Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
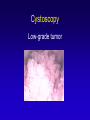
Bladder Cancer Basics, Detection, and Diagnosis Anne K. Schuckman, MD Assistant Professor USC Institute of Urology Epidemiology • • • • • • Incidence about 60,000 new cases/yr Male : female ratio - 3:1 Caucasians > African Americans and Latinos Incidence increased 33% since 1985 Age at Diagnosis: 5th-7th decade Highest Recurrence Rate of any Cancer Bladder Cancer Incidence Etiology • • • • • Smoking Industrial exposures Other environmental factors ? Radiation therapy Chemotherapy (cyclophosphamide) Smoking and Bladder CA MODIFIABLE RISK! Cost of Bladder Cancer in US Est. $3.4B annually in the U.S. 5th highest overall costs Highest per patient treatment cost ($120k200k) Long survival for non-muscle invasive cancer Intense surveillance—time lost from work, burden on quality of life Limited public awareness Symptoms & Signs • Blood in Urine (Hematuria) (80%) Must rule out bladder cancer In patients > 40 yrs old ! • • Dysuria, frequency (10-15%) Asymptomatic microhematuria (rare) (O.5-15%) Evaluation of Hematuria • Upper tract study: Intravenous pyelogram (IVP) – Historic? CT scan – sensitive with delayed phases Ultrasound-not adequate • Cystoscopy: No other Evaluation of Hematuria • Lack of Referral to Urologist • 74% for Gross, 36% for Microscopic • Gross: 13-35% have bladder cancer Flexible Cystoscopy Cystoscopy Low-grade tumor Cystoscopy High-grade, invasive tumor Transurethral Resection Bladder cancer Predictors of Behavior • Stage – depth of invasion • Grade – microscopic appearance • Genetic abnormalities (p53 mutation, etc) Staging Systems TNM System: Ta T1 T2a T2b T3 Bladder Cancer Natural History 80% superficial, low-grade Most recur (75%) Few die of bladder cancer (15%) 20% invasive and/or high grade Higher rate of progression to metastasis & death CIS - the precursor of invasive disease Non-Muscle Invasive Disease • Surveillance with Cystoscopy • 20% risk of Progression to invasive disease Goal of to identify and treat high risk lesions, prevent progression to invasive disease! Urinary Cytology - Very accurate for high-grade or CIS - Poor sensitivity for low-grade disease Sensitivity and Specificity of urinary markers Konety B, BJU Int 102:1234, 2008 Marker Sensitivity Specificity Hematuria dipstick 68 (40–93) 68 (62–98) Urine cytology 48 (16–89) 96 (81–100) BTAstat 68 (51–100) 75 (54–93) BTA TRAK 66 (51–78) 71 (50–98) NMP22 67 (21–100) 79 (43–95) ImmunoCyt 77 (18–100) 76 (62–86) UroVysion 79 (44–96) 88 (46–100) NMP 22 • FDA approved for Bladder Cancer screening in 2000 • Trial of 2000 patients • Measures level of Nuclear Matrix Protein 22 • Increased expression from cancerous bladder cells NMP 22 • Sensitivity: depends on grade of disease • Low 50-70% • Med 50-75% • High 72-100% • Overall Sensitivity 75% • Overall Specificity 86% BTA Stat • In Office assay (5 min) • Detects hCFHrp (human complement factor H related protein) • Sensitivity: 56% 62% 90% • Specificity: 72% • False + from BCG/infection FISH (UroVision) • Detect chromosomal abnormalities in 3, 7, 17. • Multiple copies of genes Urinary markers improve accuracy of cystoscopy Prior knowledge of a positive urine test resulted in urologist detecting more recurrent cancer on cystoscopy Arm Tumor seen on cysto No knowledge of test 5% Knowledge of positive test 32 % Adjuncts to Cystoscopy Florescent Cystoscopy Mynderse et al. AUA Annual Meeting, 2009 •766 randomized patients using Hexvix •45% increase in CIS detection •Decreased recurrence at 9 months 46% to 36% Confocal Laser Endomicroscopy Sonn et al, J Urol 182:1299, 2009 •Exciting new technology for in situ microscopy •May aid in grading tumors, assessing TURBT Optical Coherence Tomography Manyak et al. J Endourology 19:570, 2005 •Provides 2-D images to 2-3mm, identifies invasion Fluorescent Cystoscopy • Protoporphyrin IX (PpIX) induced by installation of Hexyl-ester of acid 5aminolevulinic acid (HAL) • PpIX Selectively “build up” in precancerous lesions (20:1) • Fluorescence induced with violet light • Increase Sensitivity and Specificity of Cystoscopy Flat multicentric CIS Fluorescent Cystoscopy Witjes JA and Douglass J (2007) The role of hexaminolevulinate fluorescence cystoscopy in bladder cancer Nat Clin Pract Urol 4: 542–549 Fluorescent Cystoscopy: Causes for “False Positive” • Inflammation/dysplasia • Prior Immunotherapy (BCG) • 58% of false-positive PpIX-fluorescing specimens displayed genetic changes similar to those in papillary carcinomas found in the same patients Fluorescent Cystoscopy: Impact on Recurrence Witjes JA and Douglass J (2007) The role of hexaminolevulinate fluorescence cystoscopy in bladder cancer Nat Clin Pract Urol 4: 542–549 Fluorescent Cystoscopy: Impact on Cost of Care • 301 pts with 7-year follow-up: • All Patients with Ta disease White Light Fluorescent Recurrence 42% 18% TUR’s 0.8/pt 2.0/pt # 1/pt Recurrence 0.3/pt Cost 420/pt 1750/pt Burger M et al. (2007) Photodynamic diagnostics and non-invasive bladder cancer: is it cost-effective in long-term application? Eur Urol 52: 142–147 Optical Coherence Tomography • Use with fluorescent cystoscopy • Allows three dimensional imaging of bladder using near-infrared light • May help limit unnecessary biopsy Schmidbauer, Remzi et al, EUROPEAN UROLOGY, 56 (2009) 914–919. Indications for Cystectomy • Muscle invasion • High-grade T1 • CIS not responsive to intravesical BCG • High grade Ta refractory to BCG • Endoscopically uncontrollable tumor Quality of Life Tools • Fact-G (physical, social, emotional, functional) • Fact-BL (Bladder Cancer) • Fact-VCI (Vand. Cystectomy Index) • EORTC QLQ-BLM30 • EORTC QLQ-BLS24 • Bladder Cancer Index (BCI) Quality of Life Tools • Not designed specifically for Bladder cancer patients • Do not address continence and body image domains adequately to ―find‖ differences in treatment groups • Do not assess patients not undergoing cystectomy (ie: bladder sparing protocols) • Retrospective • Cannot separate patient selection ―biases‖ inherent in choosing diversion type Bladder Cancer Index • Developed by University of Michigan • Measures Urinary, Sexual, and Bowel with Functional and Bother Domains • Includes RC and Endoscopic Management • Originally, 315 patients with prospective HRQOL data used to assess instrument Gilbert S, Wood D, Dunn R; ACS, March 2007 Bladder Cancer Index • Initial Findings: Sensitive to differences in patient populations • Low urinary function scores observed in ON patients due to incontinence when present • Neobladder patients had higher urinary “bother” than any native bladder patients, but not than IC patientsGilbert S, Wood D, Dunn R; ACS, March 200 Gilbert S, Wood D, Dunn R; ACS, March 2007 Conclusions • New Developments hold Promise for diagnosis • Quality of Life Tools can help “Quantify” what is working for patients • Never be afraid to ask for a Second Opinion!