Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Childhood immunizations in the United States wikipedia , lookup
Common cold wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Urinary tract infection wikipedia , lookup
Hepatitis C wikipedia , lookup
Gastroenteritis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Hepatitis B wikipedia , lookup
Neonatal infection wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Infection control wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
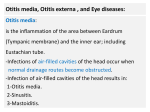
OTITIS EXTERNA Boucles D’Oreilles (The Earrings), Oil on canvas, William Adolphe Bouguereau 1891 At the first sign of otitis externa, the earrings must unfortunately come off! OTITIS EXTERNA Introduction External ear infection is a relatively common problem. It may be local (as in a furuncle) or it may be diffuse. More commonly the term otitis externa refers to a diffuse infection of the pinna and/ or external auditory meatus. The principle causes are bacterial infection, fungal infection or chronic dermatitis. Pathology Causes Inflammation of the external auditory canal and pinna may be due to infective causes or noninfective causes. Infective causes: 1. 2. Bacterial, including: ● Pseudomonas species (the majority of cases) ● Staphylococcus species ● Proteus species. Fungal causes: ● Aspergillus species (90% of cases) ● Phycomycetes ● Rhizopus species ● Actinomyces species ● Penicillium species ● Candida Non Infective Causes: 1. Eczema 2. Seborrhea 3. Contact dermatitis from earrings 4. Sensitivity to topical medications Predisposing Factors 1. Recurrent water exposure / swimming, (“swimmer’s ear”). 2. Jewelry, such as earrings. 3. Topical antibiotic use. 4. Hair dyes, (especially paraphenylenediamine) and other chemical compounds. 5. Traumatized external canal (particularly due to cotton-tipped swabs) 6. Skin conditions such as eczema may predispose to secondary bacterial infection. Complications Spread to adjacent cartilage is a significant complication. Acute otitis externa may spread to the pinna, resulting in a chondritis, particularly in diabetics or patients with newly pierced ears. Clinical Features Diagnosis is usually obvious on clinical grounds. Purulent otitis media with perforation of the tympanic membrane and drainage may occasionally masquerade as otitis externa. Before making a diagnosis of otitis externa exclude a perforated eardrum. Important points of History: 1. Irritation 2. Scanty discharge 3. Pain: 4. ● Moderate, occasionally severe if accompanied by frank cellulitis. ● Fungal infection tends not to cause as much pain as bacterial infections. Reduced hearing, (conduction loss) ● 5. If there is significant swelling of the ear canal. Predisposing factors: ● In particular check for a recent history of swimming or trauma. Important points of Examination: 1. Tenderness: ● 2. Periauricular adenitis: ● 3. Tenderness on gentle traction of the pinna or pressure on the tragus is a suggestive sign. This may occur, but it is not necessary for the diagnosis. Auroscopy: This can be very difficult, when there is significant pain 4. ● There is erythema and edema of the epithelium, ● Accumulation of moist debris in the canal. ● Spores and hyphae may be seen in the external canal, if the etiology is fungal. Check for predisposing skin conditions: ● Predisposing eczema of the pinna may be present. ● In the acute phases of allergic or dermatitic conditions, the skin is erythematous, edematous, and pruritic. Small, raised circumscribed lesions (papules), weeping fluid-filled lesions (vesicles), exudation, and crusting may be present. These lesions may become secondarily infected. An important differential diagnosis with respect to vesicular lesions, is shingles or Ramsay Hunt syndrome. ● 5. In chronic dermatitis phases, the skin may become thickened as a result of chronic rubbing or scratching. Thickening of the skin (lichenification), fissuring, and hyperpigmentation may be seen. Cellulitis: ● Frank cellulites will show the typical features of erythema, warmth and significant local tenderness. Investigations Otitis externa is a clinical diagnosis. Gram stain and culture of the canal discharge may be helpful, especially when a fungal cause is suspected. Viral swabs may be taken, if viral infection is suspected. Imaging and “septic workups” are only required when more serious invasive bacterial complications are suspected. Management Management consists of the following principles: 1. 2. Prevention of any causative/ aggravating factors. ● Remove jewelry, earrings. ● Avoidance of water contact with silicone ear plugs ● Avoidance of scratching / poking at the ears. ● Avoid aggravating soaps/ chemical General ear “toilette” This needs to be thorough and atraumatic. ● Gentle syringing with warm water to clear any debris. ● Gentle cleaning of debris with cotton wool buds. ● Ear wicks: In more severe cases, a Pope Otowick (Xomed) ear wick is very useful, (below): This is a semi-rigid foam wick, when inserted into the ear canal, swells and absorbs moisture as well as opening up the ear canal. Topical otic drops can be applied to it. The patient is reviewed on a daily basis to change the wick and continue the ear toilet. 3. Treatment directed to allergic or dermatitic conditions. ● 4. If the etiology is clearly allergic, then ceasing the offending agent and application of topical steroid is the treatment. Treatment directed toward specific infections: The clinical distinction between allergic, bacterial or a fungal cause is often difficult in the first instance. Preparations, which cover all these possibilities, are available. They generally contain a mix of neomycin, nystatin and triamcinolone drops. Most infective causes of otitis externa will be bacterial or fungal. Bacterial infection: ● Topical antibiotic drops, such as neomycin, framycetin or soframycin, are generally used. ● Oral antibiotics should be given if there is thought to be bacterial cellulitic involvement. Flucloxacillin or ciprofloxacin may be used. Fungal, (otomycosis): ● This is treated with ear toilet and topical antifungal agents. Viral: ● 5. Viral infection conventionally is not usually classified as otitis externa. It will more commonly be a form of localized shingles of the trigeminal nerve or Ramsay Hunt syndrome, a herpes infection of the seventh cranial nerve. Referral: ● Severe, or chronic cases, or those failing to respond to treatment, should be referred to an ENT specialist. References 1. Kumar S. ENT Emergencies in Cameron et al. Textbook of Adult Emergency Medicine, Churchill Livingston, 3rd ed 2008. Dr J. Hayes Reviewed November 2010