Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
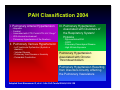
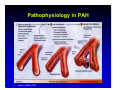
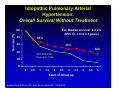
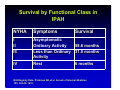
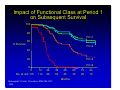
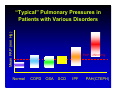
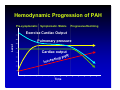
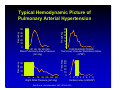
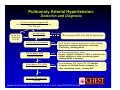
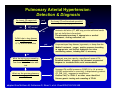
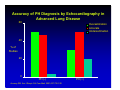
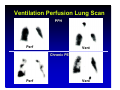
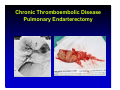
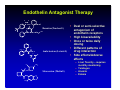
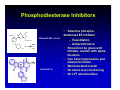
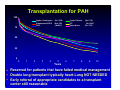
Pulmonary Arterial Hypertension: The OTHER Hypertension: What do you need to know? O O S O NH O N N OH N O N Robert Schilz DO, PhD Medical Director of Lung Transplant and Pulmonary Vascular Disease Case Western Reserve University Cleveland, OH Potential Conflicts of Interest • • • • • • • • • Actelion Ltd. Encysive Glaxo-Wellcome Myogen (Gilead) Pfizer ICOS INO Therapeutics United Therapeutics Aztra-Zeneca Really Useful Things to Remember About PAH • Classification Dictates Treatment – Pulmonary hypertension is an observation not a diagnosis • Diagnosis is Critical and Difficult – – – – Echocardiography is best for screening but lacks specificity Alternate and unusual diagnoses are the rule. V/Q scan is important to exclude chronic thromboembolism Right (possibly with Left) heart catheterization is the standard of care for diagnosis. • Therapy – Calcium channel blockers are the best drugs nobody will ever use – Current therapy consists of risk stratified use of prostacyclins, endothelin receptor antagonists and phosphodiesterase inhibitors • Future Therapies and Concepts are Rapidly Evolving What is an abnormal pulmonary pressure? Mean PAP greater than: 25 mm Hg at rest 30 mm Hg during exercise, Pulmonary Arterial Pressure (mm Hg) Systolic 18 - 25 Diastolic 6 - 10 Mean 12 - 16 PCWP 6 - 10 PVR (dynes-sec-cm-5) 60-120 PAH Classification 2004 I. Pulmonary Arterial Hypertension - Idiopathic - Familial - Associated with CTD, Portal HTN, HIV, Drugs* - With Venous Involvement - Pulmonary Hypertension of the Newborn II. Pulmonary Venous Hypertension - Left Ventricular Dysfunction (Systolic or diastolic) - Valvular Disease - Pulmonary Vein Disease or Anomaly - Pericardial Constriction III. Pulmonary Hypertension Associated with Disorders of the Respiratory System/ Hypoxia - Hypoventilation/OSA - COPD - Pulmonary Parenchymal Disease - High Altitude Exposure Pulmonary Hypertension Associated with Chronic Thromboembolism Pulmonary Hypertension Resulting from Disorders Directly Affecting the Pulmonary Vasculature Adapted from Simonneau G, et al. J Am Coll Cardiol 2004;43:5S-12S What is the estimated prevalence of pulmonary arterial hypertension in United States? • Population – – – – – – – – Idiopathic Familial Connective Tissue HIV Portal Pulmonary Anorexigen Congenital Heart Disease CTEPH (600,000 PE) 1-4:500,000 (6-26% of IPAH) 10%-20% 1:5000 5-8:1000 1:25000 100% of unrepaired 3:100 Overall prevalence independently estimated at France prevalence* 15/million 3000 cases 7500-30000 cases 200 cases 8000 cases ?3000-10000 cases 18000 cases 50-100000 cases. *American Journal of Respiratory & Critical Care Medicine. 173(9):1023-30, 2006 What distinguishes PAH from other elevations of pressures in the lungs? • • • Pathology Progressive, fatal course Magnitude of pressure elevations in symptomatic patients • Hemodynamic limitation of exercise • Treatment Pathophysiology in PAH Gaine, JAMA, 2000 Idiopathic Pulmonary Arterial Hypertension: Overall Survival Without Treatment Est. Median survival: 2.8 yrs (95% CI, 1.9 to 3.7 years) Survival (%) 100 80 68% 60 48% 34% 40 lSSc With PAH Stupi et al. 1986 20 0 0 0.5 1 1.5 2 2.5 3 Years of follow up adapted from D’Alonzo GE, et al. Ann Int Med 1991;115:343-49 3.5 4 4.5 5 Survival by Functional Class in IPAH NYHA Symptoms I II III Asymptomatic Ordinary Activity 58.6 months Less than Ordinary 31.5 months Activity Rest 6 months IV Survival NIH Registry Data: D’Alonzo GE et al. Annals of Internal Medicine 105: 343-49, 1991. Impact of Functional Class at Period 1 on Subsequent Survival 100 80 FC=1 60 % Survival FC=2 40 20 FC=3 FC=4 0 0 No. at risk: 115 12 112 24 86 McLaughlin VV et al. Circulation. 2002;106:14771482. 36 63 48 46 Months 60 30 72 20 84 10 Mean PAP (mm Hg) “Typical” Pulmonary Pressures in Patients with Various Disorders Normal PAP = 25mm Hg COPD OSA SCD IPF PAH(CTEPH) Hemodynamic Progression of PAH Pre-symptomatic Symptomatic /Stable Progressive/Declining Exercise Cardiac Output Level Pulmonary pressure Cardiac output VR P g in s a e r Inc Time Typical Hemodynamic Picture of Pulmonary Arterial Hypertension Frequency Frequency 50 40 30 20 10 0 30 20 10 0 10 20 3040 50 60 70 80 90 Pulmonary Vascular Resistance Index (U*M2) Frequency Frequency 20 40 60 80 100 120 Mean Pulmonary Artery Pressure (mm Hg) 4 8 12 16 20 24 28 Right Atrial Pressure (mm Hg) 30 25 20 15 10 5 0 50 40 30 20 10 0 1 2 3 4 5 6 7 8 Cardiac Index (L/Min/M2) Rich S et al. Ann Intern Med. 1987;107:216-223. Key Elements in Classification • All pulmonary hypertension is not the same. • Pulmonary arterial hypertension is uniquely fatal and progressive. • Pathogenesis involves endothelial dysfunction and dysregulation of growth with important genetic susceptibilities for some cases of idiopathic diseases Diagnosis When should the diagnosis of PAH be considered? • Patients with unexplained exercise limitation • Patients with clinical signs consistent with right heart dysfunction • Patients with abnormal right ventricular findings on radiography, echocardiography or electrocardiography • Patients with systemic disease known to be associated with PAH Pulmonary Arterial Hypertension: Detection and Diagnosis Is there a reason to suspect PAH Clinical history (symptoms, risk factors, family Hs.), Exam, CXR, ECG yes no No further evaluation for PAH no Is PAH likely? Echo Rationale TRV to measure RVSP; RVE; RAE; RV Dysfunction: yes Is PAH due to LH disease? Echo yes no Is PAH due to CHD? Echo with contrast yes no Is PAH due to CTD, HIV? Serologies yes Dx LV systolic, diastolic dysfunction; valvular disease: Appropriate treatment and further evaluation if necessary, including R&LHC Dx abnormal morphology; shunt: Surgery. Medical treatment of PAH or evaluation for further definition or other contributing causes, including R&LHC if necessary Dx Scleroderma, SLE, other CTD, HIV: Medical treatment of PAH and further evaluation for other contributing causes, including RHC no Is chronic PE suspected? VQ scan adapted from McGoon M, Gutterman D, Steen V, et al. Chest 2004;126:14S-34S Pulmonary Arterial Hypertension: Detection & Diagnosis Is chronic PE suspected? VQ scan no yes Is chronic PE confirmed and operable? Pulmonary angiogram yes VQ normal no Is PAH due to lung disease or hypoxemia? PFTs, arterial saturation no What limitations are caused by the PAH? Functional class; 6-minute walk test What are the precise pulmonary hemodynamics? RHC yes Anatomic definition (CT, MRI may provide additional useful but not definitive information): Thromboendarterectomy if appropriate or medical treatment; clotting evaluation; a/c Dx parenchymal lung disease, hypoxemia, or sleep disorder: Medical treatment, oxygen, positive pressure breathing as appropriate, and further evaluation for other contributing causes, including RHC if necessary Document exercise capacity regardless of cause of PH: Establish baseline, prognosis and document progression/ response to treatment with serial reassessments Document PA and RA pressures, PCWP (LV or LA pressure if PCWP unobtainable or uncertain), transpulmonary gradient CO, PVR, SvO2, response to vasodilators: Confirm PAH, or IPAH if no other cause identified Discuss genetic testing and counseling of IPAH adapted from McGoon M, Gutterman D, Steen V, et al. Chest 2004;126:14S-34S Alternative Diagnoses of Patients Referred to PAH Specialty Clinic ILD VTE Other Structural Heart Disease OSA LV Dysfunction Obstructive Lung Disease All Alternative Diagnoses N = 268, all patients referred to PAH specialty center. Moghbelli MH, et al. Am J Respir Crit Care Med. 2008;177:A923. Pulmonary Hypertension: Signs and Symptoms Symptoms Signs Dyspnea on exertion Jugular vein distention Fatigue Syncope Accentuated pulmonic valve component (P2) Anginal chest pain Right-sided third heart sound (S3) Hemoptysis Tricuspid insufficiency murmur Raynaud’s phenomenon Hepatomegaly Prominent right ventricular impulse Peripheral edema Nauser TD, Stites SW. Am Fam Physician 2001;63(9):1789-98 Findings on Electrocardiogram • RVH, RAE, RAD, RBBD Findings in PH Chest Radiography • Cardiac enlargement • Prominent proximal PA • “Pruning” of distal PA Echocardiography in PAH • • • • • • TR RVE RAE RVH Flattening of IVS Dilated IVC Accuracy of PH Diagnosis by Echocardiography in Advanced Lung Disease 60 Overestimation Accurate Underestimation 40 % of Studies 20 0 PH (-) Arcasoy SM. Am J Respir Crit Care Med. 2003;167:735-740. PH (+) 317 patients with RHC & Doppler less than 30 days apart 160 RHC PASP (mm Hg) 140 120 100 80 60 40 20 0 0 50 100 Echo RVSP (mm Hg) 150 200 Ventilation Perfusion Lung Scan PPH Perf Vent Chronic PE Perf Vent Chronic Thromboembolic Disease Pulmonary Endarterectomy Misclassification of PAH Due to Use of PCWP Rather Than LVEDP Halpern SD, et al. Am J Respir Crit Care Med. 2008;177:A259. Key Elements and Pitfalls in PH Workup • PAH in a differential diagnosis should be considered frequently but is a rare diagnosis • Echo RVSP estimates can be unreliable • Chronic thromboembolism is an important consideration among patients with PH • Be suspicious of cases which do not fit “typical” patient presentations • All patients getting treatment for PAH deserve right heart cath (and perhaps left heart cath) Targets for Therapy in PAH McLaughlin VV, McGoon MD. Circulation. 2006;114:1417-1431. General Supportive Therapy for PAH • • • • • • Oxygen Diuretics Digoxin Anticoagulation Contraception Avoid anemia General Points on Therapy of Pulmonary Hypertension • The vast majority of data reflect IPAH patients and is abstracted to PAH • Experience and data (when available) does not support the use of patients that do not have the diagnosis of PAH Why are calcium channel antagonists like Brooke Shields? • Both have gotten significant attention while offering very little to very few! Definitions for Calcium Channel Antagonist Therapy • Acute challenge with inhaled NO, intravenous epoprostenol or intravenous adenosine. • Positive Response: – >10mm mean PAP decrease and – < 40mm final mean PAP – Unchanged or increased CI • Sustained Response to CCB: – Attainment of NYHC I or II with normal or near normal hemodynamics after several months of therapy. Prostacyclin Therapy HOOC O Epoprostenol (Flolan®) O H O H COOH CH • Multiple Potential Therapeutic Actions Iloprost (Ventavis®) 3 OH OH HO2C-CH2-O Treprostinil(Remodulin®) HO HO • • • • • • Vasodilation Antiproliferative Antiplatelet Increase NO Decrease ET-1 Inonotrope Epoprostenol Delivery System • • • • • • • • Continuous IV infusion Short t1/2 & chemical instability) Adverse outcomes related to delivery system Initial dosing 4-8 ng/kg/min Ultimate dosing frequently 40-60 ng/kg/min Expensive ($25,000-125,000/year) Difficult to manage follow-up Improves: • exercise capacity • hemodynamics • survival Treprostinil SC Delivery System • A stable prostacyclin analog • Longer t 1/2 • Subcutaneous delivery • Similar SE profile compared to epoprosetenol* • Site pain Ventavis® (iloprost) Inhalation Solution: Dosage and Administration • Indicated for inhalation via the Prodose® AAD® system only • 6-9 inhalations daily during waking hours – No more than once every two hours • Dose: maximum of 2.5 or 5 mcg per treatment – 2.5 mcg initial dose – If well tolerated, increase to 5 mcg and maintain. – If 5 mcg dose not tolerated, reduced to 2.5 mcg and maintain. ET-1 ACTIVITIES ARE MEDIATED BY ETA AND ETB RECEPTORS NO blocks ET-1 production ET-1 NO ET-1 binding to ETB stimulates ÇNO/PGI2 production and clears ET-1 ET-1 ETB ETB NOS NO COX-1 L-Arg PGI2 ET-1 ETB bET-1 ET-1 ECE ET-1 NO NOS NO promotes vasodilatation ETB NO COX-1 PGI2 L-Arg ETB ETB PDE5 Endothelial Cells ETA ETA Migration Proliferation ETA ETA ETB ÇCa++ Contraction sGC GTP 5'GMP cGMP PDE5 sGC GTP 5'GMP cGMP ÈCa++ Relaxation AC ÈCa ++ cAMP ATP Relaxation Smooth Muscle Cells Studies suggest that the blockade of the ETB receptor contributes to the imbalance of the L-arginine/NO pathway. Adapted from Spieker LE et al. J Am Coll Cardiol. 2001;37:1493-1505, and Luscher TF and Barton M. Circulation. 2000;102:2434-2440. Endothelin Antagonist Therapy O O S O NH O N N N O N O H 3 C O O H O N N Cl O CH3 O S NH N O Sitaxsentan (Thelin®) O S O CH3 • Dual or semi-selective antagonism of OH endothelin receptors • High bioavailability • Once or twice daily dosing • Different patterns of drug interaction Ambrisentan (Letaris®) • Side effects/Adverse effects Bosentan(Tracleer®) O – Liver Toxicity – requires monthly monitoring – Teratogen – Anemia – Edema Phosphodiesterase Inhibitors Sildenafil (Revatio®) Tadalafil (®) • Selective phosphodiesterase E5 inhibitor – Vasodilation – Antiproliferative • Should not be given with nitrates, caution with alpha blockers • Can have hypotension and edema formation • Well tolerated overall • No blood level monitoring • No LFT abnormalities Transplantation for PAH 100 Alpha-1 Antitrypsin Emphysema/COPD PPH 75 (N=1,234) (N=4,353) (N=691) Cystic Fibrosis IPF Sarcoidosis (N=1,703) (N=1,855) (N = 276) 50 25 0 0 1 2 3 4 5 6 7 8 9 10 Years • Reserved for patients that have failed medical management • Double lung transplant typically heart-Lung NOT NEEDED • Early referral of appropriate candidates to a transplant center still reasonable Algorithm for the Management of PAH Anticoagulants + Diuretics +Oxygen + Digoxin Acute Vasoreactivity Testing Positive Oral CCB Sustained Response NYHC I or II? Negative Lower Risk No ERA’s or PDE-5 (oral) Epoprostenol or Treprostinil (IV) Iloprost (Inhaled) Treprostinil (SC) * Yes Continue Oral CCB Investigational Protocols Combination Therapies * Higher Risk Epoprostenol or Treprostinil (IV) ERA’s or PDE-5 Iloprost (Inhaled) Treprostinil (SC) * Investigational Protocols Combination Therapies * * Atrial Septostomy Lung Transplantation *Reassess at 1-3 month intervals: Are Goals of Therapy Met? Adapted from McLaughlin VV, McGoon MD Circulation2006 114:1417-1431 Prognostic Factors for Risk of PAH Disease Progression Determinant Higher Risk Lower Risk Evidence of RV failure Yes No Progression Rapid Gradual WHO class IV II, III 6-minute walk distance <325 m >380 m Brain natriuretic peptide >180 pg/mL <180 pg/mL Echo findings Pericardial effusion; significant RV dysfunction Minimal RV dysfunction Hemodynamics High RAP, low CI Normal/near normal RAP and CI Adapted from: McLaughlin VV., McGoon MD. Circulation. 2006;114:1417-1431. Current Treatment and Follow-up • Consider coumadin, digoxin, diuretics and oxygen • Goal directed therapy (Walk +/hemodynamics +/- FC) • Frequent follow-up with exercise and imaging proportional to need, risk and expected drug action • Recath with vasodilator testing at 6-12 mo, with changes in therapy and consideration cath yearly Sobering Facts About Current Therapy • Medical therapy will statistically fail in almost all patients at some time • Statistical failure is different for different therapies and only partially defined • We usually have no clear indication of which agents are best for any given patient • Optimal combination therapy is unknown • Current experience suggests that many combinations are not likely optimal Future Directions in PAH: Potential New Therapeutic Targets • Prostacyclin Analogs – Oral and inhaled treprostinil • Endothelin Antagonists • Sitaxsentan • NO Augmentation – C-GMP phosphodiesterase inhibitors (tadalafil) • Tyrosine kinase/growth factor receptor inhibitors – Imatinib, sorafenib • • • • • • • Vasoactive intestinal peptide (VIP) Serotonin transporter agonists Adrenomedullin Rho-kinase inhibitors Cicletanine Endothelial progenitor cells Gene therapy – Vectors expressing prostacyclin synthase, endothelial NOS, or vascular endothelial growth factor Really Useful Things to Remember About PAH • Classification Dictates Treatment – Pulmonary hypertension is an observation not a diagnosis • Diagnosis is Critical and Difficult – – – – Echocardiography is best for screening but lacks specificity Alternate and unusual diagnoses are the rule. V/Q scan is important to exclude chronic thromboembolism Right (possibly with Left) heart catheterization is the standard of care for diagnosis. • Therapy – Calcium channel blockers are the best drugs nobody will ever use – Current therapy consists of risk stratified use of prostacyclins, endothelin receptor antagonists and phosphodiesterase inhibitors • Future Therapies and Concepts are Rapidly Evolving QUESTIONS?