Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
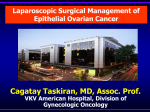
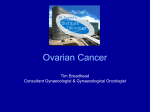
Gynecologic Oncology 135 (2014) 595–605 Contents lists available at ScienceDirect Gynecologic Oncology journal homepage: www.elsevier.com/locate/ygyno Review Primary debulking surgery for advanced ovarian cancer: Are you a believer or a dissenter? John O. Schorge a,⁎, Rachel M. Clark a, Susanna I. Lee b, Richard T. Penson c a b c Vincent Gynecologic Oncology Service, Massachusetts General Hospital, USA Division of Abdominal Imaging, Massachusetts General Hospital, USA Division of Medical Gynecologic Oncology, Gillette Center for Gynecologic Oncology, Massachusetts General Hospital, USA H I G H L I G H T S • The goal of primary debulking surgery should be the complete resection of all macroscopic disease. • Neoadjuvant chemotherapy has an emerging role in the treatment of selected patients. • Preoperative innovations under investigation are aimed at better triaging women to upfront surgery or chemotherapy. a r t i c l e i n f o a b s t r a c t Article history: Received 8 September 2014 Accepted 7 October 2014 Available online 12 October 2014 Nothing stirs the collective soul of primary debulking surgery (PDS) advocates like hard data suggesting equivalent outcomes of neoadjuvant chemotherapy (NAC). These opposing views have even metaphorically come to blows at the highly entertaining “SGO Fight Night” that took place during the 2008 Annual Meeting on Women's Cancer, replete with teams supporting each of the would-be gladiators. Decades of retrospective data supporting the clinical benefit of PDS has recently been challenged by the publication in 2010 of a randomized phase III trial conducted in Europe supporting the clinical efficacy of NAC. Naturally, a firestorm of criticism among believers ensued, yet practice patterns within the United States did slowly change, suggesting an emerging block of dissenters. Another randomized phase III European trial, as presented in abstract form in 2013, showed similar findings. Few other topics within the field of gynecologic oncology have participants so entrenched in the “corners” of their existing practice patterns. This review attempts to consolidate the current evidence supporting both sides so that the patient can be declared the winner. © 2014 Elsevier Inc. All rights reserved. Keywords: Primary debulking surgery Neoadjuvant chemotherapy Advanced ovarian cancer Contents Introduction . . . . . . . . . . . Primary debulking surgery . . . . Neoadjuvant chemotherapy (NAC) PDS v NAC: phase III trials . . . . Special circumstances . . . . . . The elderly . . . . . . . . . Obesity . . . . . . . . . . . Stage IV disease . . . . . . . Clinical innovations . . . . . . . Preoperative imaging . . . . . Minimally invasive surgery . . Ultra-radical surgery . . . . . Synopsis . . . . . . . . . . . . Future strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 596 596 598 598 599 599 599 599 600 600 601 602 602 602 ⁎ Corresponding author at: Vincent Gynecologic Oncology Service, Massachusetts General Hospital, Harvard Medical School, Yawkey-9E, 55 Fruit St, Boston, MA 02114, USA. Fax: +1 617 726 6898. E-mail address: [email protected] (J.O. Schorge). http://dx.doi.org/10.1016/j.ygyno.2014.10.007 0090-8258/© 2014 Elsevier Inc. All rights reserved. 596 J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Introduction The consistent inability to reliably detect ovarian cancer before widespread metastases has proven to be logistically problematic and a source of ongoing disappointment. Unfortunately, routine screening has not been shown to meaningfully improve early detection, nor reduce mortality in either the high-risk or general populations [1–3]. The U.S. Preventative Services Task Force currently recommends against screening given the scant evidence for any benefit, but consistently observed harms from unnecessary interventions [4]. Symptoms of ovarian cancer tend to be vague and are often attributed to menopause, stress, or functional bowel problems. Substantial delays prior to diagnosis are very common, often until an abdominal-pelvic computed tomography (CT) scan is obtained. As a result, two-thirds of women who are newly diagnosed with invasive epithelial ovarian cancer still present, as they always have, with stage III–IV disease typically characterized by ascites, carcinomatosis and omental caking. Advanced ovarian cancer is a heterogeneous disease requiring a disciplined sequence of treatment to consistently achieve the best outcomes. No two clinical presentations are quite the same, nor would two different clinicians necessarily be in sync on every patient. Whether to start with an operation, or platinum-based therapy, is not always obvious, no matter what the pre-existing biases. Primary debulking surgery (PDS) requires knowledge of the disease process, mastery of a wide spectrum of different procedures, and the willingness to manage complex postoperative sequelae. Neoadjuvant chemotherapy (NAC) appears to involve less short-term morbidity, and has demonstrated equivalent efficacy, at least in one published phase III trial [5]. Clinical teams are charged with the challenging task of striking the perfect balance between being appropriately aggressive and trying to avoid unnecessary morbidity. The most strident advocates of either PDS or NAC will have treated selected patients with the alternative on at least some occasions. This intriguing frequency of crossover is well-known, but not often stated. Due to the complexities of providing longitudinal care for patients with ovarian cancer, better outcomes are reported when a subspecialist is involved [6,7]. Unfortunately, fewer than half of patients in the United States and Europe will have that opportunity [8]. Instead, the majority are managed by physicians not necessarily intimately familiar with the interplay between medical and surgical management. However, maximizing overall survival depends on the precise coordination of both forms of treatment at a center with expertise. PDS and NAC each have their believers and dissenters. Recently, decades of retrospective data supporting the former has collided with phase III data supporting the latter position. Apropos to the boxing analogy, we cannot retreat into our corner at this point, but must be willing to go the distance with the best currently available evidence for the benefit of all women diagnosed with advanced ovarian cancer. Furthermore, we must look for ways to improve our treatment paradigms. and other retrospective data rapidly accrued thereafter to establish PDS as the de facto standard of care for advanced ovarian cancer [11–13]. Removal of the uterus, ovaries and any other intra-abdominal tumors as part of ovarian cancer treatment is an easy concept for patients and their families to understand. Often there is an unrealistic assumption that taking out the offending site of origin will stop the spread of cancer, and that peritoneal dissemination includes a finite number of tumors that once removed, will not return. The actual clinical benefits of debulking have been harder to prove in a rigorous fashion. Within the broader field of oncology, this type of aggressive surgical approach to widely metastatic disease has some parallels, especially when complete cytoreduction can be achieved [14–17]. Several supportive, but mostly theoretical, arguments have been proposed to justify the biological plausibility of debulking (Table 1) [18,19]. Disseminated ovarian cancers, like other solid tumors, are postulated to contain a small subpopulation of highly specialized cells with self-renewal capacity and the potential to reconstitute the entire cellular heterogeneity of a tumor. These ovarian cancer stem cells are thought to be responsible for tumor initiation, maintenance and growth. Presumably, ineffective targeting of this cell population is responsible for the therapeutic failures and tumor recurrences frequently observed [20,21]. The elimination of these chemo-resistant cells, removal of the supportive tumor microenvironment, and potential for improved drug delivery, are, in theory at least, other benefits of surgical cytoreduction. Additionally, removal of bulk disease should reduce the number of Primary debulking surgery Joe V. Meigs, a gynecologic surgeon at the Massachusetts General Hospital (Fig. 1), initially described ovarian tumor debulking in 1934 [9]. The initial intent was to enhance the effects of radiation therapy in an era before modern chemotherapeutics. However, due to limited clinical benefit, the concept did not really gain traction until the mid-70s when platinum drugs were emerging. Griffiths' (Fig. 2) landmark study appeared to conclusively demonstrate the inverse relationship between residual tumor diameter and patient survival [10]. Case series 603 603 Fig. 1. Joe V. Meigs. J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 Fig. 2. C. Tom Griffiths. chemotherapy-treated cancer cells that will undergo spontaneous mutations to drug-resistant phenotypes [22]. PDS is a technically challenging endeavor for a number of different reasons. Tumor-related sequelae such as symptomatic pleural effusions or hypoalbuminemia, especially when accompanied by co-existing health problems, often impact the ability to recover from any major surgical procedure. Within the peritoneal cavity, anatomical landmarks are often encased by tumor or otherwise obliterated. Routinely, radical pelvic dissection, bowel resection, and aggressive upper abdominal surgery are necessary to achieve an optimal result [23]. Sound clinical judgment is required in order to be appropriately aggressive, without inducing a cascade of potentially disastrous complications. Despite the accumulated evidence supporting the importance of PDS, it remains controversial whether the better outcome is due to the surgeon's technical proficiency or some ill-defined, intrinsic feature of the cancer that makes the tumor implants easier to remove [24,25]. While patients definitely do appear to benefit from one maximal debulking attempt, the timing of the operation and what defines success have become increasingly controversial. Proficient cytoreduction depends on numerous factors, including patient selection, tumor location, and surgeon expertise. To achieve a Table 1 Theoretical arguments for debulking surgery. Removing large necrotic masses promotes drug delivery to small tumors with good blood supply Removing resistant clones decreases the likelihood of early onset drug resistance Tiny implants have a higher growth fraction that should be more chemo-sensitive Removing cancer in specific locations, such as tumors causing a bowel obstruction, improves the patient's nutritional and immunologic status 597 survival benefit, an optimal result was initially defined as no residual tumors individually measuring more than 2 cm in size [26]. For purposes of uniformity, the Gynecologic Oncology Group (GOG) re-defined optimal debulking as residual implants ≤1 cm [27]. For some decades, this criterion served as the benchmark of success. Patients undergoing PDS who were rendered optimal (≤ 1 cm residual disease), followed by intraperitoneal (IP) platinum-based chemotherapy were shown to have a median overall survival of 66 months — the longest duration ever reported in a phase III study [28]. The clinical outcomes achieved in this GOG trial still serve as the benchmark for comparisons with any other sequence of treatment. Yet one valid criticism of cytoreductive surgery is the biased, subjective assessment of gross residual disease by the surgeon at the completion of the operation. Due to tissue induration, inadequate exploration, radiologist over-estimation, or other factors, inaccuracies of residual tumor size are common [29,30]. Perhaps due to the inability to reliably quantify the remaining disease, a recent sub-analysis of accumulated data from several prospective GOG trials demonstrated that patients with 0.1 to 1.0 cm residual disease had only marginally improved overall survival compared to patients with N1 cm residual disease for stage III ovarian cancer. In fact, dramatic survival benefit was only achieved with complete resection to microscopic residual disease [31]. Based on these findings and other similar reports, there is a growing consensus that optimal cytoreduction should be defined using a more stringent criterion. Thus, the current goal of PDS is to achieve complete resection with no residual disease [32]. Raising the bar for surgical success accordingly decreases the proportion of patients with advanced ovarian cancer in which this redefined optimal result can be accomplished, unless there is a change in practice. For stage IIIC disease, rates of complete resection predominantly range from 15 to 30%. However, the clinical benefits appear substantial when it can be achieved (Table 2) [33–35]. Within the last decade, multiple institutions have demonstrated the ability to revise their surgical paradigm in order to safely debulk to no residual disease at a rate that approaches or exceeds 50% [36–38]. Broader incorporation of these types of surgical improvement programs could significantly improve outcomes. In a meta-analysis of 18 studies involving 13,257 patients, Chang et al. observed that each 10% increase in the proportion undergoing complete cytoreduction was associated with a 2.3-month increase in cohort median survival. Additionally, for each 10% increase in the proportion receiving IP chemotherapy, there was a 3.9-month increase in median cohort survival time [39]. Recently, Rosen et al. reported an astonishing seven-year survival rate of 90% in women undergoing PDS with no residual disease who subsequently received IP treatment [40]. All attempts should be made to achieve complete (hereafter defined as optimal in this review) resection, as these patients, when treated with adjuvant platinum-based IP chemotherapy have survival measures that exceed any rates previously seen in this population [41]. However, despite the subjective nature of classifying residual disease, there is evidence to support minimizing the amount of remaining tumor as much as possible. Chi et al. analyzed a prospective database for outcomes of 465 women with stage IIIC ovarian cancer who underwent PDS. They observed a median overall survival of 33–34 months for those with N1 cm residual disease, 48 months with 0.6–1.0 cm residual, Table 2 Median overall survival of stage IIIC ovarian cancer patients undergoing primary debulking surgery (months). Study Residual disease Microscopic 0.1–1.0 cm N1 cm Aletti [33] Chang [34] Chi [35] N84 86 106 34 46 59 25 37 33 598 J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 66 months for those with ≤.5 cm, and 106 months for patients with no gross residual disease [35]. Additionally, in a Cochrane Database review of 11 retrospective studies, “near optimal” patients with b1 cm residual disease collectively had better outcomes than “suboptimal” cases with residual disease N1 cm [42]. Occasionally, a gynecologist planning to remove an adnexal mass or a general surgeon performing abdominal surgery for presumed bowel obstruction unexpectedly encounters widespread intra-abdominal disease. These advanced ovarian cancer patients who are unintentionally taken for surgery typically do not get a maximal cytoreductive effort, but are oftentimes referred postoperatively. Fortunately, upfront reoperation before the start of chemotherapy should still be feasible, and successful, in more than half of patients with incomplete primary surgery elsewhere [43]. If it were possible to perform PDS and consistently achieve no residual disease with limited postoperative complications, then we all would be believers in this strategy. Despite attempts to develop such a model – predicting successful surgery with minimal morbidity – nothing yet has proven reproducible in a prospectively validated manner [44,45]. At present, the reality is that most patients will have some level of remaining tumor, and many will derive limited clinical benefit. Additionally, PDS may result in a prolonged postoperative recovery that is fraught with complications: an observation frequently made by dissenters to the upfront surgery paradigm. All too often, the initiation of chemotherapy may be delayed, or worse, postponed indefinitely. Neoadjuvant chemotherapy (NAC) Some patients are clearly too medically ill to initially undergo any type of upfront abdominal operation, whereas others have disease that is too extensive to be resected even by an experienced ovarian cancer surgical team. In these circumstances, NAC is routinely used after the diagnosis has been confirmed. Core biopsy of the primary tumor or one of the metastases is the gold standard to prove the existence of a disseminated ovarian carcinoma. Cytological diagnosis by fine needle aspiration may also be acceptable if the CA125/CEA ratio is N25 (as defined in trials) [46]. Following three to four courses of treatment, the feasibility of surgery can be reassessed. In some retrospective series, NAC followed by interval debulking has demonstrated comparable survival outcomes to those reported for primary surgery [47–50]. Fewer radical procedures may be required, the rate of achieving minimal residual disease may be higher, and patients may experience less morbidity. Six cycles of NAC prior to surgery are another less commonly used option. In 82 patients treated with this extended regimen, the rate of complete resection to no residual disease was 63.7%, and 23.1% were found to have had a clinical complete response [51]. However, a metaanalysis of 81 cohorts of 6885 patients with stage III or IV ovarian cancer suggested that NAC in lieu of PDS is associated with an inferior overall survival [52]. Direct comparison has historically been difficult to perform. Unfortunately, preoperative CA125 levels, imaging tests and physical examinations all have limitations in consistently identifying which patients can be optimally debulked to no residual disease by a gynecologic oncologist. Invariably, the final determination cannot be made until abdominal exploration. When it is clinically evident during surgery that achieving b1 cm is not feasible, great discretion is required to confirm the diagnosis, but not provoke unnecessary complications that could delay subsequent therapy. Two phase III trials were conducted to determine whether a second interval debulking procedure was worthwhile after an unsuccessful initial attempt followed by a few courses of chemotherapy. A multicenter trial conducted in Europe demonstrated a 6-month median survival advantage in patients who were re-explored after three cycles of chemotherapy [53]. In contrast, no survival advantage was demonstrated when a similar study was conducted in the United States [54]. These seemingly conflicting reports are most easily explained by clarifying who performed the first surgery. In the US trial, virtually all patients had their initial attempt by a gynecologic oncologist, unlike the European study where relatively few had their first surgery performed by a subspecialist. Therefore, interval debulking appears to yield benefit only among the patients whose primary surgery was not performed by a gynecologic oncologist, if the first try was not intended as a maximal resection of all gross disease, or if no upfront surgery was performed at all [55]. PDS v NAC: phase III trials In 1986, the GOG and separately a collaborative group in the Netherlands each opened randomized phase III trials to test the hypothesis that primary debulking was superior to NAC in advanced ovarian cancer. Both studies were closed due to poor accrual. One prevailing opinion at the time was that clinicians did not want to subject their patients to ‘substandard’ NAC treatment. Until recently, the presumed benefits of primary surgical cytoreduction in advanced ovarian cancer had not been rigorously tested. The results of the randomized European Organization for Research and Treatment of Cancer (EORTC protocol # 55971) phase III trial were first presented in October 2008 and subsequently published in September 2010. The data has fostered debate of how best to initially treat women with advanced ovarian cancer. In the study, 670 patients were randomized to PDS versus NAC. After three courses of platinumbased treatment, the 90% of NAC patients who demonstrated a response underwent interval debulking. The authors reported a median overall survival of 29 to 30 months, regardless of the initial assigned treatment group. In the multivariate analysis, complete resection of all macroscopic disease at debulking surgery was identified as the strongest independent prognostic factor, but the timing of surgery did not seem to matter. Based on the authors' interpretation of their data, NAC and interval debulking was the preferred treatment [5]. Despite these findings, the Society of Gynecologic Oncology members queried in 2010 largely remained unconvinced. Of respondents to a survey sent to the membership, most use NAC in less than 10% of advanced stage ovarian cancer cases [56]. In light of the phase III data, some European gynecologic oncologists have openly questioned what kind of evidence would be needed to convince their US colleagues about the superiority of the NAC approach [57]. At least two criticisms of the trial have been suggested as reasons why the results may not be applicable in the United States. First, the duration of patient survival in the study was shorter than expected. The median survival (29 to 30 months) was less than half that reported for optimally debulked stage III patients receiving postoperative intraperitoneal chemotherapy (66 months) [28]. Additionally, only 42% of those patients randomized to PDS had ≤1 cm of residual disease. Since expert centers in the United States often report achieving cytoreduction to ≤ 1 cm of residual disease at least 75% of the time, it is feasible to think that a more aggressive initial attempt might have led to a better outcome for the group randomized to surgery. Chi et al. analyzed the outcomes of patients treated with PDS at the Memorial Sloan-Kettering Cancer Center during the same time period in which the EORTC trial was conducted, using identical inclusion criteria. Of 316 eligible patients, 285 (90%) underwent PDS. In 203 patients (71%), ≤1 cm of residual disease was achieved with an overall median overall survival of 50 months [58]. The long-term outcomes were intriguing, but whether this was a fair comparison has been debated [59]. A second recently presented study is also of interest. The Medical Research Council (MRC) CHemotherapy OR Upfront Surgery (CHORUS) trial is a phase III, non-inferiority randomized controlled study conducted in the United Kingdom and New Zealand. Five hundred fifty-two newly diagnosed advanced ovarian cancer patients with suspected stages III–IV ovarian cancer were enrolled between March 2004 and August 2010. Women were randomized to undergo PDS followed by 6 cycles of chemotherapy, or NAC with interval debulking surgery J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 599 after 3 cycles, followed by completion chemotherapy. The primary outcome was overall survival, with secondary outcomes of toxicity and quality of life. Complete resection was achieved in 16% of the PDS arm versus 40% in the NAC arm. Grades 3–4 postoperative adverse events (24% v 14%) and death (5.5% v 0.5%) within 28 days of surgery were both more common in the PDS group. Median overall survival was comparable between the two arms: 22.8 months for the PDS arm and 24.5 months for the NAC group [60]. Peer-review of the manuscript is eagerly awaited as it represents another meaningful contribution to the literature on this topic. Ultimately, a prospective phase III trial conducted within the United States will need to be performed to sway opinion and markedly change the practice of gynecologic oncologists in this country. Unfortunately, recent attempts through the GOG or with industry support have not yet been successful in launching. Meantime, the controversy will persist and individual patterns of care will continue. PDS is certainly the standard of care for patients with stage IIIA and IIIB ovarian cancer. PDS is also favored for those with IIIC disease, in the absence of evidence for unresectability or poor performance status. The treatment of stage IV is typically individualized in current patterns of practice, but NAC is a reasonable alternative [61]. aged ≥65 years who had PDS for stage III or IV epithelial ovarian cancer between 1995 and 2005. The overall 30-day mortality was a sobering 8.2%. Advancing age, increasing stage, and increasing co-morbidity score were all associated with an increase in 30-day mortality [67]. Wright et al. analyzed the SEER-Medicare database to identify women aged ≥ 65 with stages II–IV ovarian cancer who survived at least 6 months from the date of diagnosis. A total of 9587 patients were identified who received treatment from 1991 to 2007. Interestingly, the use of primary surgery decreased from 63.2% to 49.5% over time. In addition, overall survival with NAC did not differ from PDS in this older population [68]. In an analysis of 28,651 women undergoing surgery for ovarian cancer from 1998 to 2007 using the Nationwide Inpatient Sample, complication rates increased with age from 17.1% in those b50 years of age to 31.5% in those ≥80. Morbidity was observed to be greatest in the elderly, where the effects of age and the number of radical procedures performed had an additive effect on complication rates [69]. En masse, the data suggests that NAC will likely continue to have a more prominent role in the elderly. When complete cytoreduction is not feasible during PDS, the operation should be limited in scope to avoid unnecessary postoperative morbidity as ultra-radical procedures can be especially poorly tolerated in this population. Special circumstances Obesity The elderly The epidemic of obesity taking place in the United States and throughout much of the world is increasingly going to impact the treatment of ovarian cancer. While studies exploring the association between obesity and ovarian cancer survival have yielded conflicting results [70–74], using a body mass index (BMI) of 30 kg/m2 as the tipping point for the definition of obesity hardly seems to reflect reality. In the current vernacular, 40 is the new 30, at least as far as the aging process goes, and we should be able to comfortably extrapolate that also to BMI. Kumar et al. analyzed the Mayo experience with 620 stages IIIC–IV patients who underwent PDS between 2003 and 2011, divided into three groups according to BMI. Women with a BMI of ≥ 40 were found to have substantially higher rates of severe 30-day postoperative morbidity and 90-day mortality after PDS. Although the high BMI group had limited numbers of patients, there did not appear to be deficits in achieving optimal cytoreduction, nor did it impact long-term oncologic outcomes [75]. It seems obvious enough that the likelihood of postoperative complications is demonstrably higher when performing PDS in the morbidly obese population. Even though the ability to achieve complete cytoreduction would seem to be in jeopardy with increasing body size, current data do not bear this out, perhaps due to a mitigating effect of excess body weight on tumor biology [76]. Matthews et al. observed that survival rates were similar between obese and non-obese patients when the amount of residual disease was the same [77]. Regardless, there is a price to be paid for aggressive PDS in the morbidly obese, though NAC too has potential limitations in this population. Wright et al. observed that obese patients treated with chemotherapy on a GOG protocol experienced substantially less toxicity than normal weight women. Substandard drug dosing was thought to be causative [78]. In an analysis of the Australian Ovarian Cancer Study of 333 patients, obese women were significantly more likely to have received b85% of relative dose intensity of carboplatin, leading to worse outcomes [79]. Appropriate dosing for obese patients with ovarian cancer is a must, whether as NAC or given as postoperative adjuvant treatment. When they undergo effective and receive appropriate doses of chemotherapy, obese patients do not have a poorer prognosis [80]. Since the likelihood of a woman developing ovarian cancer increases with every decade, and the population is living longer than ever before, it stands to reason that more and more women will be diagnosed later in life. The precise meaning of the term ‘elderly’ is somewhat fluid, occasionally referring to those as young as 65 years of age, but in some studies defined as 75 years and older. While increasing age as a stand-alone variable should not immediately lead to a more palliative approach, it is a relevant factor as almost half of ovarian cancer patients diagnosed in the United States each year will be at least 65 years of age. Though the exact reasons are usually difficult to separate out and tend to be multifactorial, increasing age does adversely impact survival. As a group, elderly patients with ovarian cancer are less likely to receive care with a gynecologic oncologist, or to undergo PDS followed by adjuvant chemotherapy [62,63]. Some of the differences in patterns of care are likely driven by medical co-morbidities, well-meaning physician bias and/or individual quality of life choices. Increasing age and co-morbid conditions are risk factors for surgical morbidity and mortality, but the interactions have not been rigorously analyzed. Several studies have emphasized that elderly patients are able to tolerate an aggressive approach with relatively few complications, when adjusted for performance status. Langstraat et al. reviewed the Mayo experience of 280 consecutive patients ≥65 years with stage IIIC or IV ovarian cancer treated over a 10-year period. A significant number of elderly women were able to undergo PDS and adjuvant chemotherapy. However, median overall survival still decreased with increasing age and the impact of residual disease was greater on older patients. In addition, 37.5% of patients ≥75 years had significant perioperative morbidity [64]. Glasgow et al. performed a retrospective cohort study of women ≥70 years with stage IIIC or IV disease treated at Yale, and observed that the 42 NAC patients had similar outcomes, but significantly reduced perioperative morbidity compared to 62 women who underwent PDS [65]. Worley et al. reviewed the outcome of 165 patients aged ≥ 70 years at their institution. Median overall survival was similar between the 125 women who underwent PDS, compared to the 40 receiving NAC, but readmission rates within 30 days of surgery was dramatically higher in the PDS cohort (17.6% v 2.5%) [66]. These single institution studies highlight the caution that is indicated for elderly women, especially in the presence of other significant co-morbidities. Thrall et al. analyzed the Surveillance, Epidemiology and End Results (SEER) data -base to identify a cohort of 5475 women Stage IV disease Roughly one-third of patients with advanced ovarian cancer will have stage IV disease at the time of their diagnosis [81]. This designation is widely believed to be associated with a more aggressive tumor biology having significant implications on surgical outcome and response to 600 J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 Table 3 Success rates of primary debulking surgery in stage IV ovarian cancer. Study Aletti [76] Bristow [77] Rauh-Hain [78] Trope [79] Winter [80] Residual disease Microscopic 0.1–1.0 cm N1 cm 6% – 8% 14% 8% 43% 30% 50% 36% 22% 51% 70% 42% 50% 70% chemotherapy. Accordingly, the likelihood of achieving complete cytoreduction at the time of PDS is particularly dismal (Table 3) [82–86]. Furthermore, Winters et al. retrospectively reviewed 360 stage IV patients treated on phase III GOG protocols and did not observe a benefit with 0.1 to 1.0 cm residual disease versus those with 1.1 to 5.0 cm residual. They concluded that ultra-radical procedures might best be targeted to those selected patients in whom microscopic residual disease is achievable [86]. Based on the available data, this would seem to apply to less than 1 in 10 patients. Van Meurs et al. used data from the EORTC 55971 trial to report that patients with stage IV disease and large (defined as N 45 mm) metastatic tumors treated with NAC had demonstrably higher survival, compared to an attempt at PDS followed by postoperative chemotherapy [87]. In addition, NAC patients with stage IV disease who subsequently undergo interval debulking surgery appear to have less peri-operative morbidity, a higher likelihood of complete resection and shorter hospital stay [88]. In the EORTC trial, 10% of patients randomized to NAC never had a cytoreductive attempt [5]. Another advantage of NAC in this high-risk population appears to be the ability to better triage only responding patients to interval debulking surgery. Among this subset, aggressive cytoreduction has been shown to be beneficial [89]. While historically the stage IV subcategory represented a range of clinical findings lumped together, since January 2014 these have been separated out to better reflect the disease processes [90]. It will be of interest to see whether having stage IVA or IVB disease will have implications on the success of upfront treatment. Based on current available evidence, the ability to achieve complete resection to no residual disease is so limited, that upfront surgery should be limited to very select patients, while the majority should be treated with NAC. Clinical innovations Preoperative imaging The ability to reliably identify patients most likely to benefit from PDS based on imaging findings has proven to be an immense challenge. Bristow et al. retrospectively analyzed preoperative CT scans in a blinded fashion and correlated them with surgical outcome to develop a predictive index model [91]. In a similar study, Dowdy et al. identified only diffuse peritoneal thickening and large volume ascites as findings associated with a low rate of optimal debulking [92]. These attempts, and others like them, have not led to a paradigm shift, mainly due to Table 4 Suidan et al. criteria associated with suboptimal primary cytoreductive surgery. Clinical Radiologic Age ≥ 60 years CA125 ≥ 500 U/mL ASAa 3–4 Suprarenal retroperitoneal nodes N1 cm Diffuse small bowel adhesions/thickening Lesion(s) N1 cm small bowel mesentery Lesion(s) N1 cm root of superior mesenteric artery Lesion(s) N1 cm perisplenic area Lesion(s) N1 cm lesser sac a American Society of Anesthesiologists Physical Status classification system. Fig. 3. Ovarian carcinosarcoma with peritoneal carcinomatosis. Coronal image from an abdominal-pelvic CT with oral and intravenous contrast shows a 17-cm primary right adnexal tumor (star). Bulky tumor in the lesser sac (arrow) would suggest the inability to perform complete cytoreductive surgery. variations of image interpretation and surgical expertise across institutions. In a multi-institutional reciprocal validation study, high accuracy rates of CT predictors could not be confirmed [93]. Suidan et al. have recently reported the results of a prospective, non-randomized twocenter trial of 669 patients from 2001 to 2012 that underwent PDS for stages III–IV ovarian, fallopian tube, and peritoneal cancer. Based on three clinical and six radiologic criteria (Table 4, Fig. 3), they developed a predictive model in which the suboptimal rate was directly proportional to the predictive value score [94]. These findings have yet to be validated more broadly. The utility of preoperative whole-body (18)F-fluorodeoxyglucose (FDG) PET/CT is controversial. More accurate detection of supradiaphragmatic disease via imaging might understandably dissuade clinicians from favoring PDS. While fusion PET/CT shows higher staging accuracy than either CT or FDG-PET alone [95–97], the impacts of these findings on rates of successful PDS have yet to be demonstrated. Hynninen conducted a study of 41 patients undergoing preoperative PET/CT followed by diagnostic high dose contrast-enhanced CT scan. They observed that PET/CT was not superior to CT for the detection of intra-abdominal disease spread, but was more effective in identifying extra-abdominal metastases (Fig. 4) [98]. Fruscio et al. reviewed their experience with 95 patients in which more than a quarter were clinically upstaged from stage III to stage IV by PET/CT. However, women upstaged to IV had a similar prognosis as stage III patients, presumably because it was the intraperitoneal tumor load that was more likely to lead to death [99]. J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 601 Minimally invasive surgery Fig. 4. Stage IV high grade ovarian serous carcinoma. Axial fusion images from whole body FDG PET-CT exam shows a hypermetabolic right adnexal primary tumor (A) and retroperitoneal adenopathy (B). Chest portion of the exam (C) reveals unsuspected left supraclavicular adenopathy (arrow) that may impact primary treatment. While there is as yet no clear consensus on the criteria for resectable peritoneal lesions, radiologic imaging serves as an important roadmap for treatment planning. The American College of Radiology's Appropriateness Criteria consensus recommendations currently rate abdominal–pelvic CT as the modality of choice for pre-treatment evaluation of ovarian cancer patients [100]. Chest CT is also indicated should the chest radiograph prove abnormal. Accurate interpretation requires radiologist expertise in complex intra-abdominal anatomy, and clinical dialogue with a gynecologic oncologist having familiarity with specific disease sites that are likely to present particular difficulties with regard to surgical access and technique [101]. Although CT is at present the most predictive procedure, it is not in and of itself accurate enough to consistently guide clinical management. The inherent limitations in accurately correlating imaging findings for a disease with varying levels of intraperitoneal surface implant dissemination detected at surgery has led to evolving paradigms wherein preoperative laparoscopic evaluation of disease is used to help triage patients toward PDS or NAC. In theory, this approach would avoid unnecessarily morbid, suboptimal laparotomies that unduly lengthen the time of treatment and increase overall costs. Several prospective and retrospective studies have investigated the use of laparoscopy to predict the outcome of debulking surgery. In a pilot study of patients undergoing laparoscopy followed by standard laparotomy, Fagotti et al. observed that optimal debulking was achievable in 87% of cases selected as being completely resectable by explorative laparoscopy [102]. With this promising preliminary data, a laparoscopy-based quantitative predictive model (predictive index value [PIV]) was devised to provide an objective score of intraperitoneal disease spread (Table 5). The PIV has subsequently undergone initial testing and validation as a triage tool [103,104]. To minimize the chances of inappropriately failing to perform PDS, the best PIV cutoff was noted to be ≥8, corresponding to a positive predictive value of 100%, or a zero percent chance of complete resection among these investigators [105]. Fagotti et al. subsequently reported on 300 consecutive patients who underwent staging laparoscopy. Importantly, none had complications related to the procedure. Based on high tumor load (PIV ≥ 8), 152 (50.7%) went on to receive NAC and 57.5% had no residual disease at the time of interval debulking. Of the 148 who underwent PDS, 62.1% had complete resection. The authors concluded that this minimally invasive strategy may help to meaningfully individualize treatment, while avoiding unnecessary open surgery and its sequelae [106]. Vizzielli et al. also reported 348 consecutive advanced ovarian cancer patients who underwent preoperative laparoscopic evaluation. All study women received a PIV score and were stratified into three groups based on volume of disease. In a multivariate analysis, tumor load stratified by PIV was found to be independently associated with overall survival, along with the amount of residual disease and performance status [107]. In a multicenter trial (Olympia-MITO 13) to prospectively evaluate the accuracy and reproducibility of staging laparoscopy at different satellite centers, 168 patients underwent PIV scoring. Following a short intensive training period, the technique was shown to be an accurate and reliable assessment of intraperitoneal diffusion of disease in advanced ovarian cancer patients [108]. The LapOvCa-trial is a randomized multicenter trial including all gynecologic oncology centers in the Netherlands and their affiliated hospitals. The purpose of this ongoing study is to investigate whether laparoscopy is cost-effective in predicting which patients will benefit from PDS and which patients should be treated by NAC and interval surgery instead [109]. Whether the PIV score will be readily adaptable to gynecologic oncologists in the United States remains an open question. Nick et al. recently presented the triage algorithm modified from Fagotti that is currently under investigation at the MD Anderson Cancer Center. Of the 33 patients who underwent laparoscopy, none had an intraoperative complication, and 19 (58%) who had a PIV score b8 subsequently underwent PDS. By the use of this approach, their rate of achieving complete resection improved from a historical rate of 44% to 84% [110]. Table 5 Fagotti laparoscopic predictive index value (PIV) score. Omental cake Peritoneal/diaphragmatic carcinomatosis Mesenteric retraction Bowel/stomach infiltration Spleen/liver superficial metastasis Each positive evaluation receives a score of 2. 602 J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 However, more data is needed. In a Cochrane Database review of seven studies reporting on six cohorts, laparoscopy identified a broad range (27–64%) of patients with too extensive disease to warrant laparotomy and correspondingly between 36–73% having disease suitable for PDS. Laparoscopy is a promising tool with minimal complications, but the limited number of studies and unproven reproducibility at present do not allow firm conclusions to be drawn from this data as yet [111]. Ultra-radical surgery Extensive upper abdominal disease is often the limiting factor determining whether a patient with advanced ovarian cancer can be optimally debulked to no residual disease. While tumor in this location is strongly indicative of aggressive tumor biology, a surgeon's experience and willingness to employ ultra-radical procedures is correlated with success in achieving complete resection [112,113]. Not every gynecologic oncologist is comfortable routinely performing liver resection, splenectomy, or diaphragmatic resection, and complications may not be trivial. However, patients referred to specialized centers where such radical procedures are commonly performed may anticipate higher rates of optimal debulking and improved survival, without necessarily leading to increased major morbidity [114]. Several institutions incorporating ultra-radical techniques have reported survival rates to improve accordingly [36–38]. Although it is still unclear what impact ultra-radical techniques have on quality of life and morbidity, the limited available evidence suggests a measured improvement in survival [115]. One common theme for safely expanding the ability to completely resect advanced ovarian cancer is the willingness to incorporate a multidisciplinary surgical team, as needed, to facilitate debulking outside of the provider's typical comfort zone. In addition, having tertiary care resources to manage the wide variety of possible postoperative complications is critically important. Complex patients warrant treatment in a specialized center. Synopsis Current surgical management of ovarian cancer requires excellent clinical judgment and technical mastery of a wide array of procedures. Involvement of a gynecologic oncologist to oversee patient care has proven to improve outcomes. Complete resection of all macroscopic disease at PDS has been shown to be the single most important independent prognostic factor in advanced ovarian cancer. Therefore, when deciding on PDS there should be a reasonable chance of leaving no residual tumor or at least substantial cytoreduction to b1 cm at the time of surgery [46]. The ability to clinically gauge those most likely to be completely cytoreduced and thereby effectively triage patients toward PDS or NAC involves a complex interplay of numerous factors, including imaging findings, physical examination, existing medical co-morbidities, and the expertise of the surgical team. No single individual has the capacity to make the right call in every circumstance, and even if it were the case, it would not necessarily benefit patients outside of his/her purview. We advocate a team approach to interpret available information and allow the patient to make an informed decision toward initial therapy. To that end, a consistent preoperative treatment planning conference is ideal, with multi-disciplinary attendance, consistent imaging review and ongoing reassessment of outcome measures. In this way, co-existing factors Table 6 Patients who appear to benefit the most from primary debulking surgery: a proposal. Stage IIIA or IIIB disease Stage IIIC disease with Fagotti laparoscopic score b8 Stage IIIC disease with promising multidisciplinary imaging review at ‘expert’ center routinely able to incorporate ultra-radical procedures as appropriate Table 7 Patients who appear to benefit the most from neoadjuvant chemotherapy: a proposal. Stage IIIC disease that is too extensive to be optimally debulked based on imaging or laparoscopic scoring Stage IV disease (likelihood of complete resection b10%) Performance status too poor to undergo an attempt at surgical debulking No access to an experienced ovarian cancer surgical team The elderly or morbidly obese when ultra-radical procedures appear necessary such as elderly age, morbid obesity or stage IV disease extension can all be taken into account (Tables 6 and 7). Further modification of current imaging techniques is unlikely to substantially improve the triage of patients upfront. The promising work on laparoscopic scoring needs to be replicated in the United States with reassuring survival outcomes, otherwise it is unlikely to be widely incorporated. Ultimately, any and all of these preoperative methods to predict complete resection are still intimately tied to the surgeon's ability to translate them into a successful outcome. While several institutions have demonstrated improvement in rates of achieving optimal debulking by incorporation of ultra-radical techniques, it is difficult to conceive of pushing the surgical limits much beyond that. Future strategies Rather than refining subjective clinical assessments such as imaging or laparoscopy, it is likely that a reproducible genomics-based model will be necessary to effectively triage patients to initial therapy. Preliminary data on a signature that predicts the success of debulking has been proposed, but much additional work is needed before this becomes a reality [116]. It seems feasible, at least in theory, that molecular analysis of a percutaneous core biopsy might ultimately be the most cost-effective method for determining when or if a patient should go to surgery, and what type of targeted therapy is likely to be most efficacious. At a more basic level, just having access to subspecialty care continues to be a significant problem. It is an unfortunate reality that geographic proximity to a high-volume hospital and travel distance to receive treatment are independent predictors of guideline-adherent care for advanced ovarian cancer. Such barriers disproportionally affect racial minorities and women of low socio-economic status [117]. Networks that are able to successfully integrate ovarian cancer treatment across tertiary and community hospitals need to be promoted and expanded so that all women diagnosed can receive the same level of care. Management of advanced ovarian cancer consistently requires a complex, multidisciplinary team to achieve the best outcomes. Whenever feasible, patients should be encouraged to seek treatment at these expert centers. Whether you are a believer or a dissenter of PDS, we have very limited data to interpret. Only a randomized phase III trial of PDS versus NAC performed in the United States with impressive rates of optimal cytoreduction will be definitive. We should embrace this challenge of constructing a well-designed definitive study and vigorously support those, such as Dennis Chi, who are trying to find a way to fund such a trial. It is telling that without substantial pharmaceutical industry support of an agent or device, there is an impasse in conducting a trial to answer this basic question. Finally, since surgical paradigms have been shown to improve with sustained effort, more transparency per provider or per institution would be helpful in measuring where there are lessons to be learned or improvements to be incorporated. Hopefully, the newly launched SGO Clinical Outcomes Registry will provide this type of detailed data. In the meantime, the gynecologic oncology community is charged with identifying further evidence-based refinements in the approach to upfront treatment, continuing to train fellows in the range of procedures that may be required for primary or interval debulking surgery, and broadening the access to subspecialty care. J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 For the foreseeable future, most women will continue to be diagnosed with ovarian cancer after it has already spread extensively within the peritoneal cavity. The debate on efficacy of PDS versus NAC appears to be still in the early rounds. None of us should prematurely declare our side the winner, nor throw in the towel on this metaphorical boxing match, but instead work together to fight the common enemy. It is incumbent upon all of us to continue exploring ways to establish a structured, consistent, transparent approach to the best initial management of this disease. Hopefully, that is something that we can all believe in, without dissent. Conflict of interest statement The authors have no financial disclosures to report at this time. References [1] Menon U, Gentry-Maharaj A, Hallett R, Ryan A, Burnell M, Sharma A, et al. Sensitivity and specificity of multimodal and ultrasound screening for ovarian cancer, and stage distribution of detected cancers: results of the prevalence screen of the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS). Lancet Oncol 2009; 10:327–40. [2] Schorge JO, Modesitt SC, Coleman RL, Cohn DE, Kauff ND, Duska LR, et al. SGO White Paper on ovarian cancer: etiology, screening and surveillance. Gynecol Oncol 2010;119:7–17. [3] Buys SS, Partridge E, Black A, Johnson CC, Lamerato L, Isaacs C, et al. Effect of screening on ovarian cancer mortality: the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled Trial. JAMA 2011;305:2295–303. [4] Moyer VA. Screening for ovarian cancer: U.S. Preventive Services Task Force reaffirmation recommendation statement. Ann Intern Med 2012;157:900–4. [5] Vergote I, Trope CG, Amant F, et al. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N Engl J Med 2010;363:943–53. [6] Earle CC, Schrag D, Neville BA, Yabroff KR, Topor M, Fahey A, et al. Effect of surgeon specialty on processes of care and outcomes for ovarian cancer patients. J Natl Cancer Inst 2006;98:172–80. [7] Engelen MJ, Kos HE, Willemse PH, et al. Surgery by consultant gynecologic oncologists improves survival in patients with ovarian carcinoma. Cancer 2006;106: 589–98. [8] Carney ME, Lancaster JM, Ford C, et al. A population-based study of patterns of care for ovarian cancer: who is seen by a gynecologic oncologist and who is not? Gynecol Oncol 2002;84:36–42. [9] Meigs JV. Tumors of the female pelvic organs. New York: Macmillen; 1934. [10] Griffiths CT. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr 1975;42:101–4. [11] Griffiths CT, Parker LM, Fuller Jr AF. Role of cytoreductive surgical treatment in the management of advanced ovarian cancer. Cancer Treat Rep 1979;63:235–40. [12] Hacker NF, Berek JS, Lagasse LD, Nieberg RK, Elashoff RM. Primary cytoreductive surgery for epithelial ovarian cancer. Obstet Gynecol 1983;61:413–20. [13] Piver MS, Lele SB, Marchetti DL, et al. The impact of aggressive debulking surgery and cisplatin-based chemotherapy on progression-free survival in stage III and IV ovarian carcinoma. J Clin Oncol 1988;6:983–9. [14] Blackham AU, Russell GB, Stewart JH, Votanopoulos K, Levine EA, Shen P. Metastatic colorectal cancer: survival comparison of hepatic resection versus cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol 2014;21: 2667–74. [15] Heng DY, Wells JC, Rini BI, Beuselinck B, Lee JL, Knox JJ, et al. Cytoreductive nephrectomy in patients with synchronous metastases from renal cell carcinoma: results from the International Metastatic Renal Cell Carcinoma Database Consortium. Eur Urol 2014;66:704–10. [16] Rudloff U, Langan RC, Mullinax JE, Beane JD, Steinberg SM, Beresnev T, et al. Impact of maximal cytoreductive surgery plus regional heated intraperitoneal chemotherapy (HIPEC) on outcome of patients with peritoneal carcinomatosis of gastric origin: results of the GYMSSA trial. J Surg Oncol 2014;110:275–84. [17] Salti GI, Ailabouni L, Undevia S. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for the treatment of peritoneal sarcomatosis. Ann Surg Oncol 2012;19:1410–5. [18] Covens AL. A critique of surgical cytoreduction in advanced ovarian cancer. Gynecol Oncol 2000;78:269–74. [19] Napoletano C, Bellati F, Landi R, Pauselli S, Marchetti C, Visconti V, et al. Ovarian cancer cytoreduction induces changes in T cell population subsets reducing immunosuppression. J Cell Mol Med 2010;14:2748–59. [20] Curley MD, Garrett LA, Schorge JO, Foster R, Rueda BR. Evidence for cancer stem cells contributing to the pathogenesis of ovarian cancer. Front Biosci 2011;16: 368–92. [21] Dean M, Fojo T, Bates S. Tumour stem cells and drug resistance. Nat Rev Cancer 2005;5:275–84. [22] Goldie JH, Coldman AJ. A mathematic model for relating the drug sensitivity of tumors to their spontaneous mutation rate. Cancer Treat Rep 1979;63:1727–33. [23] Eisenhauer EL, Abu-Rustum NR, Sonoda Y, et al. The addition of extensive upper abdominal surgery to achieve optimal cytoreduction improves survival in patients with stages IIIC–IV epithelial ovarian cancer. Gynecol Oncol 2006;103:1083–90. 603 [24] Eisenkop SM, Spirtos NM, Friedman RL, et al. Relative influences of tumor volume before surgery and the cytoreductive outcome on survival for patients with advanced ovarian cancer: a prospective study. Gynecol Oncol 2003;90:390–6. [25] Hoskins WJ, Bundy BN, Thigpen JT, Omura GA. The influence of cytoreductive surgery on recurrence-free interval and survival in small-volume stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. Gynecol Oncol 1992;47: 159–66. [26] Hoskins WJ, McGuire WP, Brady MF, et al. The effect of diameter of largest residual disease on survival after primary cytoreductive surgery in patients with suboptimal residual epithelial ovarian carcinoma. Am J Obstet Gynecol 1994;170:974–9. [27] Whitney CW, Spirtos N. Gynecologic Oncology Group surgical procedures manual.. www.gog.org Philadelphia, PA: Gynecologic Oncology Group; 2010 [Ref Type: Electronic Citation]. [28] Armstrong DK, Bundy B, Wenzel L, et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006;354:34–43. [29] Chi DS, Ramirez PT, Teitcher JB, et al. Prospective study of the correlation between postoperative computed tomography scan and primary surgeon assessment in patients with advanced ovarian, tubal, and peritoneal carcinoma reported to have undergone primary surgical cytoreduction to residual disease 1 cm or less. J Clin Oncol 2007;25:4946–51. [30] Sala E, Mannelli L, Yamamoto K, Griffin M, Griffin N, Grant L, et al. The value of postoperative/preadjuvant chemotherapy computed tomography in the management of patients with ovarian cancer. Int J Gynecol Cancer 2011;21:296–301. [31] Winter III WE, Maxwell GL, Tian C, et al. Prognostic factors for stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. J Clin Oncol 2007;25:3621–7. [32] Chang SJ, Bristow RE. Evolution of surgical treatment paradigms for advancedstage ovarian cancer: redefining ‘optimal’ residual disease. Gynecol Oncol 2012; 125:483–92. [33] Aletti GD, Dowdy SC, Gostout BS, Jones MB, Stanhope CR, Wilson TO, et al. Aggressive surgical effort and improved survival in advanced-stage ovarian cancer. Obstet Gynecol 2006;107:77–85. [34] Chang SJ, Bristow RE, Ryu HS. Impact of complete cytoreduction leaving no gross residual disease associated with radical cytoreductive surgical procedures on survival in advanced ovarian cancer. Ann Surg Oncol 2012;19:4059–67. [35] Chi DS, Eisenhauer EL, Lang J, et al. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol Oncol 2006;103:559–64. [36] Aletti GD, Dowdy SC, Gostout BS, et al. Quality improvement in the surgical approach to advanced ovarian cancer: the Mayo Clinic experience. J Am Coll Surg 2009;208:614–20. [37] Chi DS, Eisenhauer EL, Zivanovic O, et al. Improved progression-free and overall survival in advanced ovarian cancer as a result of a change in surgical paradigm. Gynecol Oncol 2009;114:26–31. [38] Harter P, Muallem ZM, Buhrmann C, Lorenz D, Kaub C, Hils R, et al. Impact of a structured quality management program on surgical outcome in primary advanced ovarian cancer. Gynecol Oncol 2011;121:615–9. [39] Chang SJ, Hodeib M, Chang J, Bristow RE. Survival impact of complete cytoreduction to no gross residual disease for advanced-stage ovarian cancer: a meta-analysis. Gynecol Oncol 2013;130:493–8. [40] Rosen B, Laframboise S, Ferguson S, Dodge J, Bernardini M, Murphy J, et al. The impacts of neoadjuvant chemotherapy and of debulking surgery on survival from advanced ovarian cancer. Gynecol Oncol 2014;134:462–7. [41] Landrum LM, Java J, Mathews CA, Lanneau Jr GS, Copeland LJ, Armstrong DK, et al. Prognostic factors for stage III epithelial ovarian cancer treated with intraperitoneal chemotherapy: a Gynecologic Oncology Group study. Gynecol Oncol 2013;130:12–8. [42] Elattar A, Bryant A, Winter-Roach BA, Hatem M, Naik R. Optimal primary surgical treatment for advanced epithelial ovarian cancer. Cochrane Database Syst Rev 2011:CD007565. [43] Grabowski JP, Harter P, Hils R, Lorenz D, Kaub C, Barinoff J, et al. Outcome of immediate re-operation or interval debulking after chemotherapy at a gynecologic oncology center after initially incomplete cytoreduction of advanced ovarian cancer. Gynecol Oncol 2012;126:54–7. [44] Aletti GD, Santillan A, Eisenhauer EL, Hu J, Aletti G, Podratz KC, et al. A new frontier for quality of care in gynecologic oncology surgery: multi-institutional assessment of short-term outcomes for ovarian cancer using a risk-adjusted model. Gynecol Oncol 2007;107:99–106. [45] Stashwick C, Post MD, Arruda JS, Spillman MA, Behbakht K, Davidson SA, et al. Surgical risk score predicts suboptimal debulking or a major perioperative complication in patients with advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer. Int J Gynecol Cancer 2011;21:1422–7. [46] Vergote I, Du BA, Amant F, Heitz F, Leunen K, Harter P. Neoadjuvant chemotherapy in advanced ovarian cancer: on what do we agree and disagree? Gynecol Oncol 2013;128:6–11. [47] Fago-Olsen CL, Ottesen B, Kehlet H, Antonsen SL, Christensen IJ, Markauskas A, et al. Does neoadjuvant chemotherapy impair long-term survival for ovarian cancer patients? A nationwide Danish study. Gynecol Oncol 2014;132:292–8. [48] Lawton FG, Redman CW, Luesley DM, Chan KK, Blackledge G. Neoadjuvant (cytoreductive) chemotherapy combined with intervention debulking surgery in advanced, unresected epithelial ovarian cancer. Obstet Gynecol 1989;73:61–5. [49] Schwartz PE, Chambers JT, Makuch R. Neoadjuvant chemotherapy for advanced ovarian cancer. Gynecol Oncol 1994;53:33–7. [50] Vergote IB, De WI, Decloedt J, Tjalma W, Van GM, van DP. Neoadjuvant chemotherapy versus primary debulking surgery in advanced ovarian cancer. Semin Oncol 2000;27:31–6. [51] da C.M. V, de Souza Fede AB, Dos Anjos CH, da Silva JR, Sanchez FB, da Silva Bessa LR, et al. Neoadjuvant chemotherapy with six cycles of carboplatin and paclitaxel in 604 [52] [53] [54] [55] [56] [57] [58] [59] [60] [61] [62] [63] [64] [65] [66] [67] [68] [69] [70] [71] [72] [73] [74] [75] [76] [77] [78] J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 advanced ovarian cancer patients unsuitable for primary surgery: safety and effectiveness. Gynecol Oncol 2014;132:287–91. Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002;20:1248–59. van der Burg ME, van LM, Buyse M, et al. The effect of debulking surgery after induction chemotherapy on the prognosis in advanced epithelial ovarian cancer. Gynecological Cancer Cooperative Group of the European Organization for Research and Treatment of Cancer. N Engl J Med 1995;332:629–34. Rose PG, Nerenstone S, Brady MF, Clarke-Pearson D, Olt G, Rubin SC, et al. Secondary surgical cytoreduction for advanced ovarian carcinoma. N Engl J Med 2004;351: 2489–97. Tangjitgamol S, Manusirivithaya S, Laopaiboon M, Lumbiganon P, Bryant A. Interval debulking surgery for advanced epithelial ovarian cancer. Cochrane Database Syst Rev 2013;4:CD006014. Dewdney SB, Rimel BJ, Reinhart AJ, et al. The role of neoadjuvant chemotherapy in the management of patients with advanced stage ovarian cancer: survey results from members of the Society of Gynecologic Oncologists. Gynecol Oncol 2010; 119:18–21. Vergote I, Amant F, Leunen K. Neoadjuvant chemotherapy in advanced ovarian cancer: what kind of evidence is needed to convince US gynaecological oncologists? Gynecol Oncol 2010;119:1–2. Chi DS, Musa F, Dao F, Zivanovic O, Sonoda Y, Leitao MM, et al. An analysis of patients with bulky advanced stage ovarian, tubal, and peritoneal carcinoma treated with primary debulking surgery (PDS) during an identical time period as the randomized EORTC–NCIC trial of PDS vs neoadjuvant chemotherapy (NACT). Gynecol Oncol 2012;124:10–4. Vergote I, Leunen K, Amant F. Primary surgery or neoadjuvant chemotherapy in ovarian cancer: what is the value of comparing apples with oranges? Gynecol Oncol 2012;124:1–2. Kehoe S, Hook J, Nankivell M, et al. Chemotherapy or upfront surgery for newly diagnosed advanced ovarian cancer: results from the MRC CHORUS trial. ASCO; 6-1-2013 [Ref Type: Abstract]. Morrison J, Haldar K, Kehoe S, Lawrie TA. Chemotherapy versus surgery for initial treatment in advanced ovarian epithelial cancer. Cochrane Database Syst Rev 2012;8:CD005343. Hightower RD, Nguyen HN, Averette HE, Hoskins W, Harrison T, Steren A. National survey of ovarian carcinoma. IV: patterns of care and related survival for older patients. Cancer 1994;73:377–83. Uyar D, Frasure HE, Markman M, von Gruenigen VE. Treatment patterns by decade of life in elderly women (Nor =70 years of age) with ovarian cancer. Gynecol Oncol 2005;98:403–8. Langstraat C, Aletti GD, Cliby WA. Morbidity, mortality and overall survival in elderly women undergoing primary surgical debulking for ovarian cancer: a delicate balance requiring individualization. Gynecol Oncol 2011;123:187–91. Glasgow MA, Yu H, Rutherford TJ, Azodi M, Silasi DA, Santin AD, et al. Neoadjuvant chemotherapy (NACT) is an effective way of managing elderly women with advanced stage ovarian cancer (FIGO Stage IIIC and IV). J Surg Oncol 2013;107: 195–200. Worley Jr MJ, Guseh SH, Rauh-Hain JA, Williams KA, Muto MG, Feltmate CM, et al. Does neoadjuvant chemotherapy decrease the risk of hospital readmission following debulking surgery? Gynecol Oncol 2013;129:69–73. Thrall MM, Goff BA, Symons RG, Flum DR, Gray HJ. Thirty-day mortality after primary cytoreductive surgery for advanced ovarian cancer in the elderly. Obstet Gynecol 2011;118:537–47. Wright JD, Ananth CV, Tsui J, Glied SA, Burke WM, Lu YS, et al. Comparative effectiveness of upfront treatment strategies in elderly women with ovarian cancer. Cancer 2014;120:1246–54. Wright JD, Lewin SN, Deutsch I, Burke WM, Sun X, Neugut AI, et al. Defining the limits of radical cytoreductive surgery for ovarian cancer. Gynecol Oncol 2011; 123:467–73. Backes FJ, Nagel CI, Bussewitz E, Donner J, Hade E, Salani R. The impact of body weight on ovarian cancer outcomes. Int J Gynecol Cancer 2011;21:1601–5. Fotopoulou C, Richter R, Braicu EI, Kuhberg M, Feldheiser A, Schefold JC, et al. Impact of obesity on operative morbidity and clinical outcome in primary epithelial ovarian cancer after optimal primary tumor debulking. Ann Surg Oncol 2011;18: 2629–37. Kotsopoulos J, Moody JR, Fan I, Rosen B, Risch HA, McLaughlin JR, et al. Height, weight, BMI and ovarian cancer survival. Gynecol Oncol 2012;127:83–7. Protani MM, Nagle CM, Webb PM. Obesity and ovarian cancer survival: a systematic review and meta-analysis. Cancer Prev Res (Phila) 2012;5:901–10. Worley Jr MJ, Guseh SH, Rauh-Hain JA, Esselen KM, Muto MG, Feltmate CM, et al. What is the optimal treatment for obese patients with advanced ovarian carcinoma? Am J Obstet Gynecol 2014;211:231.e1–9. Kumar A, Bakkum-Gamez JN, Weaver AL, McGree ME, Cliby WA. Impact of obesity on surgical and oncologic outcomes in ovarian cancer. Gynecol Oncol 2014;135: 19–24. Pavelka JC, Brown RS, Karlan BY, Cass I, Leuchter RS, Lagasse LD, et al. Effect of obesity on survival in epithelial ovarian cancer. Cancer 2006;107:1520–4. Matthews KS, Straughn Jr JM, Kemper MK, Hoskins KE, Wang W, Rocconi RP. The effect of obesity on survival in patients with ovarian cancer. Gynecol Oncol 2009; 112:389–93. Wright JD, Tian C, Mutch DG, Herzog TJ, Nagao S, Fujiwara K, et al. Carboplatin dosing in obese women with ovarian cancer: a Gynecologic Oncology Group study. Gynecol Oncol 2008;109:353–8. [79] Au-Yeung G, Webb PM, DeFazio A, Fereday S, Bressel M, Mileshkin L. Impact of obesity on chemotherapy dosing for women with advanced stage serous ovarian cancer in the Australian Ovarian Cancer Study (AOCS). Gynecol Oncol 2014;133: 16–22. [80] Barrett SV, Paul J, Hay A, Vasey PA, Kaye SB, Glasspool RM. Does body mass index affect progression-free or overall survival in patients with ovarian cancer? Results from SCOTROC I trial. Ann Oncol 2008;19:898–902. [81] Howell EA, Egorova N, Hayes MP, Wisnivesky J, Franco R, Bickell N. Racial disparities in the treatment of advanced epithelial ovarian cancer. Obstet Gynecol 2013;122:1025–32. [82] Aletti GD, Dowdy SC, Podratz KC, Cliby WA. Analysis of factors impacting operability in stage IV ovarian cancer: rationale use of a triage system. Gynecol Oncol 2007; 105:84–9. [83] Bristow RE, Montz FJ, Lagasse LD, Leuchter RS, Karlan BY. Survival impact of surgical cytoreduction in stage IV epithelial ovarian cancer. Gynecol Oncol 1999;72: 278–87. [84] Rauh-Hain JA, Growdon WB, Rodriguez N, et al. Primary debulking surgery versus neoadjuvant chemotherapy in stage IV ovarian cancer. Gynecol Oncol 2011;120: S12–3. [85] Trope CG, Elstrand MB, Sandstad B, Davidson B, Oksefjell H. Neoadjuvant chemotherapy, interval debulking surgery or primary surgery in ovarian carcinoma FIGO stage IV? Eur J Cancer 2012;48:2146–54. [86] Winter III WE, Maxwell GL, Tian C, et al. Tumor residual after surgical cytoreduction in prediction of clinical outcome in stage IV epithelial ovarian cancer: a Gynecologic Oncology Group study. J Clin Oncol 2008;26:83–9. [87] van Meurs HS, Tajik P, Hof MH, Vergote I, Kenter GG, Mol BW, et al. Which patients benefit most from primary surgery or neoadjuvant chemotherapy in stage IIIC or IV ovarian cancer? An exploratory analysis of the European Organisation for Research and Treatment of Cancer 55971 randomised trial. Eur J Cancer 2013;49:3191–201. [88] Hou JY, Kelly MG, Yu H, et al. Neoadjuvant chemotherapy lessens surgical morbidity in advanced ovarian cancer and leads to improved survival in stage IV disease. Gynecol Oncol 2007;105:211–7. [89] Rafii A, Deval B, Geay JF, Chopin N, Paoletti X, Paraiso D, et al. Treatment of FIGO stage IV ovarian carcinoma: results of primary surgery or interval surgery after neoadjuvant chemotherapy: a retrospective study. Int J Gynecol Cancer 2007;17: 777–83. [90] Prat J. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int J Gynaecol Obstet 2014;124:1–5. [91] Bristow RE, Duska LR, Lambrou NC, Fishman EK, O'Neill MJ, Trimble EL, et al. A model for predicting surgical outcome in patients with advanced ovarian carcinoma using computed tomography. Cancer 2000;89:1532–40. [92] Dowdy SC, Mullany SA, Brandt KR, Huppert BJ, Cliby WA. The utility of computed tomography scans in predicting suboptimal cytoreductive surgery in women with advanced ovarian carcinoma. Cancer 2004;101:346–52. [93] Axtell AE, Lee MH, Bristow RE, Dowdy SC, Cliby WA, Raman S, et al. Multiinstitutional reciprocal validation study of computed tomography predictors of suboptimal primary cytoreduction in patients with advanced ovarian cancer. J Clin Oncol 2007;25:384–9. [94] Suidan RS, Ramirez PT, Sarasohn DM, Teitcher JB, Mironov S, Iyer RB, et al. A multicenter prospective trial evaluating the ability of preoperative computed tomography scan and serum CA-125 to predict suboptimal cytoreduction at primary debulking surgery for advanced ovarian, fallopian tube, and peritoneal cancer. Gynecol Oncol 2014;134:455–61. [95] Kitajima K, Murakami K, Yamasaki E, Kaji Y, Fukasawa I, Inaba N, et al. Diagnostic accuracy of integrated FDG-PET/contrast-enhanced CT in staging ovarian cancer: comparison with enhanced CT. Eur J Nucl Med Mol Imaging 2008;35:1912–20. [96] Pfannenberg C, Konigsrainer I, Aschoff P, Oksuz MO, Zieker D, Beckert S, et al. (18) F-FDG-PET/CT to select patients with peritoneal carcinomatosis for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol 2009; 16:1295–303. [97] Yoshida Y, Kurokawa T, Kawahara K, Tsuchida T, Okazawa H, Fujibayashi Y, et al. Incremental benefits of FDG positron emission tomography over CT alone for the preoperative staging of ovarian cancer. AJR Am J Roentgenol 2004;182:227–33. [98] Hynninen J, Kemppainen J, Lavonius M, Virtanen J, Matomaki J, Oksa S, et al. A prospective comparison of integrated FDG-PET/contrast-enhanced CT and contrastenhanced CT for pretreatment imaging of advanced epithelial ovarian cancer. Gynecol Oncol 2013;131:389–94. [99] Fruscio R, Sina F, Dolci C, Signorelli M, Crivellaro C, Dell'Anna T, et al. Preoperative 18F-FDG PET/CT in the management of advanced epithelial ovarian cancer. Gynecol Oncol 2013;131:689–93. [100] Mitchell DG, Javitt MC, Glanc P, Bennett GL, Brown DL, Dubinsky T, et al. ACR appropriateness criteria staging and follow-up of ovarian cancer. J Am Coll Radiol 2013; 10:822–7. [101] Nougaret S, Addley HC, Colombo PE, Fujii S, Al Sharif SS, Tirumani SH, et al. Ovarian carcinomatosis: how the radiologist can help plan the surgical approach. Radiographics 2012;32:1775–800. [102] Fagotti A, Fanfani F, Ludovisi M, Lo VR, Bifulco G, Testa AC, et al. Role of laparoscopy to assess the chance of optimal cytoreductive surgery in advanced ovarian cancer: a pilot study. Gynecol Oncol 2005;96:729–35. [103] Brun JL, Rouzier R, Uzan S, Darai E. External validation of a laparoscopic-based score to evaluate resectability of advanced ovarian cancers: clues for a simplified score. Gynecol Oncol 2008;110:354–9. [104] Fagotti A, Ferrandina G, Fanfani F, Ercoli A, Lorusso D, Rossi M, et al. A laparoscopybased score to predict surgical outcome in patients with advanced ovarian carcinoma: a pilot study. Ann Surg Oncol 2006;13:1156–61. J.O. Schorge et al. / Gynecologic Oncology 135 (2014) 595–605 [105] Fagotti A, Ferrandina G, Fanfani F, Garganese G, Vizzielli G, Carone V, et al. Prospective validation of a laparoscopic predictive model for optimal cytoreduction in advanced ovarian carcinoma. Am J Obstet Gynecol 2008;199:642–6. [106] Fagotti A, Vizzielli G, Fanfani F, Costantini B, Ferrandina G, Gallotta V, et al. Introduction of staging laparoscopy in the management of advanced epithelial ovarian, tubal and peritoneal cancer: impact on prognosis in a single institution experience. Gynecol Oncol 2013;131:341–6. [107] Vizzielli G, Costantini B, Tortorella L, Petrillo M, Fanfani F, Chiantera V, et al. Influence of intraperitoneal dissemination assessed by laparoscopy on prognosis of advanced ovarian cancer: an exploratory analysis of a single-institution experience. Ann Surg Oncol 2014;21:3170–7. [108] Fagotti A, Vizzielli G, De IP, Surico D, Buda A, Mandato VD, et al. A multicentric trial (Olympia-MITO 13) on the accuracy of laparoscopy to assess peritoneal spread in ovarian cancer. Am J Obstet Gynecol 2013;209:462. [109] Rutten MJ, Gaarenstroom KN, Van GT, van Meurs HS, Arts HJ, Bossuyt PM, et al. Laparoscopy to predict the result of primary cytoreductive surgery in advanced ovarian cancer patients (LapOvCa-trial): a multicentre randomized controlled study. BMC Cancer 2012;12:31. [110] Nick AM, Ramirez PT, Rangel KM, Schmeler KM, Soliman PT, Burzawa JK, et al. Launching personalized surgical therapy for advanced ovarian cancer. Gynecol Oncol 2014;133:28 [Supp 1]. [111] Rutten MJ, Leeflang MM, Kenter GG, Mol BW, Buist M. Laparoscopy for diagnosing resectability of disease in patients with advanced ovarian cancer. Cochrane Database Syst Rev 2014;2:CD009786. 605 [112] Aletti GD, Gostout BS, Podratz KC, Cliby WA. Ovarian cancer surgical resectability: relative impact of disease, patient status, and surgeon. Gynecol Oncol 2006;100: 33–7. [113] McCann CK, Growdon WB, Munro EG, et al. Prognostic significance of splenectomy as part of initial cytoreductive surgery in ovarian cancer. Ann Surg Oncol 2011;18: 2912–8. [114] Wimberger P, Lehmann N, Kimmig R, et al. Prognostic factors for complete debulking in advanced ovarian cancer and its impact on survival. An exploratory analysis of a prospectively randomized phase III study of the Arbeitsgemeinschaft Gynaekologische Onkologie Ovarian Cancer Study Group (AGO-OVAR). Gynecol Oncol 2007;106:69–74. [115] Ang C, Chan KK, Bryant A, Naik R, Dickinson HO. Ultra-radical (extensive) surgery versus standard surgery for the primary cytoreduction of advanced epithelial ovarian cancer. Cochrane Database Syst Rev 2011:CD007697. [116] Riester M, Wei W, Waldron L, Culhane AC, Trippa L, Oliva E, et al. Risk prediction for late-stage ovarian cancer by meta-analysis of 1525 patient samples. J Natl Cancer Inst 2014;106. [117] Bristow RE, Chang J, Ziogas A, Anton-Culver H, Vieira VM. Spatial analysis of adherence to treatment guidelines for advanced-stage ovarian cancer and the impact of race and socioeconomic status. Gynecol Oncol 2014;134:60–7.