Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
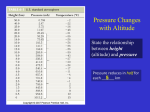
Anesthesia and Altitude Physics and Physiology of Altitude Definitions ○ High Altitude=1500 to 3500m Onset of physiologic effects of diminished Fio2. minor impairment of Sao2 (typically 9095%). Increased minute ventilation and decreased PaCo2 at rest ○ Very High Altitude= 3500 to 5500m SaO2 falls below 90% and PaO2 falls below 60mm Hg Extreme hypoxia may occur during sleep exercise or high altitude illness ○ Extreme Altitude= over 5500em Significant hypoxia and hypocapnia exist. Deterioration of physiologic function will occur. Permanent habitation can not exist Anesthesia and Altitude Physics and Physiology of Altitude Previous Medical Research ○ ○ ○ ○ ○ ○ ○ ○ Serious research started in the late 1940’s and early 1950’s as Mount Everest became the worlds foremost goal in Mountaineering. The English and other Europeans pioneered the research in a quest to summit Mount Everest. Initiated studies of Oxygen flow requirements for >8000m Mt Logan 1967-1969 Charles Houston MD AMS and HAPE Work of Carlos Monge ( South America) was pivotal in the field of chronic altitude physiology. Silver Hut research Sir Edmund Hilliary James West MD and Griffith Pugh 7440m Makalu 1982 AMREE Frank Sarnquist MD et al. First to measure alveolar gases and barometric pressure on Mt. Everest Summit 1982-1990 Denali Medical research project Peter Hacket MD Operation Everests I and II 1985 Himalayan Rescue Association Pheriche Khumbu Nepal Anesthesia and Altitude Environment at High Altitude Barometric Pressure falls with increasing altitude in logarithmic fashion. Therefore partial pressure of oxygen also falls (21% of Barometric pressure (BP). Causes Hypoxia. The primary problem. Example: Barometric Pressure is 50% at 5500m Related to position relative to equator Extreme cold fronts also cause a drop in BP. Anesthesia and Altitude Physics and Physiology Ventilation changes ○ Hypoxic Ventilatory response (HVR) is key ○ Hypoxia is profound enough to trigger ventilation not hypercarbia!! ○ Therefore, hyperventilation (relative to normal Carbon Dioxide levels) ○ ○ ○ ○ occurs. This drops the CO2 levels profoundly. Carotid body senses the decrease PaO2, triggers respiratory center in Medulla to increase ventilation. HVR is genetically determined. Not significantly improved by exercise. HVR decreased by ethanol, benzodiazepines, narcotics. HVR improved by Acetazolamide (Diamox) caffeine and cocaine Causes a primary respiratory alkalosis reachs maximal effect at 7 days. Plasma HCO3- drops!! Anesthesia and Altitude Physics and Physiology Chronic Altitude Polycythemia ○ Rise in Hemoglobin levels in response to chronic hypoxia ○ First described by Carlos Monge ○ Leads to a higher viscosity of blood ○ Higher level of DVT’s?? Anesthesia and Altitude Physics and Physiology Circulation Changes ○ Systemic Circulation: mild increase in Blood Pressure. Moderate increase in heart rate Moderate increase in cardiac output Heart rate returns to normal with acclimatization ○ Pulmonary Circulation Hypoxic pulmonary vasoconstriction causes increase PA pressures Not a complete return to normal with supplemental O2. ○ Cerebral circulation Balance of Hypoxic vasodilation and hypocapnic vasoconstriction Anesthesia and Altitude Physics and Physiology Hemopoietic changes ○ Research first done in 1890 in the Andes showed a increase level of hemoglobin. ○ Hypoxia causes erythropoietin secretiion. This causes bone marrow production of red blood cells. ○ RBC released as early as 5 days and occurs for several weeks. ○ Early rise in HgB level is due to decreased plasma levels The practice of Medicine at High and Extremely high Altitude Illnesses Aggravated by High Altitude ○ Chronic Lung Disease ○ Arteriosclerotic Heart Disease ○ Hypertension ○ Sickle Cell Disease ○ Pregnancy The practice of Medicine and Anesthesia at High and Extremely high Altitude Illnesses aggravated by high altitude Chronic Lung Disease: ○ COPD: Reduced exercise capability. Hypoxemia, pulmonary hypertension can be expected to worsen. If SaO2 is <85% at sea level, reccommend supplemental oxygen. 1920m shown to be well tolerated. ○ Pulmonary Hypertension: Increased incidence of HAPE. Travel to high altitude is contraindicated. ○ Obstructive sleep apnea: May become severely hypoxic at altitude. Periodic breathing cheyenne stokes respiration is worsened. ○ Asthma: Can be aggravated by airway heat loss of altitude, however, problems are quite unusual. Not a contraindication to travel to altitude but recommend bringing all medications The practice of Medicine at High and Extremely high Altitude Arteriosclerotic Heart Disease Healthy heart has been shown to tolerate extremely high altitude without problems. Shown by electrocardiogram, echocardiograms, heart catheterizations and exercise stress tests. Little clear evidence as yet for increased cardiac ischemic events in patients with history of ischemic cardiovascular disease. Moderate altitude is tolerated, with reduced levels of exercise. High and very high altitude is not reccomended. Patients with CABG who are asymptomatic and have normal stress tests have successfully completed climbs over 5200m The practice of Medicine at High and Extremely high Altitude Hypertension A small and transient rise in blood pressure is seen on travel to high altitude. A similar rise occurs in patients with preexisting hypertension Reccomendations to continue with current medications make sense. What about diuretics?? The practice of Medicine at High and Extremely high Altitude Sickle cell anemia Sickle cell crisis is well known complication of exposure to high altitude 20% incidence of crisis in patients with hemoglobin SC with travel to 1500-2000m Splenic infarction syndrome more common, The practice of Medicine at High and Extremely high Altitude Pregnancy Limited data exist Higher incidence of pregnancy induced hypertension and pre- eclampsia No documented increase in spontaneous abortion, placenta abruption, placenta previa, No fetal heart rate changes appear evident at moderate altitude. Airplane travel is okay but >4000m is not reccomeded The practice of Medicine at High and Extremely high Altitude The practice of Medicine at High and Extremely high Altitude Advisability of Exposure to High and Very High Altitude for common conditions Anesthesia and Altitude The practice of Anesthesia at Altitude Pre-existing medical conditions and anesthesia Reduced Partial pressure of Oxygen at altitude and hypoxia with anesthesia N2O at Altitude The practice of Anesthesia at Altitude Pre-existing medical conditions and anesthesia CAD Congestive Heart Failure HTN Serious Arrhythmias Cerebro-Vascular disease Sickle Cell Anemia Pulmonary Conditions Pulmonary Hypertension OSA Pregnancy The practice of Anesthesia at Altitude Reduced Barometric pressure causes a reduced partial pressure of oxygen. Causes an underlying hypoxic precursor. Once patient is intubated and ventilated in a semi-closed circuit the percentages of inhaled gases can be tightly controlled but the reduced barometric pressure remains the same. If patient is undergoing Intravenous sedation or regional anesthetic, then they are subjected to lower partial oxygen tension. Typically this does not cause a significant problem in healthy individuals. Can lead to issues in patients with underlying diseases as previously discussed. Inspired oxygen content is titrated to effect The practice of Anesthesia at Altitude Using Nitrous Oxide at altitude. Remember that the relative ratios of all gases remain the same. The total number of molecules in a given space is diminshed with reduced pressure. Typically our concern is simply with reduced barometric pressure causing an insuffcient oxygen delivery to meet the metabolic needs of the tissue. We recommend not delivering more than 50% Nitrous oxide over 2500m Anesthesia and Altitude Case Report #1 43 year old male for urgent laparoscopic cholecystectomy Obstructive sleep apnea Morbid obesity Lives at sea level Smokes ½ pack per day Has a room air SpO2 = 83%, RR=26 He complains of pain despite being apparently over sedated by emergency room Anesthesia and Altitude Case Report #2 75 year old female smoker, COPD, Known coronary artery disease. History of Congestive heart failure in past Lives at sea level. Has fallen, fractured her hip and now needs open reduction internal fixation of fracture