Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
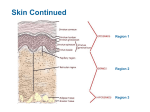
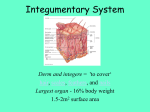
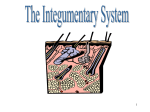
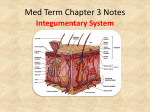
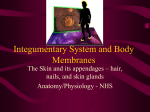
IN THE NAME OF GOD SKIN AND ORAL MUCOUS MEMBRANE GOALS Students can explain the anatomy and physiology of skin and oral cavity They can demonestrate the key point of assessment They know current disease of skin and oral mucous membrane They can explain about pressure sore and its treatment They know apropriate nursing diagnosis and outcoms ANATOMIC AND PHYSIOLOGIC OVERVIEW THE LARGEST ORGAN SYSTEM OF THE BODY , THE SKIN,IS ESSENTIAL FOR HUMAN LIFE . ANATOMY OF THE SKIN,HAIR ,NAILS AND GLANDS OF THE SKIN I Skin The Integumentary System THE SKIN IS COMPOSED OF THREE LAYER : 1-EPIDERMIS 2-DERMIS 3-SUBCUTANEOUS TISSUE OR HYPODERMIS Three Layers of skin: Epidermis: Stratified squamous epithelium; outer layer is "keratinized" or "cornified" Dermis: Dense irregular connective tissue Hypodermis: Adipose connective tissue Epidermis: Avascular. Depends on blood vessels in underlying dermis for its nutrition Cells formed by mitosis in deepest, or basal, layer, then get pushed into more superficial layers Primary cell type in epidermis = keratinocytes which produce large amounts of protein keratin Other cell types: Melanocytes produce pigment melanin & transfer it to keratinocytes Langerhans cells (really macrophages) clean up debris Merkel cells detect touch and pressure; transfer this information to sensory receptors in the dermis Dermis: Dense irregular connective tissue Separated from epidermis (stratified squamous epithelium) by basement membrane Highly vascular Highly innervated Two Layers: Papillary layer just below epidermis Reticular layer forms deep 80% SUBCUTANEOUS TISSUE (HYPODERMIS) Subcutaneous tissue (hypodermis) is deep to dermis Anchors skin to underlying organs, bones and muscles Contains half of the body’s fat; acts as padding and insulation. Appendages of the skin Hair follicles and hair Sweat glands Sebaceous (oil) glands Nails on fingers and toes Hair - Distribuled over all skin except: palms of hands soles of feet nipples glans of penis & clitoris minor labia - Formed in follicles located deep in dermis Shaft Root Bulb Each hair is associated with: One or more sebacious (oil) glands An arrector pili muscle A plexus of nerves around the root Nails: - Tips of fingers and toes - Thick layer of densely packed keratinocytes - Produced by nail matrix at proximal end Deeper layers of epidermis = nail bed Average growth: 0.5 mm per week Sebaceous (oil) glands: - Branched tubular glands - Duct opens into opening of hair follicle - Secretes sebum, consisting of lipids, proteins, ions, carbohydrates, Sweat Glands - 2 to 3 million - Two types: Merocrine: Distributed over all skin except nipples (Eccrine) Simple coiled glands in dermis Duct leads to sweat pore on surface Secreted watery sweat for cooling Apocrine: Located only in axillary, pubic, anal regions Larger than eccrine glands Duct opens into opening of hair follicle Secretes thicker sweat, high content of proteins and fats. SKIN FUNCTIONS Mechanical/Chemical damage – keratin toughens cells; fats cells cushion blows; and pressure receptors to measure possible damage Bacterial damage – skin secretions are acidic and inhibit bacteria. Ultraviolet radiation – melanin produced to protect from UV damage SKIN FUNCTIONS Thermal control – regulates body temperature Heat loss: sweat to cool the skin Heat retention: prevents blood to rush into capillary beds Waterproofing – contains lipids to prevent drying out Excretion of waste – urea and uric acid secreted in sweat Makes vitamin D – modifies cholesterol molecules in skin and converts it to vitamin D SKIN FUNCTIONS Covers the internal structures of body Senses temperature, pain, touch, pressure Promotes wound repair-cell replacement OLDER ADULT SKIN Skin atrophies - dec. sebum, dec. sweat Skin drier, flattens - paperlike Elasticity decreases and wrinkles develop’ Dec. melanocyte function-grey hair, pale, age spots. Dec. axil, pubic,scalp hair Inc. facial hair; men - ears, nose VARIATIONS ACROSS THE LIFESPAN: ELDERLY CHANGES R/T AGING Physiological change ↓ SQ tissue Loss of collagen and elastic fibers ↑ Capillary fragility ↓ sweat gland activity Over exposure to sun Loss of or inefficiency of melanocytes INTEGUMENTARY SYSTEMHEALTH HISTORY o o o o o o skin colour change any past skin problems temperature changes texture changes sweating any masses including warts or moles (nevi) INTEGUMENTARY SYSTEMHEALTH HISTORY o o o o o changes in masses, warts, nevi – also, cosmetic concerns and physical discomfort rashes or eruptions changes in hair texture or oiliness, hair loss, dandruff, hair bleaching, dyeing management of any problems with hair or scalp medications INTEGUMENTARY SYSTEMHEALTH HISTORY o o o complaints of tenderness, flakiness, itchiness, lumps, sores on scalp, bleeding problems with nails including breaking, ingrown nails, nail biting Self-care behaviours REVIEW OF SYSTEMS o A series of questions : pt’s current and past health including health promotion practices o Inquires about signs and symptoms as well as diseases related to each body system 28 HEALTH HISTORY: SKIN o o o o o o o How?When? did the changes occur? Is it a skin rash or lesion? One area or has it spread? Bleeding or drainiage from the area? Does the area itch? How much time do you spend in the sun? How do you protect from the UV rays? o (continued) HEALTH HISTORY: SKIN o o o o o o Allergies? Family hx of skin cancer or significant disease? Fever or joint pain, or weight loss? Recent insect bite? Do you take medications or herbal preparations? What changes in your skin have you observed in the past few years? HEALTH HISTORY: HAIR o o o o o o When did first notice loss (gain)? Sudden or gradual? Few spots or all over body? What was happening in your life? Any dyes, medications or herbal preparations? Did you experience itching pain, discharge, fever, weight loss? Any serious illness? HEALTH HISTORY: NAILS o o o o o When did you first notice? What type of changes have you noticed? Sudden or gradual? Other signs - bleeding,or discharge? What is normal condition of your nails? PHYSICAL ASSESSMENT WHAT ARE THE GENERAL CHARACTERISTICS OF THE SKIN THAT SHOULD ALWAYS BE NOTED? Inspection and Palpation of the skin SKIN Inspect: Color Integrity Lesions Primary Secondary Vascular Palpate Moisture Temperature Texture Turgor/elasticity Tenting INSPECTION Color: Depositions of abnormal pigments Jaundice from bilirubin Carotenemia from carotene excess ingestion of yellow vegetables (carrots) Gray from heavy metals (Au-gold, Ag- silver,Bi-bismuth) INSPECTION natural lighting preferred, need complete exposure of all skin surfaces. remember to scan nails, hair, mucous membranes Location and Distribution exact, measure, symmetry? INSPECTION Color: variation common, even within same person. Melanin maybe diffuse or localized increased: Addison’s Disease, hyperthyroidism, pregnancy, sunlight exposure decrease: albinism Erythema appearance of increased amounts of oxygenated blood in dermal vasculature INSPECTION Color: Cyanosis blue tint from venous blood (deoxygenated hemoglobin) seen associated with congestive heart failure, pneumonia Chapter 4 ecchymosis, petechiae Extravasation of blood products Pallor decrease hemoglobin in vessels close to skin secondary to anemia, shock INSPECTION Morphological structure primary lesions flat elevated -- serous filled -- pus filled -- solid INSPECTION Morphological structure secondary lesions loss of skin -- erosion -- ulcer -- fissure build-up of skin -- crust -- lichenification -- scar HOW DO YOU EXAMINE A LESION? Palpate, wear gloves Roll nodule between thumb and forefinger to assess depth Does it blanche with pressure or when stretched? SKIN LESIONS SKIN LESIONS SKIN LESIONS PALPATION Temperature localized hyperthermia from increased blood flow due to cellulitis or injury generalized hyperthermia due to fever of systemic infection, hyperthyroidism localized hypothermia caused by peripheral arteriosclerosis, Raynaud’s disease generalized hypothermai due to shock PALPATION Moisture Dryness(hypothyroidism), lubricity(acne) Texture quality character rough smooth (hyperthermia) PALPATION Elasticity decreases with age Decreased skin turgor - dehydration edema - accumulation of fluid in interstitial spaces under the skin. ASSESSING SKIN TURGOR EDEMA Edema is defined as a clinically apparent increase in the interstitial fluid volume Weight gain precedes overt edema EDEMA Pitting edema Non-pitting edema PITTING EDEMA SCALE Return to baseline 2-5 minutes Depth of indentation 8mm description severe +4 1-2 minutes 6mm moderate +3 10-15 seconds 4mm mild +2 Disappears rapidly 2mm trace +1 scale HAIR Inspect Color Quantity Distribution Condition of scalp Lesions or pediculosis Palpate Texture Scalp NAILS Inspect Color Condition Angle of attachment Abnormalities Palpate Texture Consistency Thickness Adherence to nailbed INTEGUMENTARY ASSESSMENT: DIAGNOSTIC EVALUATION Skin Biopsy Patch testing Scabies scrapings Tzanck Smear Wood’s Light Examination Skin culture What is wood’s light? Give two uses for it and what are the findings? TYPES OF WOUNDS AND LOCATION Pressure: Venous: sacrum, heels, trochanter Inside the leg -Medial -Lateral Diabetic: neuropathic areas Traumatic: anywhere WOUNDS Abrasion – skin is rubbed or scraped off Lacerations – torn, ragged, irregular edges made by blunt objects Avulsions – the tearing away of tissue from a body part Incisions – cuts made by sharp cutting instruments Punctures – caused by objects that penetrate tissue while leaving a small surface opening Amputations – traumatic is the nonsurgical removal of a limb from the body BURNS Leading cause of accidental death Classified by depth of tissue involvement 1st degree—involves epidermis only 2nd degree—involves epidermis and some dermis 3rd degree—involves epidermis, dermis and some deeper tissue are destroyed 1st and 2nd degree burns are considered partial thickness burns, and 3rd degree is a full thickness burn BURNS 1st degree – partialthickness (superficial) 2nd degree – partialthickness (deep) 3rd degree – fullthickness NURSING DIAGNOSIS AND INTERVENTIONS IMPAIRED SKIN INTEGRITY RELATED TO; Inflammation of dermal-epidermal junctions Decreased blood and nutrients to tissues Imposed immobolity Mechanical irritants or pressure Chemical trauma Environmental irritants Dry , thin skin and decreased dermal vascularity Poor hygiene INTERVENTIONS Identify causative factors Example; hard,supporting sleep or sitting tissue Removal of adhesives Profuse diaphoresis Pressure dressing Fixation devices Bladder and bowel incontinence Ng tubes Prolonged sitting or lying in same position Sensory,motor deficits REDUCE CAUSATIVE FACTORS IF POSSIBLE MECHANICAL IRRITANTS OR PRESSURE Encourage highest degree of mobility to avoid prolonged periods of pressure Change position at least every 2h Frequently supplement full-body turns with minor shifts in body weight Reduce environmental source of pressure(drains, tubes, dressings) Use lift sheet to reposition client Keep client clean and dry MECHANICAL IRRITANTS OR PRESSURE Keep cast edges smooth and away from skin surfaces Apply padding over bony prominence Protect skin around feeding tubes with a protective barrier Instruct to report discomforts Teach client/significant other appropriate measures to prevent pressure or friction DECREASED BLOOD AND NUTRIENTS TO TISSUES Increased portein-carbohydrate intake sufficient to prevent negative nitrogen balance, hypoalbuminemia , and weight loss . Increased daily intake of vitamins and minerals Adequate oxygen supply and the blood volume and ability to transport it Consult a dietitian Weigh the person daily POOR HYGIENE patients sheets be dry and clean Remove any discharges from patients skin as soon as possible Don’t share personal tools such as towel with other patients Wash linens and clothes with hot water if possible Bath patient by tepid water and mild soap daily Lubricate the patients skin with lotions if there isnt any contraindicate QUESTIONS? REFRENCE Potter-pory-2009-fundamentals of nursing –page12781342 Morton,patricia and k.fontaine -2009-critical care nursing a holistic approach page610-613,1313-1349 Hokanson.jane-2009-medical surgical nursing clinical management for positive outcoms-page2208-2210 Brunner suddarth’s-2010-text book of medical-surgical page1658-1751 Moyet-lynda jula-2009-health assessment for nursing practice-page111-148 PRODUCED BY; Zahra Abbas Ali Madadi and Maryam Sharifi The students of M.S in C.C.N