Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
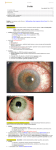
Uvea & Sclera SINA A. SHOOL MD www.drsinashool.blogspot.com Uveitis – “inflammation of the uveal tract” 1) Anatomic classification Anterior Uveitis: iris & Anterior part of the ciliary body (pars plicata Intermediate Uveitis: posterior part of the ciliary body (pars plana) Posterior Uveitis Panuveitis Anatomical - Anterior Uveitis Juvenile Rheumatoid Arthritis Fuchs’ heterochromic Iridocyclitis Ankylosing Spondylitis Reiter’s Syndrome Anatomical Intermediate Uveitis Pars Planitis Sarcoidosis Multiple Sclerosis Lyme Disease Anatomical - Posterior Uveitis Toxoplasmosis Histoplasmosis Toxocariasis Serpiginous chorioretinitis Birdshot retinochoroiopathy Anatomical - Diffuse Uveitis Sympathetic Ophthalmia VKH syndrome Behcet’s disease (2) Clinical Classification Acute Uveitis: sudden, symptomatic onset; persists for <6 weeks Chronic Uveitis: insidious onset, may be asymptomatic; persists for months (3) Etiological Classification Exogenous Uveitis: due to external injury to the uvea or invasion of microorganisms from the outside Endogenous Uveitis: caused by microorganisms or other agents from inside the patient www.drsinashool.blogspot.com (4) Pathological Classification Granulomatous Uveitis - epithelioid and giant cells, lymphocytes Non-granulomatous Uveitis - lymphocytes and plasma cells (5) Pathophysiologic Mechanisms (Opremcak) Traumatic – Surgical vs. non-surgical Infectious – Bacterial, Viral, Fungal, Protozoal, Helminthic, Insect, Animal Immunologic Masquerade Diseases Immunologic Type I hypersensitivity disorders – Ig E- mediated – Mostly ocular surface disease hay fever, vernal & atopic keratoconjunctivitis Type II – Antibody dependent cellular cytotoxicity (autoantibodies) – Ocular Cicatricial Pemphigoid; Lensinduced Uveitis Immunologic Type III – Immune Complex formation & deposition – Ankylosing Spondylitis, SLE, JRA, Behcet’s disease, PAN, Wegener’s granulomatosis, inflammatory bowel disease, other collagen vascular diseases Type IV – Cell mediated immune response – Interleukins – Contact dermatitis, Phylectnulosis, , Fuchs HI, Sympathetic Ophthalmia, VKH, Birdshot retinochoroidopathy, Pars Planitis, Leber’s Idiopathic Stellate Neuroretinitis, Sarcoidosis Antigen HLA-A1 HLA-A11 HLA-A29 HLA-B51 HLA-B7, DR2 HLA-B8 HLA-B12 Disease Relative Risk Sarcoidosis Sympathetic Ophthalmia Birdshot 50-224 Retinochoroido pathy (>97%) Behcet’s Disease 4-6 POHS 12 Anterior Uveitis 5 Behcet’s 3-4 Disease(oral) OCP Antigen HLA-B27 HLA-B53 Disease Relative Risk Ankylosing 100 Spondylitis (90%) Reiter’s syndrome 40 (76%) Acute Anterior 10 Uveitis (55%) Inflammatory Bowel Disease Psoriatic Arthritis Bechet’s Disease VKH, 75 glaucomatocylitic 75 uveitis Masquerade Syndrome Vascular tumors Infectious Congenital anomalies Metabolic/Degenerations (amyloidosis, retinitis pigmentosa) Neoplastic Disease (lymphoma, leukemia) Clinical Features Anterior Uveitis Symptoms Photophobia, pain, redness, decreased vision (Acute) *Minimal symptoms in chronic type Signs Circumcorneal injection Keratic precipitates (cellular deposits on the corneal endothelium) Iris nodules: Koeppe & Busacca Aqueous cells Aqueous flare: leakage of proteins Posterior synechiae Grading System for Anterior Chamber Flare & Cell Aqueous Flare 0 Optically empty 1+ Faint 2+ Moderate- clear iris & lens 3+ Marked- hazy iris & lens 4+ Intense- fibrin with no motion of cells Aqueous cell (1x3 mm beam @ 5-10 °) 0 0 Rare Rare Occasional 1-2 cells Trace 2-4 cells 1+ 5-15 2+ 16-25 3+ 26-60 4+ > 60 cells Limbal Hyperemia= Intraocular Inflammation Clinical Features Intermediate Uveitis Symptom Floaters s Decreased vision (if with CME) Signs Vitritis: cellular infiltration of the vitreous +Vasculitis + few cells in the anterior chamber Grading System for Vitreous Cell and Opacification Flare (Vitreous Opacification) 0 Good View of NFL 1+ Clear ON & vessels but hazy NFL 2+ ON & vessels hazy 3+ ON only 4+ No ON Cell (1x3 mm beam in anterior vitreous) Trace 0-10 cells 1+ 10-20 2+ 20-30 3+ 30-100 4+ > 100 cells Clinical Features Posterior Uveitis Symptoms Floaters and decreased vision Signs Cells, flare, opacities in the vitreous Choroiditis: yellow or greyish patches Retinitis: whitish, cloudy retina Vasculitis Phlebitis (veins); Arteritis (arterioles) Keratouveitis: with corneal involvement Sclerouveitis: with scleral involvement Keratosclerouveitis Anterior Uveitis Juvenile Rheumatoid Arthritis Fuchs’ heterochromic Iridocyclitis Ankylosing Spondylitis Reiter’s Syndrome Anterior Uveitis 1) Uveitis Associated with Joint Disease a) Juvenile Rheumatoid Arthritis (JRA) - chronic, bilateral, non-granulomatous - arthritis of at least 3 mos’ duration in a child less than 16 years - females - insidious onset - uveitis may precede the onset of arthritis JRA (cont) - types of arthritis: pauciarticular onset <4 joints polyarticular onset systemic onset > 5 joints Anterior Uveitis 2) Uveitis Associated with Joint Disease(cont) b) HLA-B27-associated - Ankylosing spondylitis - Reiter’s syndrome - Psoriatic arthritis - Inflammatory Bowel Disease (IBD) HLA-B27-associated Ankylosing Spondylitis inflammatory arthritis affecting axial skeleton Fixed flexion deformity due to fusion of spine and sclerosis of sacroiliac joints Klebsiella & Chlamydial infections HLA-B27-associated Reiter’s Disease - Triad: urethritis, conjunctivitis, arthritis - Extraarticular features: Mouth ulcers, skin lesions (keratoderma blenorrhagica), penile lesions (circinate balanitis), nail changes, cardiovascular changes, genitourinary lesions HLA-B27-associated Psoriatic Arthritis - Psoriasis: skin disease due to epidermal hyperproliferation HLA-B27-associated Inflammatory bowel disease - Crohn’s disease and ulcerative colitis - Gastrointestinal and articular manifestations - Systemic manifestations include skin lesions, oral ulcerations, hepatobiliary disorders, urogenital involvement Anterior Uveitis 3) Fuch’s Heterochromic Iridocyclitis - unilateral, insidious, third or fourth decade - No symptoms; low grade uveitis - Early cataract - Fine, stellate, evenly distributed deposits on the posterior corneal surface; iris atrophy; telangiectatic vessels in the angle - Synechiae is rare Fuch’s Heterochromic Iridocyclitis Anterior Uveitis 4) Herpetic Uveitis - unilateral, high IOP, decreased corneal sensation, iris atrophy - Herpes simplex, Herpes zoster - Treatment: oral anti-herpetic (acyclovir), topical steroids, + anti-glaucoma *posterior pole involvement: acute retinal necrosis (ARN) Posterior Uveitis - - 1) 2) 3) 4) usually associated with systemic disease Clues that can guide: Morphology of the lesion Age of the patient Unilateral/Bilateral Course of the disease Posterior Uveitis 1) - - Ocular Toxoplasmosis Toxoplasma gondii, obligate intracellular protozoan Most common cause of posterior uveitis in U.S. Domestic cat definitive hosts Treatment: pyrimethamine, sulfadiazine, clindamycin, trimethoprim/sulfamethoxazole + steroids Posterior Uveitis 2) Ocular Toxocariasis - Toxocara canis, intestinal parasite of dogs - Young children - Infection by pica or close contact with puppies - Usually unilateral - Inflammation is caused by death of the larvae in the retina 3) CMV retinitis - opportunistic infection usually found in AIDS patients - Retinal necrosis - IV ganciclovir or foscarnet; intravitreal ganciclovir 4) Adamantiades-Behcet’s Disease - idiopathic multisystem disorder - Pathology: widespread vasculitis - Triad: recurrent ocular inflammation, skin lesions, recurrent oral & genital ulcers Panuveitis 1) Sympathetic Ophthalmia rare, granulomatous, bilateral Follows a perforating eye injury, or surgery Probably due to hypersensitivity to pigment-bearing cells in the uvea Sympathetic Ophthalmia - - - Injured (exciting eye) becomes inflammed followed by fellow (sympathizing) eye Early enucleation of exciting eye (within 10 days from injury) Advanced cases: systemic steroids or chemotherapy Histopathology Dalen Fuchs’ Nodule Granulomatous Inflammation of Choroid Panuveitis 2) Tuberculous Uveitis - can occur even without pulmonary involvement - Nodules; no specific findings - Tx: antituberculosis drugs Panuveitis 3) Vogt-Koyanagi-Harada - systemic disorder involving multiple organ systems: - Ocular (panuveitis, exudative RD, optic disc hyperemia) - Auditory (tinnitus, deafness) - Nervous (headache, meningismus, CSF lymphocytosis) - Integument (alopecia, poliosis, vitiligo) VKH - autoimmunity to melanocytes in the uveal tract and integumentary system possible Areas of choroid retinal adhesions with focal proliferation of the retinal pigment epithelium. Lymphocytic infiltrates and edema are noted throughout the detached choroid Poorly defined nests of epithelioid cells present throughout the thickened choroid with a moderate lymphocytic infiltrate 4) Syphilis - great imitator - No pathognomonic signs Complications of Uveitis - - Band Keratopathy calcium deposition in anterior layer of the cornea (Bowman’s layer) Treatment: ethylenediaminetetraacetic acid (EDTA) Complications of Uveitis Synechiae -Peripheral anterior synechiae impede aqueous outflow: glaucoma -Posterior synechiae Seclusio pupillae: 360 posterior synechiae forward bulging of the iris due to fluid accumulation (iris bombe) glaucoma Complications of Uveitis Cataract -Interference with lens metabolism or steroids -Eye should be quiet for at least 3 months before undergoing cataract extraction -not all patients can tolerate IOL implantation Complications of Uveitis Retinal scars Central vision may be spared if the macula has not been involved Peripheral scars may cause scotomas Complications of Uveitis Retinal Detachment Tractional: Result of traction on the retina by vitreous strands Serous: Fluid accumulation under the retina Complications of Uveitis Cystoid Macular Edema Accumulation of edema fluid in spaces in the outer plexiform and inner nuclear layers Complications of Uveitis Optic atrophy Complications of Uveitis Hypotony Due to proliferation of exudates in the ciliary body Diagnosis Differential-based Diagnostic System – Acquistion of facts – Evaluate – Listing of Hypotheses – Selection among hypotheses Laboratory Testing – Routine Tests CBC with differential ESR/CRP VDRL/FTA-ABS – Frequently Obtained Chest X ray ACE/lysozyme ANA/RF/ANCA Skin Testing Diagnosis Specific Tests – Blood Tests Autoantibodies Specific serologies Serum proteins – Radiologic Tests Chest Radiography Sacroiliac and lumbosacral spine Gallium scan MRI CT Specific Tests – FA – Tissue Biopsy – Ultrasonography Treatment 1. 2. 3. Aims of therapy: To prevent vision-threatening complications To relieve the patient’s discomfort To treat the underlying cause Treatment Four types of medications: 1) Mydriatics 2) Steroids 3) NSAIDs 4) Immunosuppressive medications Specific Strategies for Uveitis Type I: Eliminate agents, cromolyn, antihistamine, corticosteroids Type II: Dapsone, corticosteroids, cytotoxic agents, surgical removal Type III: NSAIDS, corticosteroids, immunosuppressive and cytotoxic agents, plasmapheresis Type IV: corticosteroids, immunosuppressive and cytotoxic agents, cyclosporine Treatment 1) Mydriatics To give comfort by relieving spasm of the ciliary muscle Atropine 1%, Tropicamide, Cyclopentolate To prevent formation of posterior synechiae To break synechiae Treatment 2) Steroids a) Topical steroids: only for anterior uveitis Prednisone, prednisolone, dexamethasone Usually start with a high rate of instillation and decrease as inflammation lessens Complications: glaucoma, posterior subcapsular cataract, corneal complications, systemic side effects Treatment 2) Steroids (cont) b) Periocular injections Able to reach therapeutic concentration behind the lens Longer lasting effect with depot Triamcinolone acetonide 40mg/ml Methylprednisolone acetate 80 mg/ml Treatment 1) 2) 3) 4) 5) Indications for periocular steroids: Severe anterior uveitis Resistant cases of anterior uveitis Intermediate uveitis Poor patient compliance Cystoid macular edema Treatment 2) Steroids (cont) c) Systemic steroids (oral or intravenous) Corticosteroids Adverse Reactions Cushingoid changes (moon facies, weight gain, fat redistribution, and increased acne) Delay of pubertal growth in children below 15 Infection, hypertension, fluid retention, diabetes mellitus, hyperlipidemia, atherosclerosis, osteoporosis, glaucoma and cataracts Anxiety, sleeplessness, mood changes, easy bruising, poor wound healing Pancreatitis, aseptic necrosis of bone, myopathy, psychosis 2) Steroids (cont) d) Intravitreal steroids Treatment 3) Non-Steroidal Anti-Inflammatory agents (NSAIDs) Flurbiprofen – effective in CME Treatment 4) Immunosuppressive Drugs Indications: When systemic corticosteroids are insufficient to control the disease Steroid side effects Long term use of steroids at a high dose to suppress the inflammation Immunosuppressive Drugs Antimetabolites Azathioprine (Imuran) Methotrexate (Rheumatrex) Mycophenolate mofetil (Cellcept) T-cell inhibitors Cyclosporine (Sandimmune; Neoral) Tacrolimus (Prograf) Alkylating agents Cyclophosphamide (Cytoxan) Chlorambucil (Leukeran) Common Ophthalmic Indications for Cytotoxic Immunosuppression Type I: Autoimmune diseases: few Type II: OCP, severe lens-induced uveitis Type III: Autoimmune/collagen vascular associated disease: Bechet’s disease, PAN, Wegener’s granulomatosis, SLE, rheumatoid arthritis Type IV: Autoimmune diseases: SO, VKH, birdshot retinochoirodopathy, pars planitis Immunosuppressive Usage & Side Effects DRUG SIDE EFFECT Methotrexate Liver damage & mucosal lesions Cyclophosphomide Bone Marrow, bladder, lung CHOICE OF DRUG FOR Reiter’s Syndrome & Severe Rheumatoid Arthritis OCP, Behcet’s, PAN, relapsing polychondritis, Wegener’s granulomatosis, VKH, Serpigenous chorioretinopathy, SO Immunosuppressive Usage & Side Effects DRUG SIDE EFFECT Azothioprine Blood dyscrasia Methotrexate Mucosal ulcerations, GI disturbances, hepato & myelo toxicity, infection Nephrotoxicity Cyclosporin CHOICE OF DRUG FOR Wegener’s, OCP, JRA Rheumatoid scleritis, Ankylosing, Reiter’s, SLE, JRA-associated iridocyclitis Bilateral sight threatening conditions: Birdshot, SO, VKH, Behcet’s Serpigenous Malignancies of the Uveal Tract Sclera Dense connective tissue that encloses about five-sixths of the eye - Functions: Strength and firmness maintains the shape of the globe Aids in the maintenance of intraocular pressure Provides attachment for the extraocular muscles Protects intraocular structures from trauma and mechanical displacement - Sclera 1) 2) 3) Layers of the Sclera Episclera Scleral Stroma Lamina fusca Sclera 1) - - - Episclera forms the superficial aspect of the sclera and merges with the underlying scleral stroma Consists of loosely arranged bundles of collagen, intermingled with fibroblasts, occassional melanocytes, proteoglycans, and gylcoproteins. Rich blood supply mainly from the anterior ciliary arteries Sclera Episcleritis - a benign inflammatory disease characterized by edema and cellular infiltration of the episcleral tissue - self-limited; recurrent; rarely leaves any residual ocular damage - Idiopathic in 2/3 of cases Sclera Episcleritis - main symptom is mild discomfort - Main sign is redness which may be localized or involve the whole episclera Sclera 2) Scleral Stroma - consists of collagen bundles associated with few elastic fibers 3) Lamina Fusca - portion of the sclera adjacent to the uvea Sclera - - - Scleritis Severe inflammatory condition characterized by edema and inflammatory cell infiltration of the sclera May be progressively destructive with loss of vision Pain, tender globe, deep violaceous discoloration of the globe due to dilation of deep vascular plexus of the sclera and episclera Associated with systemic disease Sclera Clinical classification of episcleral and scleral inflammation Episcleritis Simple Nodular Scleritis Anterior scleritis Diffuse scleritis Nodular scleritis Necrotizing scleritis Posterior scleritis Sclera Disease associated with episcleritis and scleritis Diagnosis % of patients with associated disease Episcleritis 31.91% Simple 28.21% Nodular 50.00% Scleritis 56.98% Diffuse 45.45% Nodular 43.59% Necrotizing 94.87% Posterior 45.45% THANK YOU Thank You www.drsinashool.blogspot.com