Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
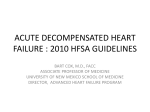
Case-based review Management of Acute Decompensated Heart Failure in Hospitalized Patients Carlos E. Sanchez, MD, and David R. Richards, DO Abstract • Objective: To review the current in-hospital management of patients with acute decompensated heart failure (ADHF). • Methods: Review of the literature. • Results: Heart failure is a leading cause of hospitalization in the elderly, and morbidity, mortality, and hospital readmission rates for ADHF remain high. The patient’s hemodynamic status along with the use of prognostic models for short-term mortality may facilitate patient triage and encourage the use of evidence-based therapy, especially in high-risk patients. Initial treatment should target the relief of congestive symptoms, and intravenous loop diuretics are the mainstay of therapy. The preferred IV vasoactive medication has yet to be determined in a large prospective randomized trial. Positive inotropic agents should be reserved for patients with signs of low cardiac output and tissue hypoperfusion; however, the risk/benefit equation should be evaluated judiciously with each treatment option before initiating therapy. For patients with refractory hemodynamic collapse, ventricular assist devices can allow stabilization until recovery or decision regarding transplantation versus destination therapy. • Conclusion: Patients with ADHF are at increased risk for readmission to the hospital as well as at increased risk for death. Risk factors need to be identified and referral to a heart disease management program should be considered for those patients deemed at increased risk for rehospitalization. H eart failure is a major public health problem in the United States and the leading cause of hospitalization in patients 65 years of age and older [1]. Patients hospitalized with acute decompensated heart failure (ADHF) have a readmission rate as high as 50% within 6 months and 25% within 30 days [2]. It is estimated that $32 billion is spent on heart www.jcomjournal.com failure care each year, the majority of which is directly related to inpatient care. Projections show that by 2030 the total cost of heart failure will increase to $70 billion per year [1]. Despite the growing burden, advances in treatment have been limited [2,3] and management continues to be a challenge. In this article, we review the current in-hospital management of patients with ADHF. CASE STUDY Initial Presentation A 64-year-old woman with a nonischemic dilated cardiomyopathy presents to the emergency department (ED) with a 4-day history of progressive dyspnea on exertion. She can not ambulate more than 50 feet without having to stop due to dyspnea and reports increased lower extremity edema. She is found to have a heart rate of 105 bpm, a respiratory rate of 30 breaths/min, and a blood pressure of 90/51 mm Hg. Physical examination is remarkable for distended neck vein, S3 gallop, end expiratory wheezing in the bases, and lower extremity edema. Blood tests, including a B-type natriuretic peptide level, are pending. Electrocardiogram and chest radiograph are ordered. The physician suspects that the patient has ADHF and admits her for further management. • What are aspects of initial management in the ED? Most patients that present for evaluation and management of ADHF are first evaluated in the ED. Initial management includes an assessment of oxygenation, hemody- From Ohio Health, Riverside Methodist Hospital, Columbus, OH. Vol. 22, No. 4 April 2015 JCOM 179 Acute Decompensated Heart Failure Evidence for Congestion (Elevated Filling Pressure) Orthopnea High jugular venous pressure Increasing S3 Loud P2 Edema Ascites Rales (uncommon) Abdominal reflux Valsalva square wave Evidence for Low Perfusion Narrow pulse pressure Pulsus alterations Cool forearms and legs May be sleepy, obtunded ACE inhibitor-related symptomatic hypotension Declining serum sodium level Worsening renal function Low perfusion at rest? Congestion at rest? No Yes No Warm and dry Warm and wet Yes Cold and dry Cold and wet Figure. 2 × 2 table of hemodynamic profiles in patients with heart failure. Reprinted from Nohria A, Lewis E, Stevenson LW. Medical management of advanced heart failure. JAMA 2002; 287:628–40. namic status, and adequacy of tissue perfusion, as well as for possibility of an acute coronary syndrome. A complete history, physical examination, chest radiography, 12-lead electrocardiogram, cardiac troponin T or I, electrolytes, and complete blood count should be obtained to allow rapid diagnosis and triage followed by prompt, aggressive treatment in the ED or observation unit. This should allev-iate the patient’s symptoms sooner, and it is intuitive that this would lessen morbidity and length of hospital stay [4]. • How are patients with ADHF classified? ADHF denotes the development of progressive signs and symptoms of distress that require hospitalization in patients with a previous diagnosis of heart failure. The American College of Cardiology Foundation/American Heart Association (ACCF/AHA) guideline for the diagnosis and management of heart failure in adults notes that the hospitalized patient with heart failure can be classified according to adequacy of systemic perfusion and volume status [5]. Most patients can be classified 180 JCOM April 2015 Vol. 22, No. 4 during bedside assessment according to the diagram shown in the Figure. Patients with fluid overload who present with adequate peripheral perfusion and signs and symptoms of congestion and are classified as “warm and wet.” Patients without congestion but with low output with evidence of tissue hypoperfusion due to heart failure are “cold and dry,” and display a continuum of severity manifested by hypotension, renal insufficiency and/or shock. Patients with fluid overload and tissue hypoperfusion or shock are “cold and wet” [5]. Although these clinical profiles differ in their prognostic significance, clinicians should recognize the need for urgent therapy based upon clinical signs and symptoms [6]. Specifically, cold and wet patients may need observation in the cardiac care unit setting, and treatment should be directed at improving tissue perfusion and relieving congestion. The ACCF/AHA guideline also classifies hospitalized patients with ADHF into subgroups with distinct clinical and hemodynamic characteristics that require special attention. These include patients with acute coronary ischemia, accelerated arterial hypertension in patients with signs and symptoms of heart failure, shock, and acutely worsening right heart failure (Table 1) [5]. www.jcomjournal.com Case-based review Table 1. Clinical Classification of Hospitalized Patients with Acute Heart Failure Based on ACCF/AHA Guidelines [5] and Clinical Presentation with Management Considerations Clinical Classification Sign and Symptoms of ADHF Management Considerations Based on Clinical Presentation Variable: None to pulmonary congestion or acute pulmonary edema 15% of patients with ACS have symptoms of heart failure ADHF frequently associated or precipitated by bradycardia, atrial fibrillation, and ventricular tachycardia Coronary angiography Revascularization: PCI/CABG Signs and symptoms of HF accompanied by accelerated hypertension Relatively preserved LV systolic function Low hospital mortality Frequent pulmonary congestion/acute pulmonary edema without systemic congestion Euvolemic or mild hypervolemic Tachycardia Hypertension due to increased sympathetic tone (vasoconstriction) Vasodilators Diuretics: with volume overload or pulmonary edema Evidence of tissue hypoperfusion induced by HF after correction of preload and major arrhythmias Rapid development of pulmonary congestion/edema SBP < 90 mm Hg or drop of MAP > 30 mm Hg Oliguria Evidence of organ hypoperfusion Arrhythmias are common Positive inotropes Norepinephrine or dopamine: If the inotropes fail to restore SBP and signs of organ hypoperfusion persist Mechanical circulatory support Peripheral edema Increased JVP ± Hepatomegaly Low left ventricular filling pressures Avoid mechanical ventilation Inotropes: with signs of organ hypoperfusion ± Diuresis Evaluate PE and RV myocardial infarction as the cause Characteristics Congestion Acute coronary ischemia and heart failure ADHF with clinical, laboratory and/or ECG evidence of acute coronary syndrome Accelerated hypertension with acute heart failure Cardiogenic shock Acute isolated right heart failure Low output syndrome in the absence of pulmonary congestion No pulmonary congestion Mechanical circulatory support Treat arrhythmias Evaluate systolic and diastolic ventricular function, valvular function or mechanical complications with echocardiography Intubation ADHF = acute decompensated heart failure; ACS = acute coronary syndrome; BP = blood pressure; CABG = coronary artery bypass graft; ECG = electrocardiogram; HF = heart failure; JVP = jugular venous pressure; LV = left ventricle; MAP = mean arterial pressure; PCI = percutaneous coronary intervention; PE = pulmonary embolism; RV = right ventricle; SBP = systolic blood pressure. • What risk assessment tools are available? B-type natriuretic peptide (BNP) and N-terminal fragment proBNP (NT-proBNP) were recently validated as diagnostic aids for the differentiation of etiologies of dypnea in patients in the ED with possible symptoms of ADHF. Use of these biomarkers can help reduce diagnostic uncertainty and associated mismanagement of patients presenting with nonspecific symptoms of dyspnea [4,5,7]. Low or normal levels (BNP < 100 pg/ml or NT-proBNP < 500 pg/ml) have a high negative predictive value for excluding heart failure. www.jcomjournal.com Elevated BNP or NT-proBNP levels may also yield prognostic information, identifying patients at increased risk of mortality or rehospitalization when value does not fall after aggressive heart failure management [8,9]. In a recent study by Fonarow et al, the levels of BNP on hospital admission correlated directly with the risk of in-hospital mortality in patients admitted with ADHF independent of left ventricular ejection fraction. When the levels of BNP were below 430 pg/ml, the in-hospital mortality was 1.9%, and when the levels were above 1730 pg/ml, the mortality went up to 6% (P < 0.001) [8]. Additionally, elevated predischarge BNP levels (BNP > 350 ng/l; P < 0.001) in patients with ADHF seem to identify those at increased risk of death or readmission after in-patient management [9]. Vol. 22, No. 4 April 2015 JCOM 181 Acute Decompensated Heart Failure Table 2. In-hospital Mortality Predictor Models in Patients Presenting with ADHF Predictor Model Number of Patients AHA Get With the GuidelinesHeart Failure [12] 39,783 ADHERE [13] 65,275 Derivation and validation cohort OPTIME-CHF [14] 949 EFFECT [15] 4031 Optimize-HF [16] 48,612 Best Predictors for Mortality Mortality Risk Comments Older age SBP BUN In-hospital mortality rates varied by deciles ranging from 0.4% to 9.7% with a predictive risk variation of >24-fold across deciles The probability of in-hospital mortality is estimated by summing points assigned to the value of each predictor with a validated tool for risk stratification. BUN > 43 mg/dL Admission SBP < 115 mm Hg Creatinine > 2.75 mg/dL In-hospital: 4.2% Admission SBP ≥ 115 mm Hg had lower mortality risk High BUN 60-day mortality: 9.6% Increased SBP and serum sodium had lower mortality Older age Respiratory rate Hyponatremia < 136mEq/L Increased BUN Comorbid conditions (eg, dementia) In-hospital: 8.9% 30-day: 10.7% 1-year: 32.9% Higher SBP (per 10-unit increase) had lower mortality Serum creatinine Admission SBP Patients age In-hospital: 3.8% In-hospital mortality increased 18% for every 0.3 mg/dL increase in SCr up to 3.5 mg/dL Every 10-year increase in age was associated with a 34% higher risk for inhospital mortality Higher admission SBP was associated with a lower risk of in-hospital mortality (up to 160 mm Hg) NYHA class IV Increasing age (per 10-year increase) Low SBP Low serum sodium AHA = American Heart Association; BUN = blood urea nitrogen; NYHA = New York Heart Association; SBP = systolic blood pressure; SCr = serum creatinine. (Modified from reference 50.) Elevated cardiac troponin T or I in hospitalized patients with ADHF also are associated with increased mortality, including in those without acute coronary syndrome or underlying coronary artery disease [10,11]. The American Heart Association Get With The Guidelines–Heart Failure (GWTG-HF) developed a validated risk score to predict in-hospital mortality in 182 JCOM April 2015 Vol. 22, No. 4 patients hospitalized for heart failure that uses commonly available clinical variables. The admission variables that were most predictive of in-hospital mortality were BUN, systolic blood pressure, and age [12]. In addition, Fonarow et al published a detailed in-hospital mortality risk stratification tool for ADHF derived from more than 65,000 patients in the ADHERE registry database [13]. www.jcomjournal.com Case-based review Of 39 variables, high admission BUN level (≥ 43) was the best single predictor for mortality, followed by an admission systolic blood pressure less than 115 mm Hg and a serum creatinine level above 2.75 mg/dL. These variables underscore the importance of renal function as a predictor of cardiac outcomes among hospitalized patients with ADHF. Other risk stratification models and predictors of mortality in hospitalized patients with ADHF have recently been published (Table 2) [12–16]. These predictor models emphasize the importance of early identification of high-risk patients, which may allow for focusing intensity of care where it is most needed. Prospective studies will be needed to determine to what degree risk stratification may improve outcomes. Case Continued Upon further evaluation by a cardiologist, the patient is cool and clammy with elevated neck veins and prominent S3 confirmed. She continues to report severe shortness of breath after 1 dose of intravenous (IV) furosemide in the ED. Repeat vital signs shows a blood pressure of 83/49 mm Hg and respiratory rate of 33. Her electrocardiogram shows sinus tachycardia. The cardiologist determines that the patient’s clinical profile is “cold and wet” and admits the patient to the cardiac care unit (CCU) with a diagnosis of ADHF. Initial blood tests show a BNP level of 1830 pg/ml, troponin I is 0.63 and stable after 2 measurements, serum creatinine is 1.6 mg/dL, BUN is 44 mg/dL, and serum sodium is 132 mg/dL. The GWTG-HF risk score for inhospital mortality was calculated based on admission data and the probability of death was estimated at > 5% to 10% [12]. Prompt aggressive medical therapy was instituted in the CCU consisting of furosemide infusion to reduce congestion and IV dobutamine to improve systemic perfusion. Enoxoparin 40 mg subcutaneously once daily was initiated for venous thromboembolism prophylaxis. • What are important aspects of therapy for ADHF? Elevated filling pressure is the culprit in the development of most of the signs and symptoms of ADHF and is the target for treatment. An important aspect in the management of ADHF is identifying precipitating factors and/or comorbid conditions (Table 3) and treating them appropriately in conjunction with volume overload [5]. Echocardiogram is a widespread and readily available diagnostic tool providing important information on systolic and diastolic ventricular function as well as other structural heart disease abnormalities. Additionally, myocardial ischemia evaluation with noninvasive testing or cardiac catheterization should be performed if ischemia is a potential contributor to the patient’s heart failure symptoms. The most common cause of heart failure readmission is noncompliance with medications or dietary restrictions. Hospitalization provides an opportunity to educate the patient about their condition and rationale for therapy as well as identify barriers to appropriate self-management. Although use of vasoactive medications such as nitroglycerin or nitroprusside are not routinely recommended for use in all ADHF patients admitted to the hospital, retrospective analysis of the ADHERE database suggests that there is a significant reduction of mortality, hospital length of stay, admission to intensive care unit, invasive procedures, and prolonged hospitalizations when IV diuretics, vasodilators (nitroglycerin, nitroprusside, nesiritide,) and/ or positive inotropes (milrinone, dobutamine) are initiated in the ED within 6 hours of an ADHF presentation [18,19]. However, whether prompt ED intervention impacts intermediate- to long-term outcomes is unknown [4]. Hospitalized patients with ADHF are at increased risk of venous thromboembolism mainly due to reduced cardiac output, increased systemic venous pressure, and reduced activity levels. Therefore, it is recommended that during the hospitalization ADHF patients receive prophylaxis against venous thromboembolism with low-dose unfractionated heparin or low-molecular-weight heparin if there is no contraindication [5]. Individual therapeutic choices for ADHF are reviewed in detail below. • What treatments are used to relieve congestion? Several days to weeks prior to the appearance of signs and symptoms of volume overload, patients may develop hemodynamic congestion, defined as an elevation of ventricular filling pressure/pulmonary capillary wedge pressure independent of clinical evidence of fluid overload [17]. www.jcomjournal.com Diuresis In patients admitted to the hospital with ADHF, initial effective diuresis is vital to lowering cardiac filling pres- Vol. 22, No. 4 April 2015 JCOM 183 Acute Decompensated Heart Failure Table 3. Precipitating Factors in Acute Decompensated Heart Failure Dietary noncompliance (excessive sodium and water intake) Medication noncompliance, including lack of access to medications Iatrogenic volume overload Unwarranted volume replacement Major surgery Progressive cardiac dysfunction Worsening underlying disease Alcohol abuse, cocaine Valvular heart disease (stenosis or regurgitation) Atrial fibrillation with rapid ventricular response Ventricular tachyarrhythmias Bradyarrhythmias Uncontrolled hypertension Acute coronary syndrome Myocardial dysfunction from right ventricular pacing Pulmonary disease Chronic obstructive pulmonary disease Obstructive sleep apnea Pulmonary embolism Anemia Hyper- or hypothyroidism Medication related Pioglitazone or rosiglitazone Non-steroidal anti-inflamatory drugs Tricyclic antidepressants (increase risk of ventricular arrhythmia) Theophylline B-agonist bronchodilators (induce tachyarrhythmia) Calcium channel blockers Bladder outlet obstruction Adapted from reference 5. sures and relieving symptoms of congestion. Intravenous loop diuretics represent the first line of treatment and have long been the mainstay of therapy for decompensated heart failure with preserved or reduced ejection fraction, reducing fluid overload, and relieving symptoms. Despite its long track record, the dose administration of IV diuretics is more of an art than a science. Medication dosage sufficient to produce a rate of diuresis that will optimize volume status and relieve signs and symptoms of congestion without causing kidney injury or hypotension is recommended [5]. Due to the relatively short half-life of loop diuretics and concerns about tubular sodium reabsorption in the kidneys, continuous IV diuretic infusion has been suggested to enhance diuresis and 184 JCOM April 2015 Vol. 22, No. 4 avoid sodium and fluid rebound [5,20,21]. However, continuous loop diuretic infusion has not proven superior to intermittent IV bolus dosing in clinical studies. Recent data from the Diuretic Optimization Strategies Evaluation (DOSE) trial comparing bolus versus continuous infusion diuretic strategy in patients with ADHF showed no difference in global symptom relief, diuresis, or any of the clinical secondary endpoints including composite of death, re-hospitalization, or ED visits with either IV bolus versus continuous infusion or low versus high doses of furosemide [22]. Concern has also been previously raised about adverse outcomes utilizing high doses of loop diuretics in the treatment of ADHF [20,23,24]. However, the DOSE trial also evaluated the safety of 2 strategies for furosemide dosing in patients with ADHF. The study randomized ADHF patients with a prior diagnosis of chronic heart failure to 4 different treatment groups, either a high dose (2.5x their daily chronic oral furosemide dose) or low dose (1x their daily chronic oral furosemide dose), which was given either twice daily via IV bolus or via continuous infusion. The study showed no difference in change in renal function from baseline to 72 hours with either IV bolus versus continuous infusion or low versus high doses of furosemide [22]. One protocol which seems reasonable is to first give an IV dose of a loop diuretic twice that of the home oral dose and reassess in 1 to 2 hours for response; if there is no response to the initial dose, the loop diuretic should be increased until adequate diuresis occurs or the maximum recommended dose is reached. In patients who fail to respond to large doses of loop diuretics, the addition of a non-loop diuretic (ie, thiazide or potassium-sparing diuretic) may be effective in enhancing the response to the loop diuretic. If the desired clinical response is not achieved, professional guidelines also recommend alternating either a bolus or continuous infusion therapy different from the initial strategy, or other loop diuretic may be considered (Table 4) [5]. Finally, previous studies have suggested that the addition of low-dose dopamine to diuretic therapy may enhance decongestion and preserve renal function in ADHF [25–27]. Dopamine at low infusion doses (1–3 mcg/min) directly activates dopaminergic receptors in the kidney promoting renal vasodilatation. This vasodilatory effect augments renal blood flow leading to an increase in urine output. This theoretical effect, however, has not translated into improved clinical outcomes in patients with ADHF. The recent Renal Optimization Strategies Evaluation in Acute Heart Failure www.jcomjournal.com Case-based review Table 4. Medications Used in the Management of ADHF Drug Initial Dose Maximum Single Dose Intravenous Infusion Bumetanide 1.0 mg IV 4 to 8 mg IV 1 mg IV load then 0.5–2 mg/hour Furosemide 40 mg IV 160 to 200 mg IV 40 mg IV load then 10 to 40 mg/hour Torsemide 10 mg IV 100 to 200 mg IV 20 mg IV load then 5 to 20 mg/hour Loop Diuretics* Thiazide Diuretics – Add to Loop Diuretic Metolazone 2.5 mg oral once or twice daily 5 mg oral once or twice daily Chlorthiazide 500 mg IV once or twice daily 1000 mg IV once or twice daily Chlortalidone 12.5 to 25 mg once daily 100 mg once daily Hydrochlorothiazide 25 mg oral once or twice daily 100 mg oral once or twice daily Nitroglycerin 20–30 mcg/min IV >100 mcg/min 10 to > 100 mcg/min Close monitoring with high doses Nitroprusside 10–20 mcg/min 300 mcg/min Rarely required and increases risk of toxicity 10 to 300 mcg/min May be increased by 20 mcg/min Niseritide 0.01 mcg/kg/min 0.03 mcg/kg/min 0.01 to 0.03 mcg/kg/min May be increased by 0.005 mcg/kg/min to achieve desired hemodynamic effects Intravenous Vasodilators Intravenous Inotropic Agents Dopamine 1-3 mcg/kg/min 20 mcg/kg min 1–3 mcg/kg/min activates dopaminergic receptors causing vasodilatation. 3–8 mcg/kg/min exerts positive chronotropic and inotropic effects. 5–20 mcg/kg/min results in vasoconstriction. Dobutamine 2 mcg/kg/min 20 mcg/kg/min 2 to 20 mcg/kg/min titrate to desired response by 1–2 mcg/kg/min Milrinone 0.25 mcg/kg/min 0.75 mcg/kg/min 0.25 to 0.75 mcg/kg/min IV = intravenous. *Loop diuretics equivalent dose: Oral – 1 mg bumetanide = 20 torsemide = 80 mg furosemide; IV – 1 mg bumetanide = 20 torsemide = 40 mg furosemide. (ROSE-AHF) study randomized patients with ADHF and renal dysfunction to low-dose dopamine (2 mcg/ kg/min) or placebo in addition to diuretic therapy. The study failed to demonstrate significant differences in urine output at 72 hours or improved renal function in patients randomized to dopamine compared to placebo [27]. Ultrafiltration For patients with marked fluid overload who are unresponsive to diuretic therapy, peripheral ultrafiltration may be considered. Initial data demonstrated that early www.jcomjournal.com ultrafiltration effectively and safely reduced congestion in patients with ADHF with diuretic resistance and renal insufficiency. Length of stay was reduced, with 60% of discharges in 3 days or less and 1 readmission at 30 days. Neurohormonal activation, indicated by reduction in BNP level, was reduced without worsening glomerular filtration rate, hypotension or electrolyte abnormalities [28]. The UNLOAD trial confirmed these results and extended their findings to show that patients undergoing peripheral ultrafiltration had greater weight and net fluid loss at 48 hours and reduced rate of rehospitalization at Vol. 22, No. 4 April 2015 JCOM 185 Acute Decompensated Heart Failure 90 days when compared with IV diuretic therapy alone in ADHF patients. Interestingly, there was no difference in the dyspnea score at 48 hours and there was a trend toward worsening of renal function in the ultrafiltration group. The study was not powered to document a survival benefit [29]. However, the more recent Cardiorenal Rescue Study in ADHF (CARRESS-HF) trial involving patients with ADHF and worsening renal function showed that there was no difference in weight loss between patients randomized to ultrafiltration or a strategy of stepped pharmacologic therapy. Additionally, ultrafiltration was associated with a significant increase in creatinine at 96 hours and a higher rate of adverse events related to the procedure, driven by complications from intravenous catheter insertion. There was no difference between the 2 groups in death or rehospitalization for heart failure [30]. At present, ultrafiltration may be a reasonable option if all diuretic strategies are unsuccessful in relieving congestion [5]. Vasopressin-Receptor Antagonists The vasopressin-receptor antagonists represent a relatively new class of medications that target the vasopressin receptors V1a and V2. Activation of the vasopressin V2 receptors by arginine vasopressin in heart failure causes inappropriate free water retention contributing to the symptoms of congestion and hyponatremia [31]. Currently, the only 2 vasopressin-receptor antagonists available for clinical use are conivaptan (V1a /V2 receptor antagonist) and tolvaptan (V2 receptor antagonist). The effectiveness of tolvaptan was tested in a randomized study (EVEREST) in patients hospitalized with ADHF [32,33]. At 1 year there was no difference seen in the primary endpoints of all-cause mortality, death from cardiovascular causes, or first hospitalization for heart failure [32,33]. However, hyponatremia, when present, was improved in the tolvaptan group. Conivaptan has a similar hemodynamic profile compared to tolvaptan, but without improving signs and symptoms in hospitalized patients with ADHF [34]. Currently, vasopressin antagonists are recommended in the management of ADHF by professional guidelines as only a class IIb indication in hospitalized patients with volume overload and severe hyponatremia [5]. Case Continued After 24 hours of medical therapy in the CCU, the patient is no longer clammy and cool but continues to have shortness of breath, and peripheral edema 186 JCOM April 2015 Vol. 22, No. 4 is not improving. She continues to have elevated JVP and S3. Her blood pressure is now 120/79 mm Hg and her heart rate is 110. A Swan-Ganz catheter placed this morning showed a cardiac index of 1.8 L/minute/m2 (reference range, 2.5–4.0 L/min/m2); pulmonary capillary wedge pressure is 28 mm Hg (reference range, 6–12 mm Hg) and systemic vascular resistance is 1932 dyne/second/ cm5 (reference range, 800–1200 dynes/sec/cm5). The physician decides to add nitroprusside to lower her filling pressure and systemic vascular resistance. • What is the role of vasoactive medications in treatment? Vasodilators Nitroglycerin is a venodilating medication with preload reduction properties at low doses and an arterial dilator at high doses [35]. Preload reduction improves left ventricular filling pressures and pulmonary congestion without increasing the oxygen demand in the heart in patients with ADHF. This leads to an improvement of symptoms, including dyspnea, in as early as 5 minutes [36]. For a highly symptomatic patient, nitroglycerin given sublingually can be useful in an acute situation because it is typically immediately available while preparations are made for administration of IV medications. Limitations of nitroglycerin include rapid tachyphylaxis within several hours of continuous exposure at high doses, resistance to the hemodynamic effects of nitroglycerin in up to 20% of patients, and hypotension, which may occur before significant preload reduction effect can be obtained [37]. When symptomatic hypotension becomes a problem, the highest hemodynamically tolerable dose should be given. Another agent with a potent vasodilator effect used in the treatment of heart failure is sodium nitroprusside (SNP). As opposed to nitroglycerin, this drug has an equally potent preloadand afterload-reducing effect [35]. Afterload reduction through its arteriodilator effect has the benefit of increasing cardiac output and decreasing myocardial oxygen demand with improvement of pulmonary congestion [36]. SNP is used in less than 1% of patients hospitalized with heart failure [38], probably due to the potential for causing marked hypotension, its need for invasive hemodynamic monitoring, and the rare risk for thiocyanate toxicity with high doses and/or longer inwww.jcomjournal.com Case-based review fusions, especially in patients with reduced hepatic perfusion and renal function, as in the case of low-output heart failure [35]. However, data demonstrating safety and efficacy of SNP infusion in patients with ADHF are limited [39]. A single-center, retrospective case-control study suggested that the administration of SNP in carefully selected patients with advanced low-output ADHF was safe and may be associated with favorable long-term clinical outcomes [39]. SNP can be attractive in severely congested patients with hypertension or severe mitral regurgitation complicating left ventricular failure, but prospective trials are needed to clarify the safety and efficacy in this patient population. Nesiritide is a human recombinant form of BNP that has a direct effect on the vascular endothelium by increasing the bioavailability of nitric oxide through stimulation of cyclic guanosine monophosphate. Its primary mechanism of action is to reduce left ventricular filling pressures by a systemic and pulmonary vasodilator effect. It also promotes diuresis and natriuresis [40]. The initial efficacy of nesiritide was demonstrated in the VMAC (Vasodilation in the Management of Acute Congestive Heart Failure) study, a randomized trial of IV nesiritide versus IV nitroglycerin or placebo in decompensated heart failure patients. A significant reduction in pulmonary capillary wedge pressure was demonstrated within 15 minutes in the nesiritide group and maintained at 3 hours compared to either nitroglycerin or placebo, with a similar improvement in dyspnea extending out to 24 hours [41]. The large ASCEND-HF (Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure) randomized ADHF patients to nesiritide or placebo and tested the hypothesis that nesiritide would be superior to placebo in improving acute dyspnea, allcause mortality, and heart failure readmission in patients presenting with ADHF [42]. Nesiritide-treated patients showed only a modest early improvement in self-assessed dyspnea and no difference in the composite endpoint of death or rehospitalization at 30 days in patients admitted with ADHF. Reassuringly, there was no increase in renal failure compared to placebo; however, the incidence of symptomatic hypotension was higher with nesiritide [42]. Although nesiritide remains in the armentarium of vasoactive medications for ADHF, less expensive vasodilators such as nitroglycerin or nitroprusside may be preferred by many clinicians. Overall, vasodilators represent a good treatment option for patients presenting with ADHF characterized by www.jcomjournal.com low cardiac output, high filling pressures, and elevated systemic vascular resistance. There is no clear evidence, however, to suggest that IV vasodilators improve survival in hospitalized patients with ADHF; thus, its use should be restricted to the relief of dyspnea in patients with stable blood pressure [5]. Inotropic Therapy The most commonly used positive inotropic agents in the management of patients with ADHF in the United States are dobutamine (beta-1, beta-2, and alpha adrenoreceptor agonist) and milrinone (phosphodiesterase-III inhibitor) [38]. Inotropes increase cardiac output by increasing myocardial contractility, reduce left and right ventricular filling pressures, and improve hemodynamic parameters. Despite these hemodynamic effects, inotropic agents have not demonstrated a survival benefit in patients with ADHF. A major limitation regarding these agents is that they increase the risk of cardiac arrhythmias by increasing intracellular calcium in cardiac myocytes. In fact, retrospective analyses suggest that most inotropic agents are associated with an increased risk of death [38,43]. Milrinone inhibits type III isoform of the enzyme phosphodiasterase leading to an increase in intracellular cyclic AMP to exert its positive inotropic effect on the myocardium. Milrinone also exerts systemic and pulmonary vasodilator effects in the circulation decreasing right atrial, pulmonary capillary wedge, and mean arterial pressure. In the OPTIME-CHF trial, patients with chronic heart failure admitted to the hospital with ADHF were randomized to short term infusion of milrinone vs. placebo plus standard therapy. Milrinone resulted in more hypotension, atrial fibrillation and ventricular arrhythmias without any benefit on mortality or re-hospitalization [44]. A retrospective analysis from the ADHERE registry showed that in-hospital mortality was twofold higher with the use of dobutamine or milrinone in patients with ADHF when compared to treatment with vasodilators [38]. Dobutamine is a beta-1, beta-2, and alpha adrenoreceptor agonist that works by increasing myocardial contractility leading to an increase in cardiac output as its primary cardiovascular effect. Currently, routine use of IV positive inotropic agents in the absence of imminent cardiogenic shock or low output ADHF with systemic hypoperfusion is generally not recommended due to concerns of adverse effects [5]. The Vol. 22, No. 4 April 2015 JCOM 187 Acute Decompensated Heart Failure ACCF/AHA guidelines recommend the use of positive inotropic agents to relieve symptoms, improve systemic perfusion and preserve end-organ function in patients with severe left ventricular systolic failure and low output syndrome with evidence of end-organ dysfunction (such as hypotension, altered mentation, cool extremities, low urine output and serum markers indicative of renal and/or hepatic dysfunction) with or without congestion [5]. Continuous outpatient therapy with inotropes may be a viable option in patients with stage D (end stage) heart failure who are deemed unlikely to survive hospital discharge [45]. This is also supported by the ACCF/ AHA practice guidelines where IV inotropic support may be considered for the previous reasons only after all alternative therapies to achieve stability have failed (Class IIB indication) [5]. • Is there a role for morphine? For decades morphine has been considered an essential component in the armamentarium for the treatment of ADHF. Its preload-reducing effect, anti-anxiety properties, and breathlessness suppression has made morphine a popular medication in the treatment of ADHF. Despite its common use, there is a lack of prospective randomized trials demonstrating the safety and benefit of this drug. In a retrospective analysis from the ADHERE database, IV morphine used for ADHF was associated with higher rates of adverse events, including increase use of mechanical ventilation, prolonged hospitalization, increased intensive care unit admissions, and higher mortality, bringing into question its safety profile [46]. Until a randomized trial is completed demonstrating safety and benefit, caution is advised regarding the use of morphine in ADHF. Case Continued Over the next 72 hours the patient’s symptoms improved. She no longer has dyspnea at rest, she has had a proper urine-output response to therapy, her serum creatinine has returned to normal, and her vital signs have remained stable. The IV vasodilator was discontinued, dobutamine was weaned off, and the patient was transitioned to guideline-directed medical therapy with an angiotensin-converting enzyme (ACE) inhibitor 188 JCOM April 2015 Vol. 22, No. 4 while continuing IV furosemide. Hospitalized patients who are hemodynamically stable should be transitioned to guideline-directed medical therapy with an oral ACE inhibitor unless the patient has a contraindication, such as marked azotemia or hyperkalemia. Low-dose carvedilol was initiated after optimization of volume status was confirmed. In the absence of shock and after optimization of volume status, every effort should be made to initiate low-dose beta blockers prior to hospital discharge. • When is mechanical circulatory support indicated in ADHF patients? Mechanical circulatory support has emerged as a reasonable option in selected patients with acute and reversible cardiogenic shock (ie, acute coronary syndrome or an acute mechanical problem such as a torn papillary muscle or ventricular septal defect) [5]. Recently, the utility of intraaortic balloon pump (IABP) in the setting of cardiogenic shock resulting from acute coronary syndrome was called into question with the negative results from the Intraaortic Balloon Pump in Cardiogenic Shock II (IABP-SHOCK II) trial [47]. The study compared IABP with best available medical therapy alone among patients with acute myocardial infarction complicated by cardiogenic shock for who early revascularization was planned. Use of IABP did not reduce 30-day mortality compared with medical therapy in this patient population [47]. Whether IABP has a significant role in mechanical complications, such as acute ventricular septal rupture or papillary muscle rupture, is unknown due to the paucity of data in the management of patients with such complications. Therefore, when patients present with severe acute cardiogenic shock refractory to medical therapy, mechanical circulatory support with either ventricular assist devices (VAD) or extracorporeal membrane oxygenation (ECMO) is the preferred means to reverse terminal circulatory collapse. VADs are effective in the short-term as a “bridge-to-recovery” or as a “bridge-to-decision” when recovery, transplant candidacy, or neurologic status are still uncertain [48,49]. There are several options currently available for mechanical circulatory support, including surgically implanted VADs or the percutaneously implanted VADs, such as the Impella 2.5, 3.5 and 5.0 (Abiomed, Danvers, MA) and the TandemHeart www.jcomjournal.com Case-based review pump (Cardiac Assist, Pittsburgh, PA). The ideal device and optimal duration of temporary support are yet to be defined. A detailed description of the function and clinical effects of mechanical support devices is beyond the scope of this article, although thorough reviews are available [48,49]. • What elements of care may help optimize the discharge process? Transition of care in hospitalized patients with ADHF to outpatient care is a critical and vulnerable period for patients given the complexity of the discharge planning for heart failure. A multidisciplinary heart failure disease management program is recommended in both the inpatient and outpatient setting to address the barriers to successful transition of care [5]. Physicians and physician extenders, nurses, pharmacists, and social workers can work together to identify risk factors for readmission and bridge the gap between the inpatient and outpatient setting. Patients at high risk for hospital readmission should be referred to a heart failure disease management program [5,37]. Patients at high risk for hospital readmission include patients with renal insufficiency, low output state, diabetes mellitus, chronic lung disease, persistent NYHA functional class III, IV symptoms, frequent hospitalizations, multiple comorbidities, history of depression, cognitive impairment, or recurrent problems with noncompliance. There is strong evidence that a heart failure disease management program will reduce rehospitalization rates and costs while improving functional status and quality of life of the patient [37]. In addition, a heart failure disease management clinic often can see the patient shortly after discharge, which may allow earlier discharge of the patient and shorter length of stay. Proven therapies such as ACE inhibitors, angiotensin-receptor blockers, beta blockers, and aldosterone antagonists can be titrated frequently in this setting. It is strongly recommended that comprehensive written discharge instructions be provided at the end of hospitalization with special emphasis on diet, discharge medications, activity level, follow-up appointment, daily weight monitoring, and instructions for recurrence of symptoms [5]. www.jcomjournal.com Case Conclusion The patient tolerated well the initiation of guideline-directed medical therapy and is continued on the ACE inhibitor and beta-blocker medications. After 4 days IV furosemide is discontinued and transitioned to oral furosemide. Precipitant causes of heart failure were addressed throughout hospitalization. It was determined that the patient had been taking high doses of nonsteroidal anti-inflammatory drugs due to knee pain. She was educated on this and other potential precipitant factors. Heart failure education was reinforced, including self-care, emergency plans, and need for medication and diet adherence. She is scheduled an early follow-up visit within 2 weeks of hospital discharge in the multidisciplinary heart failure disease management clinic. Summary ADHF is a major public health problem commonly encountered and often initially managed in the ED. Initial history and physical examination are important to estimate the degree of congestion and peripheral perfusion. The patient’s hemodynamic status along with the use prognostic models for short-term mortality may facilitate patient triage and encourage the use of evidence-based therapy, especially in high-risk patients. Initial treatment should target the relief of congestive symptoms and intravenous loop diuretics are the mainstay of therapy. The preferred IV vasoactive medication has yet to be determined in a large prospective randomized trial. Positive inotropic agents should be reserved for patients with signs of low cardiac output and tissue hypoperfusion, however, the risk/benefit equation should be evaluated judiciously with each treatment option before initiating therapy. For patients with refractory hemodynamic collapse, ventricular assist devices can allow stabilization until recovery or decision regarding transplantation versus destination therapy. Patients with ADHF are at increased risk for readmission to the hospital as well as increased risk for death. Risk factors need to be identified and referral to a heart disease management program should be considered for those patients deemed at increased risk for rehospitalization. Corresponding author: Carlos E. Sanchez, MD, 3705 Olentanfy River Rd., Columbus, OH 43214, [email protected]. Financial disclosures: None. Vol. 22, No. 4 April 2015 JCOM 189 Acute Decompensated Heart Failure Author contributions: conception and design, CES; analysis and interpretation of data, CES; drafting of article, CES; critical revision of the article, CES, DRR; collection and assembly of data, CES. References 1. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics–2013 update: a report from the American Heart Association. Circulation 2013;127: e6–245. 2. Fonarow GC. ADHERE Scientific Advisory Committee. The ADHF National Registry (ADHERE): opportunities to improve care of patients hospitalized with ADHF. Rev Cardiovasc Med 2003;4(suppl 7):S21-S30. 3. Philbin EF, Dec GW, Enkins PL, et al. Socioeconomic status as an independent risk factor for hospital readmission for heart failure. Am J Cardiol 2001;87:1367–71. 4. Weintraub NL, Collins SP, Pang PS, et al.; on behalf of the American Heart Association Council on Clinical Cardiology and Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Acute heart failure syndromes: emergency department presentation, treatment, and disposition: current approaches and future aims: a scientific statement from the American Heart Association. Circulation 2010;122:1975–96. 5. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e147-239. 6. Nohria A, Tsang SW, Fang JC, et al. Clinical assessment identifies hemodynamic profiles that predict outcomes in patients admitted with heart failure. J Am Coll Cardiol 2003;41: 1797–1804. 7. Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med 2002;347:161–7. 8. Fonarow GC, Peacock WF, Phillips CO, et al. ADHERE Scientific Advisory Committee and Investigators. Admission B-type natriuretic peptide levels and in-hospital mortality in ADHF. J Am Coll Cardiol 2007;49:1943–50. 9. Logeart D, Thabut G, Jourdian P, et al. Pre-discharge B-type natriuretic peptide assay for identifying patients at high risk of re-admission after decompensated heart failure. J Am Coll Cardiol 2004;43:635–41. 10. Peacock WFIV, De Marco T, Fonarow GC, et al. Cardiac troponin and outcome in acute heart failure. N Engl J Med 2008;358:2117–26. 11. Ilva T, Lassus J, Siirila-Waris K, et al. Clinical significance of cardiac troponins I and T in acute heart failure. Eur J Heart Fail 2008;10:772–9. 12. Peterson PN, Rumsfeld JS, Liang L, et al. A validated risk score for inhospital mortality in patients with heart failure from the American Heart Association Get With The Guidelines program. Circ Cardiovasc Qual Outcomes 2010;3:25–32. 13. Fonarow GC, Adams KF, Abraham WT, et al, for the ADHERE Scientific Advisory Committee, Study Groups and Investigators. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classification and regres- 190 JCOM April 2015 Vol. 22, No. 4 sion tree analysis. JAMA 2005;293:572–80. 14. Felker GM, Leimberger JD, Califf RM, et al. Risk stratification after hospitalization for decompensated heart failure. J Card Fail 2004;10:460–6. 15. Lee DS, Austin PC, Rouleau JL, et al. Predicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical model. JAMA 2003;290:2581–7. 16. Abraham WT, Fonarow GC, Albert NM, et al. Predictors of in-hospital mortality in patients hospitalized for heart failure. J Am Coll Cardiol 2008; 52:347–56. 17. Gheorghiade M, Shin DD, Thomas TO, et al. Congestion is an important diagnostic and therapeutic target in heart failure. Rev Cardiovasc Med 2006;7(suppl l):S12-S24. 18. Peacock WF, Emerman C, Costanzo MR, et al. Early vasoactive drugs improve heart failure outcomes. Congest Heart Fail 2009;15:256–64. 19. Maisel AS, Peacock WF, McMullin N, et al. Timing of immunoreactive B-type natriuretic peptide levels and treatment delay in acute decompensated heart failure: an ADHERE analysis. J Am Coll Cardiol 2008;52:534–40. 20. Salvador DRK, Rey NR, Ramos GC, et al. Continuous infusion versus bolus injection of loop diuretics in congestive heart failure. Cochrane Database Syst Rev 2005(3):CD003178. 21. Pivac N, Rumboldt Z, Sardelic S, et al. Diuretic effects of furosemide infusion versus bolus injection in congestive heart failure. Int J Clin Pharmacol Res 1998;18:121–8. 22. Felker GM, Lee KL, Bull DA, et al. Diuretic strategies in patients with ADHF. N Engl J Med 2011;364:797–805. 23. Cotter G, Metzkor E, Kaluski E, et al. Randomized trial of high-dose isosorbide dinitrate plus low-dose furosemide versus high-dose furosemide plus low-dose isosorbide dinitrate in severe pulmonary edema. Lancet 1998;351:389–93. 24. Butler J, Forman DE, Abraham WT, et al. Relationship between heart failure treatment and development of worsening renal function among hospitalized patients. Am Heart J 2004;147:331–8. 25. Giamouzis G, Butler J, Starling RC, et al. Impact of dopamine infusion on renal function in hospitalized heart failure patients: results of the Dopamine in ADHF (DAD-HF) Trial. J Card Fail 2010;16:922–30. 26. Cotter G, Weissgarten J, Metzkor E, et al. Increased toxicity of high-dose furosemide versus low-dose dopamine in the treatment of refractory congestive heart failure. Clin Pharmacol Ther 1997;62:187–93. 27. Chen HH, Anstrom KJ, Givertz MM, et al. Low-dose dopamine or low-dose nesiritide in acute heart failure with renal dysfunction: the ROSE acute heart failure randomized trial. JAMA 2013;310:2533–43. 28. Costanzo MR, Saltzberg M, O’Sullivan J, et al. Early ultrafiltration in patients with decompensated heart failure and diuretic resistance. J Am Coll Cardiol 2005;46:2047–51. 29. Costanzo MR, Guglin ME, Saltzberg MT, et al; UNLOAD Trial Investigators. Ultrafiltration versus intravenous diuretics for patients hospitalized for ADHF. J Am Coll Cardiol 2007;49:675–83. 30. Bart BA, Goldsmith SR, Lee KL, et al. Ultrafiltration in decompensated heart failure with cardiorenal syndrome. N Engl www.jcomjournal.com Case-based review J Med 2012;367:2296-304. 31. Shrier RW, Abraham WT. Hormones and hemodynamics in heart failure. N Engl J Med 1999;341:577–85. 32. Konstam MA, Gheorghiade M, Burnett Jr JC, et al. Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators. Effects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial. JAMA 2007;297:1319–31. 33. Gheorghiade M, Konstam MA, Burnett Jr JC, et al. Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators. Short-term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials. JAMA 2007;297:1332–43. 34. Goldsmith SR, Elkayam U, Haught WH, et al. Efficacy and safety of the vasopressin V1A/V2-receptor antagonist conivaptan in ADHF: a dose-ranging pilot study. J Card Fail 2008;14:641–-7. 35. Shin DD, Brandimarte F, DeLuca L, et al. Review of current and investigational pharmacologic agents for acute heart failure syndromes. Am J Cardiol 2007;99:4A–23A. 36. Mattu A, Martinez JP, Kelly BS. Modern management of cardiogenic pulmonary edema. Emerg Med Clin North Am 2005;23:1105–25. 37. Lindenfeld J, Albert NM, Boehmer JP, et al. Executive Summary: HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail 2010;16:e475-e539 38. Abraham WT, Adams KF, Fonarow GC, et al. ADHERE Scientific Advisory Committee and Investigators; ADHERE Study Group. In-hospital mortality in patients with ADHF requiring intravenous vasoactive medications: an analysis from the ADHF national registry (ADHERE). J Am Coll Cardiol 2005;46:57–64. 39. Mullens W, Abrahams Z, Francis GS, et al. Sodium nitroprusside for advanced low-output heart failure. J Am Coll Cardiol 2008;52:200–7. 40. Bhalla V, Willis S, Maisel AS. B-type natriuretic peptide: the level and the drug-partners in the diagnosis and management of congestive heart failure. Congest Heart Fail 2004;10(1 suppl 1):3–27. 41. Publication Committee for the VMAC investigators (Vasodilatation in the Management of Acute CHF). Intravenous nesiritide vs nitroglycerin for treatment of decompensated congestive heart failure: a randomized controlled trial. JAMA 2002;287:1531–40. 42. O’Connor CM, Starling RC, Hernandez AF, et al. Effect of nesiritide in patients with ADHF. N Engl J Med 2011;365:32–43. 43. Elkayam U, Tasissa G, Binanay C, et al. Use and impact of inotropes and vasodilator therapy in hospitalized patients with severe heart failure. Am Heart J 2007;153:98–104. 44. Cuffe MS, Califf RM, Adams KF Jr, et al. Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) Investigators. Short-term intravenous milrinone for acute exacerbation of chronic heart failure: a randomized control trial. JAMA 2002;287:1541–7. 45. Hershberger RE, Nauman D, Walker TL, et al. Care processes and clinical outcomes of continuous outpatient support with inotropes (COSI) in patients with refractory endstage heart failure. J Card Fail 2003;9:180–7. 46. Peacock WF, Hollander JE, Diercks DB, et al. Morphine and outcomes in ADHF: an ADHERE analysis. Emerg Med J 2008;25:205–9. 47. Thiele H, Zeymer U, Neumann FJ, et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med 2012;367:1287–96. 48. Abu-Omar Y, Tsui S. Mechanical circulatory support for AMI and cardiogenic shock. J Card Surg 2010;25:434–41. 49. Ziemba EA, John R. Mechanical circulatory support for bridge to decision: which device and when to decide. J Card Surg 2010;25:425–33. 50. Sanchez CE, Richards DR. Contemporary in-hospital management strategies for ADHF. Cardiol Rev 2011;19:122–9. Copyright 2015 by Turner White Communications Inc., Wayne, PA. All rights reserved. www.jcomjournal.com Vol. 22, No. 4 April 2015 JCOM 191