Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
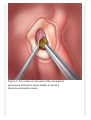
TheNeurosurgicalAtlas byAaronCohen-Gadol,M.D. UseofEndoscopesinSkullBase Surgery BasicsoftheTransnasalEndoscopicApproach Figure1:Endoscopicilluminationofthecentralskullbasecan beachievedwithastraightendoscopeplacedwithinonenostril. Endoscopespermitthevisualizationofmanyskullbase structuresincluding:sphenoidsinus,plannumsphenoidale, sella,pituitarygland,cavernoussinus,dorsumsella,suprasellar region,ethmoidroof,frontalsinus,andcribiformplate. Figure2:Efficientendoscopictechniqueinvolvesbinarial endoscopicdissection.Theendoscopeshouldbeheld superiorlywithinonenostrilbyonesurgeon.Thispermitsa secondsurgeontomanipulatetwodissectioninstruments,one withintheipsilateralandcontralateralnares. Figure3:Themiddleturbinateisremovedunderendoscopic guidance.Themiddleturbinateshouldbepreservedduringan endonasalprocedureifpossible,howeverahypertrophic turbinatewithipsilateralnasalseptaldeviationoften necessitatesremovaltopermitvisualizationandinstrument manipulation.Toperformthisremoval,theturbinateshouldbe injectedwithepinephrineandlidocainetofacilitate vasoconstrictionandbetransectedatitsrootandremoved. Figure4:Thesphenoethmoidrecesshousestheostiumofthe sphenoidsinus.Therecessisboundedmediallybythe posteriornasalseptumandlaterallybythesuperiorturbinate. Removetheposteriorthirdofthenasalseptumwithabackbitingrongeur.Asuction-debriderisusedtoremoveexcess mucosafollowingtheremovaloftheethmoidperpendicular plate.Theostiumisenlargedmedially(dashedoutline)witha kerrisonpunch.Theenlargementiscompletedwithdrillingof thesphenoidrostrumtoitsbasecentrallyandlaterally. Figure5:Awidesphenoidotomyiscreatedtopermitnecessary manipulationbytwodissectinginstrumentswithinthefield. Visualizationoftheplanumsphenoidale,tuberculumsella,sellar face,middleclivus,andthelateralwallofthesphenoidsinus adjacenttothecavernoussinus.Beginthebonyresection superficialtotheanteriorselladura,whichisrepresentedbythe lowerdashedrectangle.Thebonyexcisionisthenextended superiorlytoremovethetuberculumsellaandbonecovering theplanumsphenoidale,opticcanals,andmedialoptic-carotid recess,whichisrepresentedbytheupperdashedrectangle. Theremovalcanalsobeextendedinferiorlyandlaterally. Figure6:Completedendoscopicapproachtothepituitarygland andopticchiasm ClivalChordoma Figure1:Coronalviewofaclivalchordoma.Chordomaswithin thislocationexertmasseffectonthepituitaryglanddisplacing itrostrallyandonthebrainstemdisplacingitposteriorly.An anteriorapproachwillrequireresectionoftumoranteriorand inferiortotheglandtopermitelevationofthegland. Figure2:Axialviewofaclivalchordoma. Figure3:Sagittalviewofaclivalchordoma. Figure4:Transsphenoidalendoscopicapproachtoasphenoid sinustumor.Thewidesphenoidotomyallowsforamore optimalexposureofthetumor,thesuprasellarregion,and planumsphenoidale. Figure5:Transsphenoidalendoscopicapproachthroughthe sellaandplanumtoexposeasellartumor.Thesellarfloorand facecanberemovedwithkerrisonpunchesandadrill.Bone excisioncanbeextendedlaterallyoneachsideofthesellato theanteriorfaceofthecavernoussinus.Duralincisioncanbe madesuperiorandinferiortotheintercavernoussinus,andthe sinuscanthenbecoagulatedandremoved.Proximalpituitary glandandsuprasellarexposurecanbeachievedbywidely openingtheduraalongthesellaandsuprasellarsurface.Distal pituitaryglandexposurecanbeachievedbytransectingthe diaphragmasella. Figure6:Transsphenoidalendoscopicapproachtoa retrosellartumor(dashedline).Toachieveretrosellaraccessthe pituitaryglandmustbeelevatedoutofthesella.Tumor resectionmayrequireopeningoftheclivalordorsumsella tumor.Duralinfiltrationisobservedandcomplicatesthe resectionbutprepontinearachnoidistypicallyspared. Esthesioneuroblastoma Figure1:Coronalviewofanesthesioneuroblastoma.Erosionof thecribiformplateiscommonlyobservedleadingtoextension intotheanteriorcranialfossaorfrontalsinus. Figure2:Axialviewofanesthesioneuroblastoma. Figure3:Sagittalviewofanesthesioneuroblastoma. Figure4:Duringanendoscopicapproachthetumorcanbe viewedprojectingfromtheolfactorycleft.Themiddleturbinateis displacedlaterallytoaccommodatethetumormass. Figure5:Tumorexposureisachievedbyperformingan ethmoidectomyandmiddleturbinectomy.Thisadditional exposureiscriticaltoassistinidentifyingthetumororigin. Figure6:Piecemealresectionofthetumorisperformedandthe originisidentifiedfollowingskeletonizationofthecribiformplate andethmoidroof. Figure7:Followingidentificationoftheoriginforthe esthesioneuroblastomaalongtheduraandskullbase,generous excisionmarginsattheoriginshouldbeachievedandverified byintraoperativefrozensectionanalysis. Figure8:Theclosurerequiresaduralrepairattheintraduralsite ofthetumor.Therepairsubstanceisplacedintradurallyand extradurally.Thebonydefectresultingfromtheapproach shouldberepairedwithaseptalbonegraftorprostheticplate. Theseptalbonegraftorprostheticplateshouldbelargeenough toprovideoverlapwiththebonymargins(asseeninthe illustration).Amucosalflapisalsousedtosuperficiallyoverlay onthebonydefect.Itcanbeacquiredasapedicledflaporfree graft.Toensurecompetenceoftheclosureanadhesivecanbe usedtopreventleakageofcerebrospinalfluid. PituitaryMicroadenomaandMacroadenoma Figure1:Coronalviewofapituitarymicroadenoma.The adenomaismostcommonlypresentwithintheinferiorextentof thecentralportionofthepituitarygland.Theadenomaby definitionislessthan1cmindiameter,mostcommonly measuresapproximately5mmindiameter.Despitethesmallsize oftheadenoma,itisnecessarytowidelyremovethesphenoid bonetoallowforinstrumentmanipulationandefficient resection. Figure2:Axialviewofapituitarymicroadenoma. Figure3:Sagittalviewofapituitarymicroadenoma. Figure4:Followingthestandardendoscoptictransphenoidal approach,thesellarfloorshouldberemovedtopermita durotomyinarectangularpattern(dashedline).Bipolarforceps canbeusedtocoagulatethecornersoftherectangular durotomytopreventopeningbetweenthetwolayersand formationofatracttothecavernoussinus.Thedurotomycan beextendedbycuttingoutfromthecornersoftheinitial rectanglardurotomy(dashedline). Figure5:Followingtheextensionofthedurotomy,theanterior portionofthepituitaryglandcanbevisualized.Thepituitary glandcanbegentlydisplacedfromitslocationwithinthesellato permitinspectionofthecircumferentialduralinterface.Incision intotheglandmaybenecessarytoretrieveasmallcentrally locatedmicroadenoma(dashedline). Figure6:Locatingamicroadenomawithinthepituitary parenchymacanbechallenging.Useofcolorandtexture distinctioncanbeusefulindistinguishingadenomafromnative tissue.Anadenomawillhaveasofttextureversusthemorefirm surroundingparenchyma.Theadenomawillbetan-grayto purpleincolorversustheorangesurroundingparenchyma. Figure7:Pituitarymicroadenomascanpossesssurrounding extensionswithintheadjacentcompressedanteriorpituitary tissue,termedthepseudocapsule.Duringtheresectionofa microadenoma,thepseudocapsuleshouldalsoberemovedto betterprovideanendocrinologiccureandpreventadenoma recurrence.Removalofthissmallnativepituitarytissuedoes notimpairanteriorlobesecretoryfunction. Figure8:Followingcompleteresectionofthepituitary microadenomaandpseudocapsule,theresectioncavityis examinedforpersistentbleedingordrainageofcerebrospinal fluid.Closureofthesellarfloorshouldbeginwithplacementof anabsorbablepolyethyleneglycolblockeitherintradurallyor extradurallywithsufficientoverhang(dashedlines)overthe drilledmarginofthesellarfloortopreventherniationintothe sphenoidsinus.Thisblockisthencoveredwithanadhesive andfreemucosalgraft.Thismultilayeredclosuredecreasesthe riskofcerebrospinalfluidleakage.Sphenoidsinuspackingwith adiposetissueisnotnecessaryforasuccessfulclosure. Figure9:Coronalviewofamacroadenomaexpandingthesella inferiorlyandlaterally.Theselesionscanalsodemonstrate cavernoussinusextensionandmasseffectontheopticchiasm orhypophysealstalk.Thetranssphenoidalapproachshouldbe consideredfordomeshapedlesionswithsellarandmidline suprasellarinvolvement.Lateralextensionandirregularityofthe superiorsurfaceadjacenttotheinternalcarotidarteryare contraindicationstothetranssphenoidalapproach. Figure10:Axialviewofapituitarymacroadenoma. Figure11:Sagittalviewofapituitarymacroadenoma. Figure12:Thetranssphenoidalapproachtomacroadenomasis similartotheapproachformicroadenomasexcept macroadenomasrequiremoreextensiveremovalofthe sphenoidtofacilitatesurgicalexposure.Thesuperior intercavernousandcavernoussinuscanbereflectedtofurther enhancevisualization.Theresectionofamacroadenomabegins withcentraldebulkingusingaringcurettageorsuction,and subsequentcollapseoftheperipheralmassintotheresection cavity. Figure13:Tumorresectionproceedswithremovalofthe macroadenomaalongthesellarfloorandonthelateral extentthatborderthecavernoussinus.Thelateralextentofthe tumorcanusuallyberemovedwithoutopeningthecavernous sinus. Figure14:Thesuprasellarportionofthetumorwilldropcaudally whentheadenomawithinthesellahasbeenremoved. Identificationofthenativepituitaryglandiscommonlyobserved atthisstageduetoacommonsuperolateraldisplacementofthe glandinthepresenceofamacroadenoma.Aneasilyentered planebetweenthetumorandthenativeglandpermitstheir separation.Ifduringtheresection,foldsofglandand arachnoidareretainedwithintheperiphery,thisisasignof retainedtumorfragments. Meningoencephalocele Figure1:Coronalviewofananteriorfossaencephalocele. Anteriorskullbaseencephalocelesormeningocelescanbe observedbyinstrumentationofthenose.Optimallythe endoscopeshouldbeangled30-to45-degrees. Figure2:Axialviewofananteriorfossaencephalocele. Figure3:Sagittalviewofananteriorfossaencephalocele. Figure4:Initiallyduringtheendonasalapproachtheleftmiddle turbinateisinview.Adjacentstructuresmustberemovedto allowfortheendonasalapproachtoan encephaloceleextendingfromtheethmoidsinus(deepto dashedline).Thesestructuresincludetheuncinateprocess, ethmoidbulla,andlateralnasalwall. Figure5:Themiddleturbinateispreservedandretracted mediallytopermitdeeperdissection.Anethmoidectomyand excisionoftheuncinateprocessfacilitateexposureofthe encephalocele. Figure6:Theencephaloceleshouldbeinspected circumferentiallytoidentifythelocationoftheskullbasedefect. Thebonymarginsoftheskullbasedefectneedtobeexposed bycautiouslyremovingthemucosaandskeletonizingthe ethmoidmargins. Figure7:Bipolarcauterizationisusedtoshrinkthe encephaloceleuntiltheremnantcanbereducedinto theadjacentskullbasedefect. Figure8:Theadjacentmucosatotheskullbasedefectis removedtopermitvisualizationofthemargins.Abonyor cartilagenousplate(dashedline)shouldbeplaced intracraniallytocovertheskullbasedefectforanydehiscence greaterthan5mmindiameter.Thenasalseptumoran absorbableprostheticplatearemostcommonlyusedforthis purpose. Figure9:Theclosureiscompletedwithplacementofanasal mucosalgraftoverthedehiscentskullbaseandplateinsert.A nasalspongecanbeplacedtomaintainpressureonthe underlyingmucosalgraft. TransphenoidalDrainageofaPetrousApexCholesterol Granuloma Figure1:Axialviewofapetrousapexcholesterolgranuloma thatextendsmedialtotheinternalcarotidartery.Themedial abutmentofthesphenoidsinus(SS)makesthetranssphenoidal routefavorablefordrainage. Figure2:Adistortmentoftheposterolateralwallofthesphenoid sinusisinducedbythemedialextentionofthepetrousapex cholesterolgranuloma. Figure3:Atranssphenoidendoscopicapproach,permits incisionandevacuationofthecholesterolgranuloma. Figure4:Axialviewofapetrousapex cholesterolgranulomathatextendsmedialtotheinternalcarotid artery.Despitenothavingasextensiveabutmentwiththe sphenoidsinus,thislesioncanstillbeincisedandevacuated viaatranssphenoidalapproach. Figure5:Theposteriorwallofthesphenoidsinusmustbe opened(dashedline)topermittheexposurenecessaryto evacuatethecholesterolgranuloma. Figure6:Anangleddrillisusedtoremovetheboneliningthe posteriorsphenoidsinus. Figure7:Anincisioninthewallofthecholesterol granulomashouldbemadewidelytoavoida stenoticevacuationroute. Figure8:Axialviewofapetrousapex cholesterolgranulomathatdoesnotextendtothemedialmargin oftheinternalcarotidartery.Thismakesthetranssphenoidal approachtoincisionandevacuationnotanoptionforthis configurationofacholesterolgranuloma. AllimagesarecopyrightbyRKJackler.Permissiongrantedfornonprofiteducationaluseofimages,withattributiontotheirsource. Createdby:RobertJackler(surgeon)andChristineGralapp(artist) Withcontributionsby:NikolasBlevins,GriffithHarsh,Michael Kaplan,LawrencePitts,CharlesYingling,&CoreyMass http://med.stanford.edu/sm/ohns-skull-base-surgery-atlas/