Neutropenia and poor dental hygiene predisposes the oral mucosa to secondary infection. Assessment / Interventions Baseline assessment including the oral cavity, teeth, and gingival mucosa. History of dental exam and use of orthodontic appliances Meticulous oral care Mouth rinses Monitor hydration status Constipation Assess normal bowel habits Increase fiber and fluids in diet Stool softeners / colace Physical activity Avoid digital manipulation Diarrhea Assess for signs of dehydration Record stool patterns IV fluids as needed Low-residue or lactose-free diet Good hand washing Hair Loss More important in the older child. Most patients will experience hair loss within 10 days of induction chemotherapy Prepare patient for hair loss Males: shave hair Females: short hair style – pick out wig – scarf - hat Psychosocial Support Support groups Open communication Daily contact with oncology team Trusting relationship with nurse Growth and Development Promote normal G & D Allow decision making Establish daily routines Play therapy Friends School attendance or tutor Late Effects of Cancer Therapy Endocrine: sterility Thyroid Cardiovascular Musculoskeletal Vision Hearing Respiratory Gastrointestinal Genitourinary Hematopoietic Leukemia Most common malignancy Cancer of blood or bone marrow characterized by an abnormal proliferation of blood cells, usually white blood cells (leukocytes) Two types Acute lymphoblastic leukemia: 78% Acute Myelogenous leukemia: 15 to 20% High survival rate Prognosis Initial WBC most significant The higher the count the poorer the outcomes Greater than 100,000 WBC count = poor outcome Children under 2 years and older than 10 Girls do better than boys Diagnosis Peripheral blood smear Bone marrow analysis Lumbar puncture Assessment Pallor and fever Lethargy Anorexia Weight loss Hemorrhage / petechiae Hepatomegly / splenomegaly 3 Phase Treatment Induction: goal is to achieve remission last about a month Consolidation: most intensive phase of chemotherapy lasts 4 to 8 months Maintenance: last two to three years If leukemia cells are detected in bone marrow process is started all over again. Induction Therapy Goal of therapy is to achieve remission Leukemia cells are no longer found in the bone marrow samples, the normal cells return and blood counts become normal. Drugs used: L-asparaginase, vincristine and a steroid (dexamethasone), for high-risk children a fourth drug (daunorbucin) is often used Consolidation Phase Several drugs are used in combination to prevent remaining leukemia cells from developing resistance. Drugs include: methotrexate and 6-mercaptopurine, vincristine and prednisone Maintenance If leukemia continues to be in remission maintenance therapy can be started. Two drugs: vincristine and steroids over a brief period every 4 to 8 weeks. Duration of total therapy 2 to 3 years. CNS Therapy CNS prophylaxis is initiated at diagnosis and is used to reduce the risk for CNS disease. Preventive CNS is based on the premise that the CNS provides a sanctuary site for leukemic cells that are undetected at diagnosis and reside protected from the action of systemic therapy by the brain blood barrier. Multidisciplinary Interventions Assess for infection Monitor blood values I & O / nutrition Complications of chemotherapy Good hand washing Aseptic technique for blood draws Leukemia Time Line 1962 cure rate for pediatric cancer is 4 %. 1971 – A combination of chemotherapy and cranial irradiation proves it can cure at least half of all children with ALL. 1975 – A new combination of chemo drugs helps patients with reocurrence of the disease. 1991 Long-term survival rate increases to 73% with intensive induction therapy followed by two years of treatment with eight anti cancer drugs used on a rotating basis Time Line 1997 – Bone marrow transplants from unrelated, genetically matched donors are effective against many childhood leukemia's. 1998 – survival rate 73% to 80%. 2004 – survival rate 85% 2006 – survival rate 94% CNS Tumors • • • 2nd most common malignancy 65% have 5 year survival rate Most common tumors: • • • Astrocytomas 50% Medulloblastomas 25% Brain stem gliomas 10% Assessment Classic signs and symptoms are indicative of increased intracranial pressure. Pressure is due to tumor mass compressing vital structure, blockage of cerebrospinal fluid flow or tumor associated edema. Gait changes / ataxia Headache with or without vomiting Blurred vision, or diplopia Forceful vomiting upon rising in the morning or papilledema. Multidisciplinary Interventions Surgery if tumor accessible Chemotherapy Radiation = Reserved for patient older that 2-years of age Survival rate based on location Chemotherapy After surgery to prevent tumor from coming back Shrink tumor that cannot be operated on Shrink tumor so it can be operated on Chemotherapy Blood brain barrier – natural filter within the body that allows certain substances through from the blood to the brain tissues. Drugs used are: temozolamide, procarbazine or lomustine Methotrexate is injected intra-thecal Implantable wafers: drug is fixed with gel wafer – drug is slowly released into brain over 2 to 3 weeks Brain Tumors Astrocytoma Large right frontal lobe neoplasm with small area of necrosis Hodgkin's Disease 3rd most common malignancy 15 to 30 years Three times higher in males Excellent cure rates Assessment Night sweats Weight loss Malaise Painless, firm nodes Treatment Radiation to nodes Chemotherapy Combination therapy for six months Prednisone Stem cell transplant Neuroblastoma Approximately 600 new cases a year. Embryonic tumor Average age of diagnosis is 2 years. Poorest survival rate 50 to 60% have metastases at time of diagnosis. Assessment Depends on site of tumor Diagnosis CT scan Bone scan 95% secrete catecholamines in the urine. Multidisciplinary Interventions Determined by the stage of disease and age of child. Children who have localized disease and complete response to treatment are more likely to achieve a disease free state and long-term survival. Neuroblastoma Wilm’s Tumor Most common type of renal tumor in children Approximately 460 new cases each year. Children with hypospadius or cryptorchidism have a slightly higher incidence. African American and Females at highest risk Assessment Firm non-tender, painless mass in abdomen Hematuria Hypertension Do not palpate the abdomen CT Scan Wilm’s Tumor Wilm’s Tumor Multidisciplinary Interventions Surgery Nephrectomy Prevent rupture of capsule Sample for pathology Chemotherapy and radiation are given based on the stage of the disease. Osteogenic Sarcoma Malignant tumor of bone Peak incidence between ages 10 and 20 years Genetic predisposition Approximately 20% have metastases at diagnosis High rate of metastasis to lungs Assessment Pain in affected limb that increases with activity or weight bearing Refusal to walk and limited range of motion Tenderness and edema Diagnosis often made after traumatic injury Diagnosis Multidisciplinary Interventions Limb salvage Amputation Chemotherapy Limb Salvage http://www.clevelandclinic.org/ortho/tumor/limbSalvageLg.htm Ewing Sarcoma Tumor of flat bones Pelvis, chest, vertebrae Rare in children under 5 years 75% diagnosed by age 20 Ewing Sarcoma Rhabdomyosarcoma Most common soft bone tissue tumor Head and neck 40% GU 20% Extremities 20% Trunk 15% Prognosis Location Extent of disease Children with no detectible metastases at time of diagnosis have better outcomes Head and neck tumors have better prognosis 72% survival rate after 5 years Multidisciplinary Interventions Biopsy of tumor mass Imaging studies Surgical removal Chemo based on tissue biopsy Radiation Retinoblastoma Intraocular tumor composed of embryonal retinal cells 1 in 16,000 + family history High incidence of malignancies Assessment Child may initially present with strabismus Impaired vision Creamy white pupillary reflex Painful eyes from inflammation Retinoblastoma Pupil reflex “Cat Eyes” Multidisciplinary Interventions Surgical enucleation of eye Genetic counseling Follow-up care up to 18 Years