Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prediction of Early-Onset Esotropia From Components of
the Infantile Squint Syndrome
Clifton M. Schor* Robert E. Fusaro*^ Nance Wilson,-\% and Suzanne P. McKee%
Purpose. To examine the association between components of the infantile squint syndrome
(ISS) and age of onset of esotropia among subjects in the Cooperative Amblyopia Classification
Study (CACS).
Methods. Fifty subjects were classified retrospectively as having early-onset esotropia (EOE)
and 150 subjects were classified as having late-onset esotropia (LOE), depending on whether
symptoms of (or treatment for) strabismus occurred before the first birthday or between the
first and ninth birthdays, respectively. The authors compared the degree to which latent
nystagmus (LN), dissociated vertical deviation (DVD), monocular asymmetry of optokinetic
nystagmus (MOKN), monocular asymmetry of smooth pursuit (MSP), and perceived monocular speed bias (MSB) predicted EOE.
Results. Slow-phase velocity of MOKN and MSP were faster in response to nasal than to
temporal target motion. In contrast, MSB revealed that targets of equal velocity were perceived
as moving faster temporally than nasally. The authors evaluated MOKN, MSP, and MSB as
dichotomous and as continuous predictors. Dichotomous analysis showed significant associations between DVD and asymmetries of MOKN in the preferred eye of subjects with EOE.
Univariate logistic regression models, based on DVD and LN as well as on continuous measures
of MOKN, MSP, and MSB, revealed predictive power for all ISS components except LN. In
the preferred eye, MSP asymmetry was the strongest single predictor of EOE; multivariate
analysis revealed that prediction of EOE improved with the inclusion of DVD.
Conclusions. Multivariate analysis indicated that dichotomous measures of DVD and continuous
measures of MSP were independent predictors of EOE in a population of 8- to 40-year-old
subjects with strabismus. In the preferred eye, MOKN asymmetry was predictive of EOE in
the absence of information about MSP. Predictive values of all ISS components depended
heavily on the baseline prevalence of EOE in the target population. Invest Ophthalmol Vis
Sci. 1997;38:719-74O.
Infantile squint syndrome (ISS) is characterized by
several oculomotor anomalies associated with earlyonset esotropia (EOE), denned as esotropia that occurs during the first year of life.1"5 Historically, components of the syndrome have included latent nystagmus
(LN), dissociated vertical deviation (DVD), horizontal
monocular asymmetry of smooth pursuit (MSP), and
monocular asymmetry of optokinetic nystagmus
From the * School of Optometry and the \School of Public Health, University of
California at Berkeley, and from %The Smith-Kettlmvell Eye Research Institute, San
Francisco, California.
Supported by National Eye Institute grants EVO7657-05, EYO6883-09 SKEW, and
EYO3176-16 UCB.
Submitted for publication July 11, 1996; revised October 21, 1996; accepted October
22, 1996.
Proprietary interest category: N.
Reprint requests: Clifton M. Schor, School of Optometry, University of California at
Berkeley, 420 Minor Hall, Berkeley CA 94720-2020.
(MOKN) .3>6 8 The latter two conditions are characterized by reduced gain of smooth movements9"11 and
slow phase of MOKN6712"15 stimulated monocularly
by target motion in the temporal direction. Horizontal
asymmetry is most striking for MOKN when tested
with high retinal image velocities (>6°/second) and
is exaggerated for MSP when tested with low image
velocities (<5 o /second). 141617 Recently, it was suggested that a monocular asymmetry of horizontal motion perception, referred to here as monocular speed
bias (MSB), be included as a sensory component of
ISS whereby the same target velocity appears to move
at a higher speed in the nasal than in the temporal
direction.11 In several subjects with strabismus, the
perceived motion asymmetry was found to be most
pronounced at low retinal image velocities.11 Because
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
Copyright © Association for Research in Vision and Ophthalmology
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
719
720
Investigative Ophthalmology 8c Visual Science, March 1997, Vol. 38, No. 3
velocity discrimination provides feedback for MSP and
MOKN, it has been suggested that motion asymmetry
could be the basis of the horizontal motor asymmetries that characterize ISS.11
No comprehensive, population-based studies of
the ISS components have been reported. Studies of
large clinical populations of EOE have investigated
the prevalence of certain ISS components, such as
MOKN67'18'19 or DVD with LN.3'20"22 Several small studies have documented MSP asymmetries in subjects
with amblyopia, esotropia, or both.9"11'23"25 In addition, several small studies of motion sensitivity in subjects with strabismus, amblyopia, or both, yielded
mixed results concerning the presence of motion
asymmetries and their direction25"29; however, large
population-based studies of asymmetric MSP and
MSB, and the prevalence of these conditions in association with strabismus, have yet to be conducted.
Information about age of onset is useful in forming a prognosis for functional correction of strabismus
when it is associated with amblyopia in adults.30 Uncorrected amblyopia interferes with the binocular sensory
feedback necessary for maintaining binocular eye
alignment. Accordingly, the prognosis for functional
correction of strabismus in adults hinges on the prognosis for functional correction of amblyopia, which is
greater for binocular disorders of late onset than for
early onset. The association between EOE and various
components of the ISS can be used to estimate retrospectively the age of onset of esotropia when it is unknown.19
In this study, we investigated the degree to which
each of the five ISS components predicted EOE in
200 subjects with strabismus from the Cooperative Amblyopia Classification Study (CACS)31 using two data
analysis approaches. In the first analysis, we categorized continuous ISS measurements as normal or abnormal based on the 95th percentile of nonpreferred
eye measurements of a normal control group from
CACS (TO = 69). We estimated the positive and negative predictive values for EOE of each ISS component.
Although such dichotomous prediction rules are convenient, they may be inefficient and even misleading
given the crucial role of the diagnostic cutoff. Therefore, in the second analysis, we used logistic regression
to calculate MOKN, MSP, and MSB as continuous
measurements, without dichotomization, in univariate
and multivariate prediction models of EOE. Analysis
revealed that DVD, MSP, and MOKN were strong predictors of EOE. Predictive values of any ISS component ultimately depended on the prevalence of EOE
in the target population. Our results address the problem of forming a prognosis for functional correction
of strabismus in subjects with a history of amblyopia
who ranged in age from 8 to 40 years.
SUBJECTS AND METHODS
We evaluated the data base records of 200 subjects
with strabismus and 69 normal control subjects recruited for the CACS.31 We retrospectively classified
50 of the subjects with esotropia as having early-onset
esotropia and 150 subjects as having late-onset esotropia, depending on whether a history was reported of
symptoms of (or treatment for) strabismus during the
first year or between the first and ninth birthdays,
respectively. During childhood, the strabismus could
have been associated with amblyopia, as indicated by a
history of monocular patching therapy. In the current
clinical evaluation, amblyopia was defined as a bestcorrected acuity that was worse than or equal to 20/
40 in one eye. For 19 additional subjects with strabismus in the CACS data base, age of onset was indeterminable; hence, these subjects were not included in
our study. Ocular histories were obtained from medical records and from parents and subjects. Because
subjects were recruited primarily from public address
advertisements, age of onset was estimated from patient- and parent-reported histories. Ninety-six percent of the early-onset group, and 89% of late-onset
group, either had or had recovered from amblyopia
at the time of their participation in this study. Those
who recovered from amblyopia had a history of patching and a best-corrected visual acuity of better than
20/40 in both eyes. Anisometropia of at least 2 D was
observed in 26% of the early-onset group and in 42%
of the late-onset group. All 200 subjects with strabismus had undergone some form of treatment for strabismus and amblyopia (if present). Known treatments
included surgery in 101 subjects and patching in 173
subjects. Strabismus was classified as accommodative
if the horizontal angle of strabismus, as measured by
alternate cover test, was classified in a higher esotropia
or a lower exotropia category at the near rather than
at the far test distance. Generally, if the angle of strabismus increased at the near distance by one diagnostic category (the near angle of deviation was at least
3 base out prism diopters greater than the far angle
of deviation), the AC/A ratio was at least 7A/1 D. Age
of onset was determined during the clinical examination. Laboratory tests were conducted by a different
examiner who had no knowledge of the age of onset.
Subjects were informed fully about the nature of the
procedures, which were performed according to the
guidelines of the Declaration of Helsinki, and gave
their written consent before the beginning of the experiment.
Table 1 lists the prevalence of the various categories of strabismus present at the time of examination
in the CACS study for early- and late-onset groups.
Constant esotropia was more prevalent in EOE than
it was in LOE; corrected strabismus was more preva-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
Retrospective Prediction of Early-Onset Esotropia
721
l. Qualitative Characteristics of
Subjects With Strabismus in CACS Sample
of EOE and LOE
TABLE
Strabismus
Unilateral
Alternating
Intermittent
Constant
Accommodative
(high AC/A)
Esotropic
Exotropic
Orthotropic-recovered
Early Onset
Late Onset
(n = 50)
(n = 150)
82
12
6
74
72
10
10
54.7
14
64
30
6
16.6
46.7
34.7
18.7
CACS = Cooperative Amblyopia Classification Study; EOE =
early-onset esotropia; LOE = late-onset esotropia.
lent in LOE than it was in EOE. The other categories
(e.g., unilateral, alternating) had similar representation in the early- and late-onset groups. Other than
age of onset, characteristics of childhood strabismus
were unknown. We have assumed that in infancy the
strabismus was esotropic, even though some subjects
had exotropia during the examination. This assumption is based on the observation that esotropia is approximately five times more prevalent than exotropia
during the first decade of life32 and that after surgical
treatment, those with corrected esotropia may exhibit
exotropia.32'33 The mean (± SD) of ages at visit for
subjects classified as having EOE and LOE were 26.6
(±9.4) and 27.3 (±10.4) years, respectively.
Clinical Testing Procedure
All subjects enrolled in the study underwent clinical
examination of refractive error measured under dry
and cycloplegic conditions; visual acuity evaluated
with Bailey-Lovie LogMar test with the best optical
correction; horizontal and vertical angles of deviation
quantified with prism-cover test; DVD manifest by
cover test; latent nystagmus observed with cover test
and visuoscopy; and ocular health (assessment of the
optic disks and maculae). The presence of DVD and
strabismus were evaluated using standard criteria.33
During unilateral and alternating cover tests, each eye
was occluded for at least 5 seconds. Latent nystagmus
was diagnosed if a conjugate jerk nystagmus was present on covering either eye with the slow phase directed
toward the covered eye. Latent nystagmus was not diagnosed if a temporal drift of the unoccluded-fixating
eye was present on covering either eye. The preferred
eye of subjects with and without strabismus was defined using a monocular sighting task of a distant target viewed through a small aperture held near the
subject's face.
LABORATORY METHODS
All subjects underwent a series of oculomotor and
psychophysical tests to determine the functioning of
each eye. Only three of these tests are relevant for the
this article: the speed of the OKN response to drifting
sinusoidal gratings, the speed of smooth pursuit to a
moving target, and the speed discrimination for drifting sinusoidal gratings. Stimuli for all three tests were
displayed on a Princeton Max-15 monitor (Princeton
Graphic Systems, Princeton, NJ) (P-4 phosphor) with
screen dimensions of 19.7 X 25.5 cm. Mean luminance
for the displays was 90 cd/m 2 . Tests were made monocularly while the other eye was covered with an opaque
eye patch. Subjects wore their best optical corrections,
as determined by clinical examination preceding laboratory testing.
Eye movements for MOKN and MSP were measured with an Eye-Trac Model 210 Limbus Tracker
(Applied Science Laboratories, Waltham, MA). This
device consists of two infrared detectors for each eye
that respond to the amount of light reflected from
the limbal-scleral boundary; the difference in reflected light signaled by the detectors is converted into
degrees of eye rotation per volt. Before oculomotor
measurements were taken, the tracker was calibrated
for each eye by asking the patient to look at a large
flashing X presented first in the center of the monitor
and then 4.5° to the left or the right of center. Differential changes in voltage produced by the changes in
gaze were used to scale subsequent eye movements.
Monocular Asymmetry of Optokinetic
Nystagmus
The target for the MOKN measurements was a lowfrequency sinusoidal grating moving in one of two
directions (left or right) at 9.4°/second. The spatial
frequency of the grating was scaled with visual acuity;
for LogMar acuities better than 20/100 (Snellen
equivalent), the frequency was 1 cyc/deg; for acuities
between 20/100 and 20/600, the frequency was 0.5
cyc/deg, and for acuities poorer than 20/600, the frequency was 0.25 cyc/deg. Corresponding changes in
target temporal frequency were made to keep die
speed approximately constant at 9.4°/second for all
subjects. Stimulus duration was 15 seconds. Subjects
were instructed to look at the moving grating and to
allow their eyes to follow it. Viewing distance was 1
meter, at which the stimulus field subtended a visual
angle of 13°.
Eye position was sampled every 5 msec and stored
for further analysis. Raw data were smoothed by averaging with a moving window 11 samples wide (average
the 11 samples; assign the mean to the center of the
window; move the window by one sample; repeat the
procedure). Abrupt changes in position between
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
722
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
nearby samples that exceeded a threshold value (14°/
second for adjacent samples or 12°/second for samples three steps apart) were deemed saccades and were
removed from the record; these saccadic segments
were replaced with segments indicating no change of
eye position. Optokinetic nystagmus speeds were calculated from the desaccaded record by averaging with
a moving window 50 samples wide (250 msec). The
speeds for each 50-sample segment were sorted by
direction; speeds < 0.26°/second were discarded. The
mean speed for the accepted segments was calculated
for each direction.
Monocular Smooth Pursuit
The test stimulus for pursuit was a large moving X, 1°
in height for subjects with acuities better than 20/40
and 2° in height for subjects with acuities of 20/40 or
worse. The target moved left and right at 3.5°/second
for 40 seconds; traverse length was 7°. Subjects were
instructed to keep looking at the moving X. Viewing
distance was 1 m. Eye position was sampled every 5
msec and was stored on disk for subsequent analysis.
Pursuit data were analyzed using a procedure similar to the one used for analyzing OKN. The initial 250
msec of each record, corresponding to the latency and
acceleration phases of pursuit, was discarded. After
initial smoothing and desaccading, pursuit samples
were sorted by stimulus direction. As for OKN records,
pursuit speed was calculated by averaging with a moving window 50 samples wide; samples containing
speeds < 0.26°/second or >15°/second were discarded. Mean speed then was calculated from the accepted smoothed samples for each direction.
Speed Discrimination and Monocular
Speed Bias
The target for speed discrimination was a vertical sinusoidal grating of 1 cyc/deg drifting at a mean speed
of 3°/second. A small 1° fixation spot was superimposed on the screen to control fixation. The grating
was 11.2 cm high X 23.2 cm wide; viewing distance
was 0.67 m for all subjects. Target duration was varied
at random by 25% from trial-to-trial to obscure information about the distance moved by the bars because
the distance moved would necessarily covary with incremental changes in target speed. Duration was 800
msec ± 200 msec.
The speed increment threshold was estimated
from 100 two-alternative, forced-choice trials. Subjects
judged which of two stimulus presentations contained
the faster speed. The first presentation contained a
target moving at the reference speed (3°/second) always drifting toward the left. The second presentation
contained a target moving at the test speed, drifting
either left or right, with the direction chosen at random from trial to trial. The interstimulus interval was
500 msec. The test speed could be one of four values
chosen at random (one or two steps faster or one or
two steps slower than the reference speed). The step
size was varied adaptively, depending on the performance, within a 20-trial block. The minimum step was
5% of the reference, whereas the maximum step size
was 80%. If the patient's performance was so poor
that the step was increased to the maximum, only two
steps were presented, corresponding to the fastest and
the slowest test speeds (0.6°/second and 5.4°/second).
Responses were binned by the direction of the
second (test) interval. Separate biases and thresholds
were estimated from the psychometric functions for
each direction by probit analysis and from the whole
response set (both directions pooled). The bias, also
called the point of subjective equality, was estimated
as the stimulus value corresponding to the 50% point
on the cumulative normal function fitted by probit
analysis; threshold was defined as half the difference
between the stimulus values corresponding to the 25%
and 75% points on the fitted function (d' = 0.675).
For the MOKN and MSP analysis, the ratio of the
nasal speed to the sum of the nasal and temporal
speed (N/[N + T]) was considered. If OKN nasal
speed were faster than temporal speed, this ratio was
greater than 0.5. For the analysis of MSB in the speed
discrimination task, the ratio of the temporal speed
bias to the sum of the temporal and nasal biases (T/
[T + N]) was considered. If the patient perceived the
nasal speed as faster than the temporal speed, the ratio
was greater than 0.5. From a comparison of these two
ratios, we determined whether perceived speed was
related to either MOKN or MSP in individual subjects.
Data Analysis Methods. Two broad categories of
analyses were conducted on these data to evaluate the
usefulness of ISS components for predicting whether
the age of strabismus onset was early or late. The first,
more traditional approach evaluated ISS components
when considered as dichotomous predictors—i.e., diagnostic rules that predict EOE (or LOE) depending
on the presence (or absence) of an ISS abnormality.
Because the anomalies are either absent or present,
DVD and LN are inherently binary. Several of the ISS
(MOKN, MSP, MSB) are continuous and present a
spectrum of abnormalities. To evaluate them along
with DVD and LN in this dichotomous framework, the
continuous ISS measurements were dichotomized as
either normal or abnormal compared to diagnostic
cutoff points calculated from the 95th percentile of
measured responses of the nonpreferred eyes in a
group of 69 control subjects without strabismus. For
each ISS component, subjects with abnormal and normal ISS measurements were then cross-classified with
respect to EOE or LOE. This permitted calculation of
several measures of diagnostic usefulness described
below directly from the 2 X 2 tables within Table 2.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
Retrospective Prediction of Early-Onset Esotropia
723
TABLE 2.
Numbers of Subjects Classified With Normal and
Abnormal Characteristics of Infantile Squint Syndrome
Preferred
Nonpreferred
Preferred and
Nonpreferred
EOE
LOE
EOE
LOE
EOE
LOE
9
30
9
30
9
30
Normal
41
120
41
120
41
120
DVD
12
5
12
5
12
5
Normal
38
145
38
145
38
145
MOKN bias
24
26
21
36
15
14
No bias
26
124
29
114
35
136
MSP bias
32
49
28
54
25
26
No bias
18
101
22
96
25
124
MSB bias
13
23
19
35
6
3
No bias
37
127
31
115
44
147
LN
EOE = early-onset esotropia; LOE = late-onset esotropia; LN = late nystagmus; DVD = dissociated
vertical deviation; MOKN = monocular optokinetic nystagmus; MSP = monocular smooth pursuit;
MSB = monocular speed bias.
Dichotomous predictors often are evaluated in
terms of their sensitivity and specificity. For the purposes of our study, the sensitivity of an ISS component
is the probability that a person with EOE will exhibit
an abnormal value of the component in question.
Specificity is the probability that a person with LOE
will exhibit a normal value for the component. For
example, the sensitivity of DVD is defined as the probability that a subject with EOE displays DVD. The sensitivity of DVD can be estimated as the proportion of
subjects with strabismus in our sample with EOE who
have DVD (12 of 50). Similarly, the specificity of DVD
is defined as the probability that a subject with LOE
does not have DVD, which can be estimated by the
proportion of CACS subjects with LOE who do not
have DVD (145 of 150). High sensitivity implies low
false-negative rates; high specificity implies low falsepositive rates.
Although they are useful in many respects, sensitivity and specificity do not address directly the follow-
ing clinical concern: What is the probability that a
subject with (or without) an ISS anomaly in fact has
EOE (or LOE)? This aspect of a diagnostic test's performance is embodied in its positive and negative predictive values (± PV). Positive predictive value is the
probability of EOE based on the presence of an abnormal ISS measurement; negative predictive value represents the probability of LOE (not EOE) based on the
presence of a normal ISS measurement. The +PV of
DVD is defined as the probability of EOE given DVD;
the —PV is defined as the probability of LOE given
no DVD. The prevalence of EOE in CACS, without
regard to ISS measurements (the marginal, or what
we call the "baseline," prevalence), is simply the proportion of subjects with strabismus with EOE (0.25).
Although ±PVs are of substantial clinical interest, they
depend explicitly on the baseline prevalence as well
as on the sensitivity and specificity of the test in question (see Appendix A).
The dichotomous analyses are limited in several
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
724
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
MSP
MSB
Preferred Eye
Preferred Eye
Preferred Eye
0.6
—
B f a
0.2
0.4
IV1SB
0.8
1.0
MOKN
EOE LOE Norm
EOE LOE Norm
Non-Pref. Eye
Non-Pref. Eye
Non-Pref. Eye
1.0
EOE LOE Norm
0.8
•—i
0.6
CO
in
Q_
!
en
! II ^
cjj
0.2
0.4
i.
EOE LOE Norm
EOE LOE Norm
EOE LOE Norm
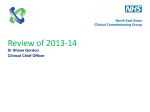
FIGURE l. Box plots illustrate the distributions of the bias ratios in the preferred and nonpreferred eyes for monocular optokinetic nystagmus, monocular smooth pursuit, and monocular speed bias for the early-onset, late-onset, and normal control groups. Lower, middle,
and upper lines of each shaded box represent the 25th, 50th, and 75th percentiles, respectively. Vertical lines extend to the most distant observation within 1.5 times the interquartile
range; outliers are represented by isolated dashes beyond these "whiskers."
important respects. First, although dichotomous tests
are clinically convenient, they may discard useful information because all "abnormal" values are considered to pose the same risk. In addition, it is difficult
to evaluate the usefulness of multiple ISS components,
e.g., DVD and MSP, using the dichotomous approach.
Therefore, we also fit logistic regression models to
the CACS data using standard maximum likelihood
techniques. We represented the continuous ISS components using piecewise linear splines. The logistic
regression parameter estimates enable us to estimate
the probability of EOE for a specific value of the continuous ISS component (for a given baseline prevalence of EOE). We selected among models by comparing their prediction errors estimated using a computer-intensive resampling technique called cross-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
725
Retrospective Prediction of Early-Onset Esotropia
For all five components, sensitivity and specificity
validation. Although we speak of "prediction"
were estimated (Table 3). Dissociated vertical deviathroughout this article, strictly speaking, the goal is to
tion displayed high specificity (0.97) but relatively low
ascertain correctly the subject's age of onset of esotropia as early or late using subsequent measurements of sensitivity (0.24). Monocular optokinetic nystagmus in
the preferred eye displayed relatively high specificity
the ISS components.
(0.83) and moderate sensitivity (0.48).
Dichotomous analysis focused on the positive and
RESULTS
the negative predictive values for all five ISS components, which are displayed, along with 95% confidence
Dichotomous Analysis: Positive and Negative
intervals,
in Figures 2A (preferred eyes) and 2B (nonPredictive Value
preferred
eyes). The confidence intervals for the ±PV
The box-and-whisker plots in Figure 1 show the distriestimates
in
Figures 2 and 3 are computed as ±2 times
butions of the MOKN, MSP, and MSB ratios of the
the
standard
errors of these estimates. In Figure 2, the
preferred and nonpreferred eyes for the early onset,
±PV for populations with the EOE prevalence of 0.25
late onset, and normal control groups. The lower,
observed
in CACS and, consequently, the standard
middle, and upper lines of each shaded box represent
errors,
are
estimated directly from Table 2 using stanthe 25th, 50th, and 75th percentiles, respectively; the
dard
methods
for proportions. In Figure 3, however,
vertical lines extend out from the box to the most
the
±PVs
(for
populations with other EOE prevadistant observation within 1.5 times the interquartile
lences) are estimated using the nonlinear functions
range; outliers are represented by isolated dashes beof sensitivity and specificity in Appendix A; hence, we
yond these "whiskers."
derived
the standard errors for ±PVs using the delta
Diagnostic cutoffs for abnormal nasal-temporal ramethod,
which relies on a Taylor series approximatios of MOKN, MSP, and MSB, set at the 95th percention.34 As shown in Appendix A, several factors detertiles of measurements of the nonpreferred eyes of the
mine the ±PV of a given ISS component, including
normal control group (n = 69), were 0.636, 0.559,
baseline prevalence of EOE in a given target populaand 0.458, respectively. The number of subjects with
tion and sensitivity and specificity of the test, which
EOE and LOE with normal and abnormal values of
are determined in part by the diagnostic cutoff criteria
thefiveISS components are shown in the 2X2 continadopted for dichotomous classification of an abnorgency tables within Table 2. These data were used to
mal response. To be a valuable predictor of EOE, a
compute prevalences, sensitivity, specificity, positive
given ISS component must have a predictive value
predictive values, and negative predictive values of the
greater than the baseline prevalence of EOE in a given
ISS components. Inspection of Table 2 shows that all
clinical population. The baseline prevalence of EOE
the ISS components, with the exception of LN, were
in our population was 50 of 200 subjects, or 0.25.
more prevalent in EOE than in LOE. The prevalence
Conversely, the baseline prevalence of LOE was 150
of DVD and the asymmetries of MOKN, MSP, and
of 200 subjects, or 0.75. Horizontal lines in Figure 2
MSB in preferred and nonpreferred eyes were higher
indicate the baseline prevalence of EOE (0.25) and
in the early group than in the late-onset group. Latent
LOE (0.75) in our sample for the + and —PV plots,
nystagmus was equally prevalent in the two groups,
respectively. Positive predictive values for DVD (0.71)
(0.18 versus 0.20). The greatest difference in prevaand for MOKN (0.48) in the preferred eye were sublence between early- and late-onset groups was for
stantially greater than the baseline prevalence of EOE
DVD (0.24 versus 0.03), but its overall prevalence in
(0.25). Although the estimated +PVs for several of
both groups was low.
3. Estimates of Sensitivity and Specificity for Components of
ISS in EOE and LOE
TABLE
Preferred Eye
Nonpreferred Eye
Both Eyes
ISS Components
Sensitivity
Specificity
Sensitivity
Specificity
Sensitivity
Specificity
DVD
LN
MOKN
MSP
MSB
0.24
0.18
0.48
0.64
0.26
0.97
0.80
0.83
0.67
0.85
0.24
0.18
0.42
0.56
0.38
0.97
0.80
0.75
0.64
0.77
0.24
0.18
0.30
0.50
0.12
0.97
0.80
0.91
0.83
0.98
ISS = infantile squint syndrome; EOE = early-onset esotropia; LOE = late-onset esotropia; LN =
latent nystagmus; DVD = dissociated vertical deviation; MOKN = monocular optokinetic nystagmus;
MSP = monocular smooth pursuit; MSB = monocular speed bias.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
726
+ PV
DVD
DVD
LN MOKN MSP MSB
-PV
DVD
LN MOKN MSP MSB
Preferred Eye
Preferred Eye
+ PV
-PV
rm
LN MOKN MSP MSB
Non-Preferred Eye
DVD
LN MOKN MSP MSB
Non-Preferred Eye
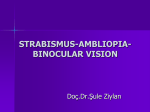
FIGURE 2. Bar graphs show the probability a subject had early-onset esotropia (+PV) or lateonset esotropia (—PV), depending on whether the subject displayed an abnormal or normal
infantile squint syndrome measure, respectively. These estimates assume that the prevalence
of early-onset esotropia was 0.25. (thin, dark vertical bars) 95% pointwise confidence intervals.
(horizontal lines) Baseline prevalence of early-onset esotropia and late-onset esotropia.
the other components were statistically significantly
different from the baseline prevalence of 0.25, none
appeared substantial enough to suggest clinical usefulness. The —PVs for all ISS components were close
to 0.75, suggesting that, in a population with an EOE
prevalence of 0.25, a normal value for an ISS component provides relatively little added information.
Generally, positive PVs of MOKN and MSP were
higher for preferred than for nonpreferred eyes. Abnormalities of both ISS components were more prevalent in preferred than in nonpreferred eyes of the
EOE group (see Table 2), leading to elevated +PV
and -PV. The greater prevalence of abnormal ratios
of MOKN and MSP in EOE for preferred than for
nonpreferred eyes probably resulted from more degraded MOKN and MSP in both the nasal and the
temporal directions in nonpreferred eyes. Abnormal
values for nasal and temporal OKN and smooth pursuit responses were set by the 95th percentiles of the
measurements of the nonpreferred eyes of the normal
control group. Among the EOE group, MOKN slowphase velocities were abnormally low in nasal and temporal directions in the nonpreferred eyes of eight subjects and in the preferred eyes of only two subjects.
Similarly, among the EOE group, MSP velocities were
abnormally low in both directions in the nonpreferred
eyes of three subjects and none of the preferred eyes.
The same trend occurred in the LOE group, in which
MOKN was reduced in both directions in the nonpreferred eyes of 16 subjects and in the preferred eyes of
eight subjects; MSP was reduced in both directions in
the nonpreferred eyes of 11 subjects and the preferred
eyes of seven subjects. Large and nearly equal abnormal responses in the two directions resulted in ratios
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
Retrospective Prediction of Early-Onset Esotropia
DVD
0.2
0.4
0.6
727
0.8
0.2
0.4
0.6
MSB
MSP
MOKN
0.2
0.8
0.4
0.6
0.2
0.8
0.4
0.6
0.8
EOE Prevalence
EOE Prevalence
EOE Prevalence
EOE Prevalence
DVD
MOKN
MSP
MSB
>
>
CL
3 •
0.2
0.4
0.6
0.8
EOE Prevalence
0.2
0.4
0.6
0.8
EOE Prevalence
0.2
0.4
0.6
0.8
EOE Prevalence
0.2
0.4
0.6
0.8
EOE Prevalence
FIGURE 3.
Plot-estimated positive {top) and negative {bottom) predictive values of the preferred
eyes for biases of dissociated vertical deviation, monocular optokinetic nystagmus, monocular
smooth pursuit, and monocular speed bias as a function of baseline prevalence of earlyonset esotropia. B and D in the monocular optokinetic nystagmus graphs represent measures
of +PV and —PV from Bourron-Madignier18 and Demer and von Noorden.19
that fell below the diagnostic cutoff, whereas greater
loss in the temporal direction resulted in larger ratios
that failed the diagnostic cutoff. If the bidirectional
anomalies are included in the group of subjects with
abnormal ratios, the motor anomalies either are
equally prevalent in the two eyes or are more prevalent
in the nonpreferred eye.
Positive and negative PVs depend explicitly on the
baseline prevalence of the disease in question (see
Appendix A). Consequently, the +PV and —PV for
any of the ISS components estimated from the CACS
data base are not universally applicable. For example,
the values of +PV shown in Figure 2 are specific to
the baseline prevalence of our clinical population. If
the baseline prevalence of EOE were greater than in
the CACS study, the +PV for the ISS component
would be higher and the —PV would be lower, as illustrated by Figure 3.
Figure 3 plots the estimated +PV and — PV in the
preferred eyes for measures of DVD, MOKN, MSP,
and MSB as a function of baseline prevalence of EOE.
The diagonal dashed lines in the upper set of figures
represent the EOE baseline prevalence for various hypothetical populations with strabismus; the dashed
lines in the lower figures represent the complementary prevalences of LOE in the same populations. The
curved functions describes the corresponding ±PV of
individual ISS components surrounded by the 95%
pointwise confidence intervals. Figure 3 shows that
DVD is a useful predictor of EOE over a large range
of baseline prevalence values. An abnormal MOKN
measurement is moderately informative. The —PV
plots suggest that normal ISS measurements appear
to provide little predictive information beyond that
provided by the baseline prevalence of EOE.
The estimates of +PV, based on asymmetric
MOKN in the current study sample, were compared
with the empirical results of two other studies of
asymmetric MOKN prevalence in early- and lateonset esotropia. 1819 Figure 3 plots the +PV and
—PV for MOKN reported by Bourron-Madignier
et al18 and Demer and von Noorden19 against the
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
728
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
c
CD
•*
CO o
0.0
0.2
0.4
0.6
0.8
1.0
Specificity
FIGURE 4. Sensitivity and specificity of monocular optokinetic nystagmus in the preferred eye are plotted for diagnostic cutoffs ranging from 0.5 to 1.0 in the Cooperative Amblyopia Classification Study data base. Values are compared
with the performance reported by (B) Bourron-Madignier18 and (D) Demer and von Noorden.19 The cutoff used
in Tables 2 and 3 and in Figures 2 and 3 was 0.64. As expected, as the cutoff criterion was altered from 0.5 to 1.0,
the sensitivity of the test decreased (fewer subjects with earlyonset esotropia were diagnosed with abnormal monocular
optokinetic nystagmus, and false-negative results increase),
whereas the specificity increased (more subjects with lateonset esotropia were diagnosed with normal monocular optokinetic nystagmus, and false-positive results decreased).
baseline prevalence for EOE and LOE reported in
their samples. Although our +PV estimate agrees
with Bourron-Madignier's for a population at
their baseline prevalence for EOE (0.54), our —PV
is substantially smaller. Our — PV estimate agrees
with Demer and von Noorden at their baseline
prevalence for EOE (0.58); however, our +PV is
substantially less. Therefore, discrepancies between our predictive value estimates cannot be explained entirely by the different baseline prevalences of EOE in the three study samples.
A possible factor that could contribute to residual differences in predictive values shown in Figure
3 is that the three studies may have used different
diagnostic cutoff criteria for categorizing MOKN
biases as abnormal. For example, a more stringent
or a higher diagnostic cutoff criterion for asymmetric MOKN might increase the +PV of MOKN. The
effect of the cutoff can be evaluated independently
of baseline prevalence by comparing sensitivity and
specificity of MOKN in the three studies. Different
cutoffs will define diagnostic tests of different sensi-
tivities and specificities that are independent of
baseline prevalence. Because the cutoffs in the
other two studies are unknown, we tested this hypothesis by reanalyzing our data using cutoffs ranging from 0.5 to 1.0 for categorizing MOKN biases
as abnormal (as shown in Fig. 4). We found that the
sensitivities and specificities reported by BourronMadignier et al18 and Demer and von Noorden19
lay substantially off our performance curve. This
discrepancy suggests that differences in sensitivity
and specificity (and, consequently, the differences
in +PV and —PV after accounting for baseline prevalence) are not simply the result of differences in
diagnostic criteria. As will be presented in the Discussion, factors such as MOKN stimulus parameters
may account for the differences in results.
Although several factors accounted for the discrepancies between +PV and —PV reported in
these three studies, a major factor was probably
the baseline prevalence of EOE. Demer and von
Noorden19 reported a +PV for MOKN (0.91) that
was nearly twice our estimate of +PV for the preferred eye (0.48). Differences in baseline prevalence for EOE (0.40) accounted for most of the
difference in +PV observed between these three
studies. Clearly, it is unwise to apply the ±PV values
from any of these studies to other clinical populations without first considering differences in baseline prevalence of EOE.
Logistic Regression Analysis of the Association
Between Infantile Squint Syndrome
Components and Early-Onset Esotropia
In this section, the predictive usefulness of the ISS components was assessed using the more powerful tool of logistic
regression. Biomedical researchers have used logistic regression models extensively to represent the association
between binary outcomes (e.g., early versus late onset
of esotropia) and various "predictor" or "explanatory"
variables (e.g., MOKN, MSP, MSB).35 The 2 X 2 contingency table analyses of die previous section, though simple to perform and interpret, required dichotomization
of the continuous ISS measurements. As cutoffs, we chose
the upper 95th percentiles of normal CACS subjects' measurements. Although this choice of cutoff is reasonable,
it is not necessarily optimal. Moreover, reducing the continuous measurement to a dichotomous variable, even
using an optimal cutoff, is likely to discard prognostic
information. The forgoing dichotomous analysis treats
all ISS measures above the diagnostic cutoff as equally
predictive of EOE. However, it is likely that MOKN asymmetries, which are extremely biased, are associated more
strongly with EOE than with smaller asymmetries, even
though both may fail the diagnostic cutoff. Thus, in this
section, logistic regression uses the continuous ISS mea-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
Retrospective Prediction of Early-Onset Esotropia
TABLE 4.
729
Univariate Logistic Regression Estimates
Parameter Estimates
a
ISS Component
Dichotomous Predictors
DVD
Latent nystagmus
Continuous Predictors
MOKN
Preferred
Nonpreferred
MSB
Preferred
Nonpreferred
MSP
Preferred
Nonpreferred
b
Estimate
Standard Error
Estimate
Standard Error
-1.3391
-1.0739
0.1818
0.1808
2.2146
-0.1300
0.5624
0.4205
-1.9241
-1.5787
0.2659
0.2401
0.8202
0.4286
0.1800
0.1432
-1.4794
-1.4214
0.2155
0.2122
1.5395
0.8711
0.5202
0.3378
-2.1068
-1.5229
0.2728
0.2282
1.2944
0.4985
0.2506
0.1695
ISS = infantile squint syndrome; DVD = dissociated vertical deviation; MOKN = monocular
optokinetic nystagmus; MSB = monocular speed bias; MSP = monocular smooth pursuit.
surements more efficiently to predict whether the onset
of esotropia was early or late.
Logistic regression provides additional data analysis
advantages over the dichotomous approach. It allows its
to estimate die probability that a subject had EOE based
on ISS measurements (and not simply to categorize die
subject widi either EOE or LOE, as in the dichotomous
analysis). This provides more refined information concerning the prognosis for a functional correction of
anomalies associated with strabismus, such as amblyopia,
and it can help clinicians formulate appropriate treatment strategies when they are considered in conjunction
with other clinical factors, including the motivation of
5. Prediction Error Estimates for
Univariate Logistic Regression Models
TABLE
Estimated Prediction Error*
ISS Component
Dichotomous Predictors
DVD
Continuous Predictors
MOKN
Preferred
Nonpreferred
MSB
Preferred
Nonpreferred
MSP
Preferred
Nonpreferred
Total
Negative
Positive
0.1728
0.5077
0.0612
0.1689
0.1733
0.4777
0.5302
0.0659
0.0543
0.1814
0.1871
0.5355
0.5483
0.0544
0.0667
0.1552
0.1827
0.4449
0.5317
0.0587
0.0664
=1= Baseline prediction errors: 0.1875, 0.5625, and 0.0625.
ISS = infantile squint syndrome; DVD = dissociated vertical
deviation; MOKN = monocular optokinetic nystagmus; MSB =
monocular speed bias; MSP = monocular smooth pursuit.
the patient and the clinician. Finally, logistic regression
facilitates a multivariate analysis, enabling us to consider
simultaneously the association of several ISS dichotomous
and continuous components with EOE.
Univariate Logistic Regression Models. If D is an indicator function of a binary outcome, die general form
of a logistic regression model for die probability of
the outcome given a single predictor, X, is as follows:
Pr[D=l\X=x]=
1 + exp(a + bx)
U)
In our case, D = 1 if the subject had EOE, and D
= 0 if the subject had LOE. The ISS predictor under
consideration is represented by A' (and its observed
value by x). The parameters, a and b, are estimated
by fitting such models to data from the CACS subjects,
(D,x), using standard maximum likelihood techniques. 35 This model is easily generalized to accommodate multivariate predictors by viewing X as a matrix
and b as a vector of parameters. Table 4 presents the a
and b parameter esdmates for eight univariate logistic
regression models, each using one of the ISS components to predict EOE.
Conditional Probability Interpretation of the Logistic
Model Parameters. The b parameter in equation 1
readily translates into a measure of association known
as the odds ratio. The odds ratio is used commonly in
epidemiology, in part because its interpretation does
not depend on the prevalence of the disease in question; in fact, the odds ratio can be estimated from
case-control studies in which the proportion of cases
is fixed by design. Although odds ratio estimates have
provided epidemiologists with considerable insight
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
730
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
TABLE
6. Multivariate Logistic Regression Estimates
Parameter Estimates and Standard Errors
Model 1
ISS Component
Est
SE
Est
SE
Est
Model 4
SE
Est
SE
1.2944
0.2506
1.1365
1.4313
0.2604
0.6273
0.8905
1.3865
0.3520
0.3079
0.6297
0.2345
0.8984
1.3940
0.3607
-0.0933
0.3134
0.6314
0.2434
0.7041
-2.1068
0.7278
-2.1269
0.2769
-2.2774
0.3026
-2.2720
0.3051
MSP
DVD
MOKN
MSB
Intercept
Model 3
Model 2
—2 log likelihood
191.113
185.753
183.534
183.517
ISS = infantile squint syndrome; MSP = monocular smooth pursuit; DVD = dissociated vertical deviation; MOKN = monocular
optokinetic nystagmus; MSB = monocular speed bias; Est = estimates; SE = standard errors.
into etiology, they are less immediately useful in clinical decision making, where a typical central question
can be: Given that an adult with strabismus shows a
particular ISS component of measurement x, what is
the probability that the subject had EOE? Equation 1
provides a way to model this conditional probability.
Thus, we will use the parameter estimates to "predict"
EOE status (D) based on these ISS measurements: By
substituting the maximum likelihood estimates from
Table 4 into equation 1, we obtain a maximum likelihood estimate for the conditional probability of EOE
(assuming that the prevalence of EOE is 0.25).
Univariate logistic regression provides no advantage over the contingency table-based methods for
predictor variables that are inherently dichotomous,
such as DVD or LN. Plugging the estimates of a and
b for DVD or LN into equation 1 provides the same
estimates of ±PV (when X= 1 and X= 0, respectively)
that can be obtained directly from Table 2 by calculating the appropriate proportions (e.g., +PV of DVD
= exp (-1.3391 + 1*2.2146)/(1 + exp (-1.3391 +
1*2.2146)) = 0.7059, which is also calculable direcdy
from Table 2 as 12/17). In contrast, logistic regression
7. Prediction Error Estimates for
Multivariate Logistic Regression Models
TABLE
Prediction Error
ISS Components
(preferred eye)
MSP
MSP,
MSP,
MSP,
MSP,
MSP,
DVD
MOKN
MSB
DVD, MOKN
DVD, MOKN, MSB
Total
Negative
Positive
0.1552
0.1524
0.1606
0.1707
0.1518
0.1544
0.4449
0.4372
0.4539
0.4987
0.4331
0.4395
0.0587
0.0574
0.0628
0.0614
0.0580
0.0594
ISS = infantile squint syndrome; MSP = monocular smooth
pursuit; DVD = dissociated vertical deviation; MOKN =
monocular optokinetic nystagmus; MSB = monocular speed bias.
provides a more powerful way to assess the predictive
power of the continuous ISS measurements. By substituting the estimates of a and b and a set of values for X
in equation 1, we can estimate Pr[D\ x] as a continuous
function of X.
Figure 5A displays these estimated Pr[D\x] functions, along with the shaded 95% pointwise confidence intervals, for the continuous ISS component
measurements in the preferred eyes of EOE and LOE
populations. Figure 5B shows the corresponding function estimates for the nonpreferred eyes. Horizontal
axes represent the directional bias of the three measures; the vertical axes represent the estimated probability of EOE given the direction bias. Note that ISS
ratios below 0.5 are considered equal to 0.5 for MOKN
and MSP, and values greater than 0.5 are considered
equal to 0.5 for MSB (see Appendix B). Figures 5A
and 5B clearly illustrate that the risk of EOE increases
with the amount of nasal bias in MOKN and MSP in
preferred and nonpreferred eyes. The evidence for
an association between MSB and EOE is much weaker,
as indicated by the very broad confidence intervals.
Horizontal dotted lines in Figure 5 represent the
baseline prevalence of EOE in CACS. The distance of
the estimated Pr[£)|x] function from this horizontal
line suggests the prognostic usefulness of the measurement in this population. Vertical dashed lines represent the diagnostic cutoffs used in the dichotomous
analysis. The sharp increase in risk beyond this cutoff,
particularly for MSP in preferred eye, illustrates the
predictive information that was not captured by the
dichotomous analysis.
Rows of small vertical lines represent individual
ISS measurements in the EOE and LOE groups. These
data facilitate the interpretation of the Pr[D\ x] functions estimated using the logistic model. For example,
the EOE data for MSP ratios in the preferred eye are
more concentrated over regions of nasal asymmetries
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
731
Retrospective Prediction of Early-Onset Esotropia
TABLE 8.
Monocular Optokinetic Nystagmus Asymmetry in Preferred
Eyes of Accommodative and Nonaccommodative EOE and LOE
Nonaccommodative ET
Accommodative ET
EOE
LOE
N
Median
IQR
N
Median
IQR
7
25
0.54
0.54
0.53-0.60
0.47-0.59
43
125
0.66
0.54
0.58-0.72
0.49-0.61
EOE = early-onset esotropia; LOE = late-onset esotropia; ET = esotropia; IQR = interquartile
range.
than are the LOE data; this corresponds to the strong
association of EOE with higher nasal MSP asymmetries. In contrast, the distributions of both MOKN and
MSB measurements were more similar among EOE
and LOE subjects. The paucity of MSB observations
0.3
A
I
I Illllllll IBll| I Mill I I III II I I
0.4
0.S
0.6
0.7
0.8
II
Illl III III II II I Mil II II I I
I I III
I
0.9
MOKN
i
B
< 0.4 suggests that the support for the apparent association of MSB with EOE is weak (also reflected in the
very wide confidence intervals for this component).
It is essential to note that the estimates displayed
in Figure 5 assume that the baseline prevalence of
MOKN
i
mi iIUIIIIIIIIIIIIIIira i
i n
i
i
MSP
FIGURE 5. Univariate logistic model estimates of Pr[Z)|a;] for the continuous measures of
three infantile squint syndrome components (monocular optokinetic nystagmus, monocular
smooth pursuit, and monocular speed bias), assuming baseline early-onset esotropia prevalence of 0.25. Plots are for preferred eyes (A) and nonpreferred eyes (B). Horizontal axes
represent the directional bias of the three infantile squint syndrome measures; vertical axes
represent the estimated probability of early-onset esotropia, conditional on the infantile
squint syndrome measurement, (vertical dashed lines) Diagnostic cutoffs used in the dichotomous analysis, (small vertical lines) Individual infantile squint syndrome measurements in
the groups with early-onset esotropia (top) and late-onset esotropia (bottom), (horizontal dotted
lines) Baseline prevalence of early-onset esotropia in our sample.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
MSB
732
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
squared difference between diat estimate and 1 (if the
subject had EOE) or 0 (if the subject had LOE).
We estimated such prediction errors from the
Q_
CACS
data by using a resampling technique called
CO §
tenfold cross-validation (see Appendix C). Table 5
presents the mean prediction error results for each
LJJ
of seven univariate logistic regression models. Total
O <P
prediction error (TPE) represents die estimated prediction error for an adult with strabismus drawn at
Q_
random from the CACS sampling population. Because
TJ
CD
TPE essentially weights die prediction errors for subco
jects with EOE and LOE according to the relative prevE
alence of EOE and LOE, TPE reflects, in part, the
</)
CACS baseline EOE prevalence. Therefore, Table 5
LJJ
also reports estimates of prediction error averaged
separately among die 50 subjects with EOE and dien
among die 150 subjects with LOE, which we term
"negative" and "positive" prediction errors (—PE
0.0
0.2
0.4
0.6
0.8
1.0
and +PE), respectively. Partitioning the prediction erEOE Prevalence
ror into ±PE provides some insight into how die ISS
FIGURE 6. Estimates of Pr[D\ x] for four values of monocular components might perform in odier populations of
smooth pursuit are plotted as a function of the baseline
adults witii strabismus with different baseline prevaprevalence of early-onset esotropia. The diagonal line reprelences of EOE. Additionally, diis allows model evaluasents Pr[D\x] equal to baseline prevalence.
tion to reflect the differential consequences of misclassifying subjects widi EOE or LOE. For example, a patient with LOE might not be treated if he or she were
EOE among the target population of adult subjects
misclassified
as having EOE, which typically has a
with strabismus is 0.25. The estimated conditional
lower
prognosis
for functional correction than LOE.
probabilities of EOE in an adult population with strabismus with an EOE baseline prevalence other than
As with our earlier analyses, it is instructive to
0.25 would differ. Figure 6 displays the estimated
compare the performance of prediction rules based
Pr[D\ MSP] for various prevalences of EOE. For refer- on ISS measurements to a simple rule based solely on
ence, the light continuous line at 45° represents the
the baseline prevalence. Because the EOE baseline
predicted Pr[E0E\ based solely on baseline prevaprevalence in CACS was 0.25, if we had not considered
lence. For example, an MSP bias of 0.60 elevates the
the ISS measurements, we would have concluded that
probability of EOE very little above any baseline prevathere was a probability of 0.25 that any individual samlence. In contrast, if there was a dramatic asymmetry
pled from the CACS data base would have an EOE.
of MSP = 0.80 (the bold series of long and short
Baseline TPE and ±PE for such a prediction rule,
dashes), the probability of EOE would be very high at
without consideration of ISS components, are calcuany baseline prevalence. The bold continuous line in
lated as follows:
Figure 6 for an MSP ratio of 0.5 indicates that if MSP
is symmetric (i.e., there is no bias), the probability
Baseline - PE = (1 - 0.25)2 = 0.5625
(2)
that a patient has EOE is less than the baseline pre2
(3)
Baseline + PE = (0 - 0.25) = 0.0625
dictive value.
••—>
*-t—>
Univariate Model Selection Based on Prediction Error.
Several of the ISS components appear associated with
EOE when considered as univariate predictors in logistic regression models. How can we choose among
them? One of our primary objectives is to assess how
the ISS components might facilitate clinical assessment of the age of strabismic onset. Thus, a natural
way to appraise the clinical usefulness of the ISS components is to estimate the prediction error that would
result if we actually used the ISS measurements,
through logistic regression, to estimate die probability
that subjects had EOE. As described in Appendix C,
we quandfy die prediction error for a subject as the
Baseline TPE = [50 X (-PE) + 150
X (+PE)]/200 =0.1875
(4)
These baseline prediction errors help us assess the
performance of the prediction models based on the
ISS components.
The TPE column in Table 5 indicates diat prediction errors were smaller for models using ISS components in preferred eyes than for models using nonpreferred eyes. The prediction error was not significantiy
reduced by using MSB in either eye (0.1814 and
0.1871, preferred eyes and nonpreferred eyes, respec-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
733
Retrospective Prediction of Early-Onset Esotropia
tively, versus baseline TPE of 0.1875) or MSP in the
nonpreferred eye (0.1827). Table 5 shows, however,
that a prediction model based solely on MSP asymmetry in the preferred eye had the lowest average TPE of
all ISS components (0.1552), which is a 17% reduction
from the baseline TPE. The next smallest TPE was for
MOKN in the preferred eye (0.1689). This contrasts
the results of the dichotomous analysis, which suggested that MOKN was the only continuous ISS component associated with EOE.
Because MSP in the preferred eye had the smallest
+PE and — PE, it is likely to have the smallest TPE
even in populations with different EOE prevalences.
In a population with a relatively low prevalence of
EOE, the +PE displayed in Table 5 would be weighted
more heavily; thus, the TPE for DVD should be
smaller. Finally, our estimated TPE assumes that negative and positive prediction errors bear equal costs;
for example, if the consequences of a false negative
are substantially less than of a false positive, Table 5
suggests that DVD may be more useful than MOKN.
Multivariate Logistic Regression Analyses
Multivariate Logistic Regression Estimates. Our univariate analyses suggested that MSP in the preferred
eye is the single best ISS predictor of EOE among
adult subjects with strabismus. We fit a series of multivariate models with additional ISS variables to determine whether the prediction of EOE could be improved by using other ISS components in conjunction
with MSP asymmetry in the preferred eye. Table 6
presents four models, starting with the univariate
model based on MSP nasal asymmetry alone and successively adding DVD, MOKN, and MSB (the latter
two measures were for preferred eyes). Adding DVD
to the univariate MSP model resulted in a statistically
significant improvement in model fit (P = 0.02); the
b parameter estimates for both these ISS components
remained large, which indicates independent and substantial associations with EOE. Adding MOKN to this
bivariate model (yielding model 3) produced no significant improvement in fit (P = 0.14) but did reduce
the strength of association between MSP and EOE
resulting from partial colinearity of MOKN and MSP.
Finally, adding MSB to the model produced no significant improvement in fit (P = 0.90) and had little
effect on the other parameter estimates. Thus, although MOKN and MSB showed substantial and statistically significant associations with EOE when considered univariately, these associations virtually disappeared when we controlled for MSP and DVD by their
inclusion in the model.
Prediction Error Estimates for Multivariate Logistic Re-
gression Models. Table 7 presents the estimated prediction errors for six multivariate models. Using a model
with DVD and MSP (preferred eye) reduces the TPE
Q
Q_
CO
LU
o
LU
CL 6
•D
CD
E "
c/)
LU
p
d
0.4
0.5
0.6
0.7
0.8
MSP (preferred)
FIGURE 7.
Estimates of Pr[D\ x] based on monocular smooth
pursuit (MSP) for subjects with (solid line) and without (dotted line) dissociated vertical deviation (DVD). Clearly, including the DVD test results improves the predictive usefulness
of MSP measurements for a wide range of continuous measures of MSP bias.
by 0.0028, or only an additional 2%. Adding MOKN
or MSB (preferred eyes) to the MSP model actually
worsened predictions slightly; adding MOKN to a
model including both MSP and DVD reduced the TPE
by 0.0006, or only an additional 0.4%. These results
suggest that it is useful to consider MSP in the preferred eye and in DVD but that adding the other ISS
variables provides little additional information in predicting EOE among adult subjects with strabismus.
Although the predictive power added by these laboratory measurements appears small, knowing their magnitude in a given adult patient may substantially reduce uncertainty about the age of onset in certain
circumstances. For example, knowing a patient has an
extreme pursuit asymmetry raises the probability that
of EOE substantially above the baseline prevalence,
whereas moderate values of MSP asymmetry provide
marginal support for EOE above the baseline prevalence (see Fig. 6).
Estimates of the Probability of Early-Onset Esotropia
as a Function of Monocular Smooth Pursuit Bias, With and
Without Dissociated Vertical Deviation. Figure 7 displays
the estimated probability of EOE based on the presence of MSP with and without DVD (Pr[EOE\ MSP,
DVD]), assuming a 0.25 baseline prevalence of EOE.
The vertical (dashed) line indicates the cutoff criterion (0.558) used in our dichotomous analysis of MSP
asymmetry. The separation between the piecewise linear logistic functions in Figure 7 (see Appendix B)
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
734
Investigative Ophthalmology 8c Visual Science, March 1997, Vol. 38, No. 3
illustrates the improved predictive power of MSP when
it is considered along with DVD. The probability of
EOE, based on measures of DVD and MSP asymmetry,
in an adult with strabismus selected at random from
a population with a 0.25 baseline prevalence of EOE,
could be estimated from this plot. The probability of
EOE for a patient with DVD and MSP asymmetry, sampled from another population or clinic with a different baseline prevalence for EOE, would differ from
that seen in Figure 7.
DISCUSSION
Dichotomous Analyses
Dichotomous analysis illustrates that early- and lateonset groups exhibited clinical signs of ISS, indicating
that the syndrome components are not exclusively associated with EOE. Consequently, a prediction of EOE
can only be made with a limited degree of certainty
when a subject has one or more ISS components. To
ascertain whether the ISS components could be used
as predictors of EOE, we analyzed these components
in terms of their sensitivity, specificity, and ±PV.
Although MOKN, MSP, and MSB had higher sensitivities to EOE, they had substantially lower specificities than did DVD (Table 3). Of all ISS components,
DVD had the highest +PV. However, the prevalence
of DVD is generally low, and, thus, it has low sensitivity,
which diminishes its clinical usefulness in predicting
EOE. We estimated the +PV of MOKN to be somewhat higher than the baseline prevalence of EOE, indicating that MOKN increased the likelihood of a correct prediction of EOE only slightly above chance.
The dichotomized versions of MSP and MSB had even
lower +PV than did MOKN. None of the -PV for
the ISS components were significantly different from
chance (baseline prevalence), indicating that they
were of little additional value for diagnosing LOE. The
only ISS component that was relatively uncommon in
EOE and LOE (0.18 and 0.20, respectively) was LN;
it has a higher prevalence in preadolescence and may
be an excellent predictor of EOE in younger popula36
tions.
Our predictive value analyses focused on unilaterally defined failure criteria—i.e., where the preferred
and nonpreferred eyes are evaluated separately with
respect to the cutoff. An alternative diagnostic strategy
would classify subjects as having EOE only if they fail
the criterion for a given ISS component in preferred
and nonpreferred eyes. Table 3 indicates that, as expected, for such a bilateral diagnostic rule, sensitivity
declines and specificity increases relative to the performance of unilaterally defined criteria because abnormal values were less prevalent in the "both" than in
the preferred or nonpreferred eye categories. In set-
tings in which false-positive results are much more
costly, this suggests that bilateral failure criteria for
MOKN, MSP, and MSB may be appropriate.
Logistic Regression Analysis
Logistic regression analysis provided a more powerful
technique for exploring the association between
MOKN, MSP, and MSB and EOE than did the dichotomous analysis of these ISS components. We found that
MOKN and MSP nasal asymmetries, as well as MSB
temporal asymmetries, all revealed an association with
EOE. Logistic regression enabled us to estimate the
probability of EOE given the magnitude of individual
ISS components. Admittedly this is clinically attractive,
but these estimates are sensitive to the baseline prevalence of EOE in any given population.
Our prediction error analysis of continuous measurements of ISS components revealed that MSP in
the preferred eye was the single strongest predictor
of EOE, in contrast to the dichotomous analysis that
relied on a diagnostic cutoff based upon the 95th percentile of the control population. Because logistic regression analysis can use continuous measures and
does not depend on a cutoff, it revealed the importance of MSP in predicting EOE. This suggests that
if MSP is measured clinically by direct observation,
considerable care is needed to establish a cutoff.
The ±PE columns in Table 5 indicated that a
logistic prediction model based solely on MSP in the
preferred eye had the smallest — PE and +PE among
the seven univariate models. Accordingly, MSP is likely
to have the smallest TPE, even in populations with
different EOE baseline prevalence. Again, TPE measures the average (squared) difference between the
probability of EOE estimated by the logistic regression
model and the actual diagnosis from the case history
(EOE or LOE) (see Appendix C). Our estimated TPE
assumes that +PE and — PE bear equal costs, which
may be incorrect. Treatment might be more aggressive
for a patient with a high rather than a low prognosis.
Consequently, a patient with LOE who is classified
incorrectly as having EOE might undergo a less effective treatment regimen, which could reduce the prognosis for functional correction of strabismus. However, the reverse error would enhance the initial treatment effort by overestimating the prognosis.
The dichotomous analysis suggested that among
MOKN, MSP and MSB, MOKN was the best indicator
of EOE. Dichotomizing the ISS data at the 95th percentile of normal subjects' measurements led to a loss
of information; however, these cutoffs may not have
been optimal, and this approach treated all measures
of ISS above the cutoff as equal. Subsequent logistic
regression analyses using continuous measures of
MOKN, MSP, and MSB revealed that MSP (preferred
eye) was the strongest single predictor of EOE.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
Retrospective Prediction of Early-Onset Esotropia
Logistic regression also facilitated a multivariate
analysis to determine whether any of the ISS components considered jointly provided independent predictive information. Both dichotomous and logistic
analyses agreed that DVD is a useful indicator of EOE.
Because of the low overall prevalence of DVD, testing
for this alone would have been of limited value. That
is, although most persons who had DVD had EOE
(thus yielding a high +PV), relatively few subjects had
DVD. We found that DVD and MSP (preferred eyes)
were the best set of two predictors. Adding MSB,
MOKN, or both to this model produced neither a
significantly better fit to the data nor a reduction in
prediction error.
Generalizability of Results. Several factors could
limit the generalizability of our results to other populations. Most of our subjects were adults with relatively
long histories of strabismus, most had a history of amblyopia, and all had undergone treatment for strabismus that may have modified their ISS components.
Clearly, our results are not generalizable to the problem of determining whether the age of onset was early
or late among children younger than 8 with strabismus.
However, our results should apply to subjects with strabismus who range from 8 to 40 years of age, have a
history of amblyopia, and seek functional correction
for strabismus. Other factors that might limit the generalizability of our results include potential misclassification, recall and selection biases, and measurement
error.
Possible misclassification of our subjects as having
EOE or LOE could bias estimates of the association
between ISS components and age of onset. Our subjects with strabismus (age range, 8 to 40 years) were
classified largely on the basis of their recollection of
the age of onset, earliest treatment, or both. Consequently, our determination of age of onset is subject
to error. If subjects were misclassified randomly, this
would generally attenuate the relationship between
the age of onset and the ISS components. It is more
likely, however, that subjects who did have EOE would
be misclassified as having LOE than the converse (for
example, if there was no recollection of the age of
onset in a subject with EOE for whom treatment occurred after the first birthday, our study would classify
this subject mistakenly as having LOE). If this misclassification was independent of ISS status at the time of
our study, this again would attenuate our estimate of
the b parameter in equation 1 and would bias our
+PV and —PV estimates down and up, respectively. If,
however, the probability of misclassification differed
according to ISS status, the potential biases could be
in either direction.
In addition, there is the issue of potential selection bias. We have discussed how the +PV, — PV, and
conditional probability estimates are all dependent on
735
the baseline prevalence of EOE in the target population. If this baseline prevalence is known, and it is
assumed that our sensitivity and specificity estimates
are unbiased, we could extend our results to other
populations as shown in Figures 3 and 6.
Finally, the ISS measurements themselves are subject to error. However, because our objective is to
evaluate the clinical usefulness of the ISS components
as measured in practice, the same error is inherent in
any clinical evaluation of ISS. A separate issue, of
course, is whether a more precise measure of MSB,
for example, might show a stronger association with
EOE; alternatively, less precise measurements of MSP
would be less predictive of EOE.
Earlier Studies and Relevance to the Current Investiga-
tion. Monocular Optokinetic Nystagmus. Figure 1 con-
firms earlier studies by Bourron-Madignier et al,18
Demer and von Noorden,19 and Mein,7 which reported that the slow phase of MOKN and MSP were
faster, on the average, for the EOE and the LOE in
response to nasal motion. These studies also indicated
that the MOKN and MSP ratios were larger for the
early-onset than for the late-onset group. Differences
between +PV of MOKN observed in our study sample
and in earlier studies by Bourron-Madignier et al18
and Demer and von Noorden19 result in large part
from differences in the clinical baseline prevalence of
EOE (Fig. 3). Other potential factors include differences in cutoff selection as well as possible differences
in population age, treatment history, and association
with amblyopia. In addition, part of the discrepancy
between the +PV measures in our study and the studies of Bourron-Madignier et al18 and Demer and von
Noorden19 may have been caused by differences in
stimulus parameters.
Bourron-Madignier et al18 and Demer and von
Noorden19 stimulated MOKN with a standard handheld OKN drum. The velocity (9°/second) and the
field size (13°) used in our study are consistent with
the use of the standard handheld OKN drum (20 cm
diameter) held a distance of 87 cm from the patient
and rotated approximately 13 times/minute. Bourron-Madignier et al18 used a slower stimulus velocity
(5.5°/second) and a larger field (22.6°) with a 20 cm
drum held 50 cm from the patient and rotated 13
times/minute. Demer and von Noorden19 used a
larger field size (37°) and a higher stimulus velocity
(38°/second) with a 20 cm drum held 30 cm from
the patient and rotated 20 rpm. Variations in these
stimulus parameters could either increase or decrease
the +PV, depending on the severity of MOKN asymmetries in the patient population under evaluation.
The +PV of asymmetric MOKN also is influenced
by an interaction between characteristics of the test
stimulus and the slow phase velocity of OKN. Increasing stimulus velocity reduces slow phase gain for
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
736
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
MOKN both nasally and temporally.3738 In addition,
asymmetric MOKN varies with the spatio-temporal parameters of die stimulus during infancy.39'40 In strabismus and amblyopia, the nasal asymmetry of MOKN
increases with stimulus velocity14 up to a limit when
MOKN fails to respond to higher stimulus velocities
in either the nasal or the temporal direction (at which
point the N:T ratio equals 1.0). The upper velocity
limit that exhibits asymmetric MOKN and die optimal
stimulus velocity for revealing asymmetric MOKN will
vary between subjects, depending on die severity of
their MOKN disorder. Increasing stimulus velocity will
enhance the asymmetry in some subjects and reduce
it in others. In the extreme, at very high stimulus velocities, asymmetric MOKN might become more apparent in the late-onset group dian in the early onset
group if the stimulus exceeds the response range of
the early onset group. The result of very high stimulus
velocity would be to decrease die +PV of die test.
Indeed, die stimulus velocity used in die current study
produced more bidirectional reduction of MOKN in
nonpreferred than preferred eyes and resulted in
greater +PV for MOKN in predicting EOE for die
preferred eye category. Finally, the upper velocity limit
for stimulating MOKN is influenced by field size37;
hence, lower stimulus velocities should be used to reveal MOKN asymmetries for small test fields (i.e., with
handheld OKN drums than for large, full-field stimulators) .
A Comparison of Monocular Optokinetic Nystagmus
in Accommodative and Nonaccommodative Strabismus. We
considered the possibility that two classes of strabismus
(accommodative and nonaccommodative) might contribute to differences in the prevalence of MOKN
asymmetries found in die EOE and LOE groups. Accommodative esotropia was classified on the basis of
an abnormally high AC/A ratio. Traditionally, diese
patients are classified as having nonrefractive accommodative esotropia33; however, we have no information concerning our adult subjects' refractive status
during infancy, so we hesitate to categorize it as either
refractive or nonrefractive. Current measures of refractive errors reveal that 6 of 7 subjects widi EOE and
18 of 25 subjects with LOE had greater than 1 D of
anisometropia. If hyperopia is defined as greater than
2 D of positive error in both eyes, one subject in the
EOE group and six subjects in die LOE group could
be categorized as having refractive accommodative esotropia. If hyperopia is defined as greater dian 2 D of
positive error in either die preferred or die nonpreferred eye at the time of participation in the CACS
study, three subjects in the EOE group and 12 subjects
in die LOE group could be categorized as having refractive accommodative esotropia.
Differences in etiology of accommodative and
nonaccommodative esotropia could result in different
characteristics of MOKN in these two classes of esotropia. Table 8 compares the median values of MOKN
asymmetry in die preferred eyes of accommodative
and nonaccommodative EOE and LOE. The 32 subjects with accommodative esotropia occurred with approximately equal prevalence in EOE and LOE (0.14
and 0.17, respectively); seven had EOE and 25 had
LOE. The median MOKN bias for subjects with accommodative esotropia was the same (0.54) for EOE and
LOE. In contrast, the median MOKN bias for subjects
with nonaccommodative esotropia was substantially
higher for EOE (0.66) than for LOE (0.54). These
results are in agreement with those of Aiello et al,41
who observed symmetrical MOKN in diree children
with accommodative esotropia. Caution is recommended in using MOKN to predict EOE in populations with a high prevalence of accommodative esotropia.
Monocular Smooth Pursuit. As mentioned, several
small population studies have documented MSP asymmetries in subjects with amblyopia, esotropia, or
both,9"11'23"25 but large population-based studies of
asymmetric pursuit and its prevalence in association
with EOE have yet to be conducted. Dichotomous
measures did not reveal a significant relationship between MSP asymmetry and EOE because of the difficulty in selecting an appropriate diagnostic cutoff.
Our logistic regression analysis, however, revealed a
strong relationship between MSP and EOE. The best
predictor of EOE was DVD in association with MSP
asymmetry in the preferred eye. These results suggest
that continuous objective measures, as opposed to dichotomous measures obtained from subjective observation of the patient's MSP, are recommended in a
clinical setting as the strongest indicator of EOE. The
continuous measures of MSP must be interpreted in
terms of the baseline prevalence of EOE in die clinical
population from which they are sampled. Figure 6
may be useful in different clinical populations by providing an estimate of EOE (contingent on the magnitude of the MSP asymmetry for different baseline prevalence).
Monocular Speed Bias. As was true for MSP, no large
population-based studies have been conducted to determine the association of MSB with EOE. In our
study, die psychophysical measures of MSB illustrate
diat subjects with strabismus perceived temporal target motion as faster than nasal target motion (see Fig.
1). These temporal velocity biases were larger for the
EOE group than for the LOE group, suggesting that
MSB might be included as a sensory component of
the ISS. The temporal MSB observed in die CACS
subjects widi esotropia followed the same direction as
reported in two recent studies. Hague et al26 observed
higher thresholds for motion detection in the nasal
than in the temporal direction in 5 of 7 subjects with
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
737
Retrospective Prediction of Early-Onset Esotropia
EOE. None of these subjects had LN or a history of
amblyopia. Brosnahan et al27 investigated MSB in 18
subjects with EOE and in 11 subjects with LOE with
a higher standard velocity (10°/second) than was used
in the current investigation (3°/second). Using diagnostic cutoff criteria similar to ours, they also observed
the same temporal MSB. Roberts and Westall28 found
no velocity bias in six subjects with strabismus and
amblyopia with unknown age of onset. Similarly, Hartmann et al20 used a motion-nulling paradigm and
found that velocity biases in four infants with esotropia
were small and mixed in direction or were nonexistent
in the presence of larger MOKN biases.
The temporal velocity biases reported here, as well
as those reported by Hague et al26 and Brosnahan et
al,27 are in the opposite direction to those reported
for two subjects by Tychsen and Lisberger." The conflicting reports regarding the direction of the velocity
bias could result from differences in the subjects examined, as well as from differences in the test stimulus
parameters. A minority of our subjects (n = 15) did
have the same directional velocity bias (nasal) as reported by Tychsen and Lisberger," but these were
uncommon compared with the number of subjects
with a temporal bias (n = 45) (7.6% nasal bias and
22.3% temporal bias). The stimulus velocity used by
Tychsen and Lisberger11 (13.5°/second to 16.5°/second) is equivalent to velocities used by Brosnahan et
al27 and Hartmann et al.29 Exposure durations and
psychometric procedures used by Tychsen and Lisberger11 were identical to those used in the current
study and by Brosnahan et al.27 An important difference between the study by Tychsen and Lisberger"
and those listed above is that Tychsen and Lisberger
used a single moving bar to test MSB, whereas all the
other studies used drifting gratings. Spatial parameters such as field size, number of bars, and spatial
frequency content might help to explain the differences.
The temporal velocity bias observed by us and by
Hague et al26 and Brosnahan et al27 could result from
an interaction between the asymmetric MOKN and
the drifting grating stimulus for testing velocity discrimination. Normally, perceived velocity is lower
when the eyes pursue the moving stimulus than when
fixation is held stationary, as observed in the AubertFleischel phenomenon.42"'14 Perhaps the moving grating stimulus for MSB engaged OKN during the motion test, and, when MOKN was biased, the viewing
eye followed the drifting grating at a higher velocity
when it moved in the dominant direction. The single
bar used by Tychsen and Lisberger" would be less
likely to engage OKN. Our study and that of Brosnahan et al27 used a fixation spot to suppress OKN. However, small, following eye movements might still have
occurred.
Clinical Relevance
It is usually difficult, if not impossible, to obtain any
documented information about age of onset of strabismus or amblyopia from an adult patient. The ISS components provide a way of estimating the probability
of EOE when the age of onset is unknown. Logistic
regression indicated that DVD, MSP, MOKN, and MSB
were useful in discriminating between early- and lateonset esotropia in adult subjects. This information
could be helpful in forming a prognosis for the functional correction of strabismus in adults when it is
associated with amblyopia.30 After correction of strabismus, well-maintained functional binocular alignment requires that disparity be sensed by the two eyes.
This is possible only if both eyes have adequate visual
acuity. Thus, the prognosis for functional correction
of strabismus hinges on the prognosis for correction
of amblyopia that may be associated with strabismus.
Worth45 demonstrated that when treatment is delayed
to adulthood, the prognosis for functional correction
of amblyopia is reduced drastically for patients with
EOE, whereas many patients with LOE achieved good
visual acuity. There are numerous current reports of
corrected amblyopia in adult patients.40"49 The age of
onset influences the prognosis for functional correction that, according to comparative studies,50'51 is attributable to plasticity of the adult visual cortex. Therefore, the association of the ISS with EOE provides a
means to assess age of onset from measures of sensory
and motor visual functions.
These measures can be used to form a prognosis
for functional correction of strabismus associated with
amblyopia in adults for whom there is no documentation of the age at which binocular vision was disrupted.
The prognosis is based on the assumption that EOE
is more difficult to treat than LOE. Probability estimates of EOE and LOE can be derived from current
measures of ISS components; however, the predictive
values of these measures must be tempered by the
baseline prevalence of EOE and LOE, perhaps obtained from the patient records of a given clinic. Baseline prevalence can vary as a result of many factors,
including the specialties of the practicing clinicians,
the age of patients, the socioeconomic structure of
the community served by the practice, and access to
and thoroughness of the health care available to the
population.
Key Words
motion perception, optokinetic nystagmus, pursuit eye
movements, statistics, strabismus
References
1. Costenbader FD. Infantile esotropia. Trans Am OphthalmolSoc. 1961;59:397-429.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
738
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
2. Ciancia A. La esotropia en la lactante diagnostico y
tratamiento. Arch Chilean Ophthalmol 1962;9:117. In
Spanish.
21.
3. Lang J. Squint dating from birth or with early onset.
Transactions of the First Internatinal Congress of Orthoptists. London: Kimpton; 1968:231-237.
4. Kommerell G. The pathophysiology of infantile strabismus. In: Kauffman H, ed. Trans Sixteenth Meeting
Eur Strabismol Assn. Giessen, Germany: European Strabis22.
mological Association 1987:47-53.
5. Nixon RB, Helveston EM, Miller K, Archer SM, Ellis
RD. Incidence of strabismus in neonates. AmJOphthal23.
mol 1985; 100:798-801.
6. Mein J. The OKN response and binocular vision in
early onset strabismus. Aust Orthoptf. 1983;20:13-l7.
24.
7. Mein J. The asymmetrical optokinetic response. Br
OrthoptJ. 1983;40:l-4.
8. Kommerell G. Ocular motor phenomena in infantile
25.
strabismus. In: Lennerstrand G, von Noorden GK,
Campos EC, eds. Strabismus and Amblyopia. London:
Macmillan Press; 1988:99-109.
26.
9. Schor CM. A directional impairment of eye movement
control in strabismus amblyopia. Invest Ophthalmol.
1975; 14:692-697.
10. Fukai S, Tsutsui J, Nakamura Y. Abnormal pursuit
movements of the fellow eye in amblyopia with strabismus. In: Moore S, Mein J, Stockbridge L, Stratton
27.
L, eds. Orthoptics: Past, Present and Future. New York:
Symposia Specialist Medical Books; 1976:75-91.
11. Tychsen L, Lisberger SG. Maldevelopment of visual
28.
motion processing in humans who had strabismus
with onset in infancy, f Neurosci. 1986;6:2495-2508.
12. Nicolai H. Differenzen zwischen optokinetischem
29.
Recht-und-Links-nystagmus bei einseitiger Schiel Amblyopie. Klin Mbl Augenheilk. 1959:134;245-250. In
German.
13. Loewer-Spieger DH. Amblyopie een studie over de
30.
kenmerken en de behandeling. / Ruysendaal Amsterdam. 1962; 52:107-119. In Dutch.
31.
14. Schor CM, Levi DM. Disturbances of small-field horizontal and vertical optokinetic nystagmus. Invest Ophthalmol Vis Sci. 1980; 19:668-683.
15. Flynn JT, Pritchard C, Lasley D. Binocular vision and
32.
OKN asymmetry in strabismic patients. Strabismus II
ISBN. Orlando: Grune & Stratton; 1984:35-43.
33.
16. Schor CM. Subcortical binocular suppression affects
the development of latent and optokinetic nystagmus.
Am f Optom Physiol Opt. 1983;60:481-502.
17. Tychsen L. Binocular vision. In: Hart WH, ed. Adler's
34.
Physiology of the Eye: Clinical Applications. St. Louis: CV
Mosby; 1992.
35.
18. Bourron-Madignier M, Ardoin ML, Cypres C, Vettard
S. Study of optokinetic nystagmus in children. In:
Lenk-Schafer M, ed. Transactions of the Sixth International Orthoptic Congress. Harrogate, UK: International
Orthoptic Congress; 1987:134-139.
36.
19. Demer JL, von Noorden GK. Optokinetic asymmetry
in esotorpia. J Ped Ophthalmol Strabismus. 1988; 25:286292.
20. Harcourt B, Mein J. Early onset esotropia In: van Balen ATM, Houtman WA. Strabismus Symposium CESSD, 37.
Docu Ophthal Proc Series, Vol 32. The Hague: Dr.
W.Junk. 1982:79-81.
Murray ADN, Calcutt C. The incidence of amblyopia
in longstanding untreated infantile esotropia. In:
Campos EC, ed. Strabismus and Ocular Motility Disorders:
Proceedings of the International Strabismological Assn. Surfers Paradise Basingstroke. London: Macmillan Press;
1990:45-50.
von Noorden GK. A reassessment of infantile esotropia: XLIV Edward Jackson Memorial Lecture. Am f
Ophthalmol. 1988; 105:1-10.
Tychsen L, Hurtig R, Scott W. Pursuit is impaired but
the vistibulo-ocular reflex is normal infantile strabismus. Arch Ophthalmol. 1985; 103:536-539.
Sokol G, Peli I, Moskowitz A, Reese, D. Pursuit eye
movements in late-onset esotropia. fPediatr Ophthalmol
Strabismus. 1991; 28:82-86.
Steinman SB, Levi DM, McKee SP. Discrimination of
time and velocity in the amblyopie visual system. Clin
Vis Sci. 1988;2:265-276.
Hague S, Shallo - Hoffman J, Fells P, Gresty M. Abnormal motion perception in early onset esotropia. In:
Lennerstrand G, ed. Update on Strabismus and Pediatric
Ophthalmology. ProcofthefointlSA and AAPO&'S meeting,
Vancouver, Canada June 19-23, 1994. London: CRC
Press; 1995; 106:109. Abstract.
Brosnahan D, Norcia AM, Schor CM, Taylor D. OKN,
VEP and perceptual directional biases in strabismus.
Vision Res. 1997; in press.
Roberts N, Westall CA. OKN asymmetries in amblyopia-their effect on velocity perception. Clin Vis Sci.
1990;5:383-389.
Hartmann EE, Succop A, Buck SL, Weiss AH, Teller
DY. Quantification of monocular optokinetic nystagmus asymmetries and motion perception with motionnulling techniques. OptSocAmA. 1993; 10:1835-1840.
Levi D. Pathophysiology of binocular vision and amblyopia. CurrOpin Ophthalmol. 1994; 5:1-10.
McKee SP, Schor CM, Steinman SB, et al. The classification of amblyopia on the basis of visual and oculomotor performance. Tr Am Ophthalmol Soc. 1992;
LXXXX:123-148.
Frandsen AD. Occurrence of squint. Ada Ophthalmol
ScandSuppl. 1960;62:33.
von Noorden GK. In: von Noorden, ed. Burian-von
Noorden's Binocular Vision and Ocular Motility—Theory
and Management for Strabismus. 3rd ed. St. Louis: CV
Mosby; 1985:168-416.
Bishop YMM, Fienberg SE, Holland PW. Discrete Multivariate Analysis. Cambridge: MIT Press; 1975:486-490.
Breslow NE, Day NE. Unconditional Logistic Regression for Large Strata. In: Statistical Methods in Cancer
Research. Vol. 1. The Analysis of Case-Control Studies.
Lyon: International Agency for Research in Cancer,
World Health Organization; 1980:192-246.
MacLellan AV. A further investigation into the problems of alternating sursumduction. In: Mein J, Bierlaagh JJM, Brummelkamp-Dons TEA, eds. Orthoptics.
Proceedings of the Second International Orthoptic Congress.
Amsterdam: Excerpta Medica; 1972:103-108.
Schor CM, Narayan V. The influence of field size upon
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
Retrospective Prediction of Early-Onset Esotropia
38.
39.
40.
41.
42.
43.
44.
739
the spatial frequency response of optokinetic nystagmus. Vision Res. 1981; 21:985-994.
Dichgans J. Optokinetic nystagmus as dependent on
the retinal periphery via the vestibular nucleus. In:
Baker R, Berthoz A, eds. Control of Gaze by Brain Stem
Neurons. Amsterdam: Elsevier; 1977:261-267.
Roy N, Lachapelle, P, Lepore F. Maturation of the
optokinetic nystagmus as a function of the speed of
stimulation in full term and preterm infants. Clin Vision Sci. 1989; 4:357-366.
Mohn G, Sireteanu R, van Hof-van Duin J. The relation of monocular optokinetic nystagmus to peripheral binocular interactions. Invest Ophthalmol Vis Sci.
1986; 27:565-573.
Aiello A, Wright KW, Borchert M. Independence of optokinetic nystagmus asymmetry and binocularity in infantile esotorpia. Arch Ophthalmol. 1994; 112:1580-1583.
Aubert H. Die Bewegungsempfindungen. Pflugers
Arch. 1986;39:347-370. In German.
Dichgans J, Wist E, Diener HC, Brandt T. The AubertFleischel phenomenon: A temporal frequency effect
on perceived velocity in afferent motion perception.
Exp Brain Res. 1975; 23:529-533.
Heidenreich SM, Turano KA. Speed perception and
APPENDIX A
Simple application of Bayes' Theorem demonstrates
that both +PV?md —PVdepend explicitly on the prevalence of the outcome in question.
Let EOE represent an early-onset of esotropia
(i.e., younger than 12 months), and let ISS represent
an abnormal value of the infantile squint syndrome
component under consideration. Then, the sensitivity
45.
46.
47.
48.
49.
50.
51.
eye movements. ARVO Abstracts. Invest Ophthalmol Vis
Sci. 1995;36:S356.
Worth CA, Squint: Its Causes, Pathology and Treatment.
Philadelphia: Blakiston; 1903.
Kupfer C. Treatment of amblyopia: Ex anopsia in
adults. Am J Ophthalmol. 1957;43:918-922.
Birnbaum MH, Koslbwe D, Sanet R. Success in amblyopia therapy as a function of age: A literature survey.
Am] Optom Physiol Opt. 1977;54:269-275.
Wick B, Wingard M, Cotter S, Scheimam M. Anisometropic amblyopia: Is the patient ever too old to treat?
Optom Vis Sci. 1992; 69:866-878.
Flom MC. Early experience in the development of
visual coordination. In: Young FA, Lindsley DB, eds.
Early Experience and Visual Information Processing in Perceptual and Reading Disorders. Washington, DC: National Academy of Sciences; 1970:2291-301.
Chino Y, Kaas JH, Smith EL, Langston AL, Cheng H.
Rapid reorganization of cortical maps in adult cats
allowing restricted deafferation in retina. Vision Res.
1992; 32:789-796.
Gilbert CD, Wiesel TN. Receptive field dynamics in
adult primary visual cortex in the cat. Nature. 1992;
336:150-152.
Assuming sensitivity and specificity estimates generalize beyond the study population, one can use these
formulas to estimate ±PVs for populations with other
prevalences of early-onset esotropia.
APPENDIX B
Below we describe how to choose a functional form
for the continuous infantile squint syndrome compoesotropia are defined as follows (where Pr[A \ B] is the nents.
probability of A given B):
Fitting logistic regression models using the continuous infantile squint syndrome components requires
choosing an appropriate scale. A simple linear model
Sens = Pr[ISS \ EOE]
of the association of these predictors with the log odds
Spec = Pr[not ISS \ not EOE]
(logit) of early-onset esotropia across the full range of
asymmetries (from temporal to symmetric to nasal)
If (f) represents the marginal, or baseline, preva- could lead to biased estimates. For example, suppose
lence of early-onset esotropia (i.e., (f> = Pr[early-onset esothat subjects with monocular optokinetic nystagmus
ratios of 0.3 and 0.4 are likely to be at equally low
tropia]), then by Bayes' Theorem
risk for early-onset esotropia, but that subjects with
monocular
optokinetic nystagmus ratios of 0.8 may be
+PV = Pr[EOE \ISS]
at substantially higher risk than those with ratios of
Pr[ISS | EOE] X Pr[EOE]
0.7. The linear logistic model applied in such a case
Pr[ISS]
falsely presumes that a unit difference in monocular
optokinetic nystagmus ratio implies the same differSens X </>
ence in logits in both cases.
[Sens X 4>] + [(1 - Spec) X (1 - 4>)
Therefore, we represent the continuous asymmetry data (monocular optokinetic nystagmus, monocuSimilarly
lar smooth pursuit, and monocular speed bias) using
piecewise linear functions. For example, the logistic
Spec X (1 — (/>)
regression parameter estimates for monocular optoki-PV=
netic nystagmus in the preferred eye assume that per[Spec X (1 - 4>)] + [(1 - Sens) X <f>]
and specificity of infantile squint syndrome for early-onset
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017
Investigative Ophthalmology & Visual Science, March 1997, Vol. 38, No. 3
740
sons with temporal monocular optokinetic nystagmus
biases (ratios < 0.5) are at the same risk for early-onset
esotropia. However, for those with nasal asymmetries
(ratios > 0.5), the logit of early-onset esotropia increases linearly with the magnitude of the asymmetry,
and the slope is estimated by .fitting the model using
maximum likelihood techniques.
This parsimonious representation was suggested
through the use of flexible nonparametric logistic regression techniques indicating that the piecewise linear function captured the essential relationship between monocular optokinetic nystagmus nasal biases
and risk for early-onset esotropia. Based on similar
reasoning and analogous nonparametric regression
results, the same piecewise linear transformations
were used for monocular optokinetic nystagmus in the
nonpreferred eyes and for monocular smooth pursuit
and monocular speed bias in preferred and nonpreferred eyes. However, temporal monocular speed biases appeared to be more strongly associated with
early-onset esotropia than for nasal biases; therefore,
temporal rather than nasal biases in monocular speed
bias represent the region of linearly increasing logits.
APPENDIX C
Estimating the prediction errors for various models
requires choosing a metric for prediction error and
choosing an estimation method.
Choosing A Prediction Error Metric
Consider the prediction error for a candidate
model with respect to a single subject with strabismus,
i, drawn from the same population as the Cooperative
Amblyopia Classification Study sample, whose age of
onset is known as early (2>, = 1) or late (A = 0). A
natural approach to assessing the model's predictive
usefulness is the following:
Measure subject i's infantile squint syndrome
component(s), %, denoting the actual value by
Estimate the probability that subject i had an early
onset given the measurement, Pr[D, \Xi = ^ ] , by
substituting % and the parameter estimates for a
and b from the candidate model into equation 1.
This is the model's "prediction" for i.
The model's prediction error, with respect to subject i, can then be quantified as {D\ — Pr[D, \ % =
*]). 2
For example, if subject i had an early onset (Dt =
1), the larger the estimated Pr[D\\Xk = x^], the smaller
the prediction error would be. Similarly, if D, = 0,
larger estimates of Pr[D{ \ X± = Xj] result in larger prediction errors. Using data from multiple subjects, we
could estimate the average prediction error for the
candidate model by averaging (D, — Pr[Dj|^ = Xj])2
for all subjects.
Estimating Prediction Error.
If sufficient data are available once a metric is
chosen, ideally one would fit the various candidate
models to a "learning" data set and then estimate the
prediction error for each model by applying it to a
new "test" data set. Instead, we use the following resampling technique known as tenfold cross-validation:
Divide the subjects randomly into 10 groups.
Exclude one group containing 10% of the data,
and fit the candidate models to the remaining
90% of the subjects.
Using parameter estimates obtained in the previous step, calculate the prediction error for die
excluded subjects.
Repeat the second and third steps 10 times, and
exclude another group of 10% of the subjects in
each iteration until each subject has served in a
test set.
Summarize the prediction error for each candidate model by die mean prediction error for all
200 subjects.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933197/ on 05/05/2017